Das könnte Ihnen auch gefallen
- Foot reflexology chart shows how hand acupressure points relate to body partsDokument3 SeitenFoot reflexology chart shows how hand acupressure points relate to body partsgautamlipika100% (2)
- Critical Care Notes Clinical Pocket Guide - (Gastro-Urinary)Dokument1 SeiteCritical Care Notes Clinical Pocket Guide - (Gastro-Urinary)Britanny Nelson100% (1)
- Rehabilitation in Guillian Barre SyndromeDokument6 SeitenRehabilitation in Guillian Barre Syndromeanon_681345291Noch keine Bewertungen
- Guillian Barré GBS Pediatrics in ReviewDokument10 SeitenGuillian Barré GBS Pediatrics in ReviewJohnnathan MolinaNoch keine Bewertungen
- Guillain-Barre Syndrome: Causes, Symptoms and TreatmentDokument8 SeitenGuillain-Barre Syndrome: Causes, Symptoms and TreatmentyasiraNoch keine Bewertungen
- Fish & Shellfish PoisoningDokument29 SeitenFish & Shellfish Poisoningkolita kamal100% (4)
- Guillain Barre SyndromeDokument16 SeitenGuillain Barre SyndromeNeha Rathore100% (1)
- GBSDokument21 SeitenGBSCherr NollNoch keine Bewertungen
- Pre-Test Maternal and Child Health NursingDokument18 SeitenPre-Test Maternal and Child Health NursingDefensor Pison GringgoNoch keine Bewertungen
- Guillan Barre Syndrome FinalDokument16 SeitenGuillan Barre Syndrome FinalAswathy RCNoch keine Bewertungen
- Guillain-Barré Syndrome (GBS)Dokument17 SeitenGuillain-Barré Syndrome (GBS)Desima Tamara sinuratNoch keine Bewertungen
- Tinetti PDFDokument2 SeitenTinetti PDFKenn yahweexNoch keine Bewertungen
- Communicablediseaseqa 140829080936 Phpapp02Dokument20 SeitenCommunicablediseaseqa 140829080936 Phpapp02Keiarah Kath Estrada CallaoNoch keine Bewertungen
- Guillaine Barre SyndromDokument15 SeitenGuillaine Barre Syndromirma ervinaNoch keine Bewertungen
- Guillain-Barre Syndrome: Practice EssentialsDokument18 SeitenGuillain-Barre Syndrome: Practice EssentialsAna-Maria DuMiNoch keine Bewertungen
- Overview of Guillain-Barré Syndrome: I. Literature ReviewDokument10 SeitenOverview of Guillain-Barré Syndrome: I. Literature ReviewS Dian RNoch keine Bewertungen
- Gullain-Barre SyndromeDokument7 SeitenGullain-Barre Syndromejanellekate1224Noch keine Bewertungen
- GUILLAIN-BARRE SYNDROME (1)Dokument42 SeitenGUILLAIN-BARRE SYNDROME (1)suraj rajpurohitNoch keine Bewertungen
- Guillain-Barré Syndrome Autoimmune Attack Peripheral NervesDokument5 SeitenGuillain-Barré Syndrome Autoimmune Attack Peripheral Nervesavinash dhameriyaNoch keine Bewertungen
- Dampd 5 Manual Del Jugador EspDokument24 SeitenDampd 5 Manual Del Jugador EspClaudio ReichelNoch keine Bewertungen
- Guillain Barre SyndromeDokument18 SeitenGuillain Barre SyndromeRendy AndikaNoch keine Bewertungen
- Guillain-Barré Syndrome Diagnosis and Clinical ManifestationsDokument27 SeitenGuillain-Barré Syndrome Diagnosis and Clinical ManifestationsEssaAyazNoch keine Bewertungen
- Guillain Barre SyndromeDokument6 SeitenGuillain Barre SyndromeErtania NirmalaNoch keine Bewertungen
- Script For PresentDokument3 SeitenScript For PresentTanya HoNoch keine Bewertungen
- Acute Flaccid Paralysis: A Review of Guillain-Barré Syndrome (GBSDokument33 SeitenAcute Flaccid Paralysis: A Review of Guillain-Barré Syndrome (GBSNor Ubudiah SetiNoch keine Bewertungen
- Guillain-Barré Syndrome Med Student PresentationDokument16 SeitenGuillain-Barré Syndrome Med Student PresentationRon ShenkarNoch keine Bewertungen
- Siti Wahyuni Maharani.S.Ked Asrianti S.Ked Pembimbing: Dr. Andi Weri Sompa, SP.SDokument8 SeitenSiti Wahyuni Maharani.S.Ked Asrianti S.Ked Pembimbing: Dr. Andi Weri Sompa, SP.SwahyuniNoch keine Bewertungen
- Capstone ProjectDokument4 SeitenCapstone Projectapi-662708357Noch keine Bewertungen
- Guillain Barre Syndrome: Molebatsi TheletsaneDokument16 SeitenGuillain Barre Syndrome: Molebatsi TheletsaneSri KombongNoch keine Bewertungen
- Gullian Barry SyndromeDokument19 SeitenGullian Barry SyndromeSayeeda AreebaNoch keine Bewertungen
- Gbs HarshaDokument34 SeitenGbs HarsharobyanaoktvNoch keine Bewertungen
- Jurnal GBSDokument16 SeitenJurnal GBSdzakiyahNoch keine Bewertungen
- Guillain-Barre Syndrome: Practice EssentialsDokument16 SeitenGuillain-Barre Syndrome: Practice EssentialsUKMBasketNoch keine Bewertungen
- Guillain BarreDokument17 SeitenGuillain Barrerk_s7Noch keine Bewertungen
- GBS: Overview of Guillain-Barré SyndromeDokument3 SeitenGBS: Overview of Guillain-Barré SyndromeclaudiaNoch keine Bewertungen
- Guillain-Barré Syndrome in Adults - Clinical Features and DiagnosisDokument14 SeitenGuillain-Barré Syndrome in Adults - Clinical Features and DiagnosisElsyAlegríaNoch keine Bewertungen
- Guillain Barre SyndromeDokument38 SeitenGuillain Barre SyndromePeterson Wachira HscNoch keine Bewertungen
- Understanding Guillain-Barré Syndrome and Myasthenia GravisDokument31 SeitenUnderstanding Guillain-Barré Syndrome and Myasthenia GravisTheresia Avila KurniaNoch keine Bewertungen
- Guillain-Barré Syndrome ExplainedDokument12 SeitenGuillain-Barré Syndrome ExplainedSoraya Dwi KhairunnisaNoch keine Bewertungen
- Guillain Barre SyndromeDokument13 SeitenGuillain Barre SyndromeAdreiTheTripleANoch keine Bewertungen
- Guillain Barre SyndromDokument10 SeitenGuillain Barre SyndromMiirnaawatii YalidaaNoch keine Bewertungen
- Guillain-Barre Syndrome GuideDokument13 SeitenGuillain-Barre Syndrome GuideUzra ShujaatNoch keine Bewertungen
- Askep Pasien Yang Mengalami Guillain-Barré Syndrome: Maridi M. DirdjoDokument14 SeitenAskep Pasien Yang Mengalami Guillain-Barré Syndrome: Maridi M. DirdjoPalupi Setyo HapsariNoch keine Bewertungen
- The Efficacy of Intravenous Immunoglobulin in Guillain-Barré Syndrome: The Experience of A Tertiary Medical CenterDokument7 SeitenThe Efficacy of Intravenous Immunoglobulin in Guillain-Barré Syndrome: The Experience of A Tertiary Medical CenterHadana RetnopratiwiNoch keine Bewertungen
- Differentiating Familial and Guillain-Barré NeuropathiesDokument22 SeitenDifferentiating Familial and Guillain-Barré NeuropathiesKartika IwangNoch keine Bewertungen
- Guillain Barre Syndrome and Its VariantsDokument12 SeitenGuillain Barre Syndrome and Its VariantsShauki AliNoch keine Bewertungen
- Guil LianDokument18 SeitenGuil LianPdianghunNoch keine Bewertungen
- Intensive Care Management of Guillain Barre Syndrome: A Retrospective Outcome Study and Review of LiteratureDokument10 SeitenIntensive Care Management of Guillain Barre Syndrome: A Retrospective Outcome Study and Review of LiteratureFakhrur RaziNoch keine Bewertungen
- Aan ?event Print&disorder - Id 935: TreatmentDokument3 SeitenAan ?event Print&disorder - Id 935: TreatmentclaudiaNoch keine Bewertungen
- GB SyndromeDokument17 SeitenGB Syndromehajra StudentNoch keine Bewertungen
- GBS1Dokument20 SeitenGBS1Yenza FaheraNoch keine Bewertungen
- Manejo Del SGB 10 PasosDokument13 SeitenManejo Del SGB 10 PasosRonald ReyesNoch keine Bewertungen
- Guillain-Barré Syndrome (GBS) : Prepared by Dr. Madiha Anees PT Asst. Prof/VP RCRS MS-PT, BS-PTDokument26 SeitenGuillain-Barré Syndrome (GBS) : Prepared by Dr. Madiha Anees PT Asst. Prof/VP RCRS MS-PT, BS-PTaneelala kanwal kanwalNoch keine Bewertungen
- Treatment: Guillain-Barré Syndrome (GBS) (Dokument15 SeitenTreatment: Guillain-Barré Syndrome (GBS) (akku_m1991Noch keine Bewertungen
- 2021_Neuromuscular Disorders in the Intensive Care UnitDokument21 Seiten2021_Neuromuscular Disorders in the Intensive Care UnitOlga Manco GuzmánNoch keine Bewertungen
- Consensus: StatementDokument13 SeitenConsensus: StatementElfrida FernandesNoch keine Bewertungen
- GBSDokument37 SeitenGBSmirabel IvanaliNoch keine Bewertungen
- Emergency Medicine EducationGuillain-Barré Syndrome - Third Time's The Charm - EmDOCs - Net - Emergency Medicine EducationDokument14 SeitenEmergency Medicine EducationGuillain-Barré Syndrome - Third Time's The Charm - EmDOCs - Net - Emergency Medicine EducationPgmee KimsNoch keine Bewertungen
- Guillain-Barré Syndrome Pediatrico 2018Dokument4 SeitenGuillain-Barré Syndrome Pediatrico 2018Mariam Plata100% (1)
- cprl1 0708Dokument3 Seitencprl1 0708adlbrlnNoch keine Bewertungen
- What Is GuillainDokument4 SeitenWhat Is GuillainHelda SeptivanyNoch keine Bewertungen
- 4 - Gullian Barr SyndromeDokument12 Seiten4 - Gullian Barr SyndromeHADI BADWANNoch keine Bewertungen
- Guillain-Barré Syndrome Literature OverviewDokument4 SeitenGuillain-Barré Syndrome Literature OverviewArlentinaNoch keine Bewertungen
- Guillain-Barré SyndromeDokument21 SeitenGuillain-Barré SyndromeZulkarnainBustamamNoch keine Bewertungen
- Jurnal GBSDokument26 SeitenJurnal GBSfajar sugandaNoch keine Bewertungen
- Nclex-Gi 2Dokument1 SeiteNclex-Gi 2Kenn yahweexNoch keine Bewertungen
- 69443164Dokument78 Seiten69443164Kenn yahweexNoch keine Bewertungen
- Freshmen Students Bank Procedures For Non-ATM Accounts or CashDokument2 SeitenFreshmen Students Bank Procedures For Non-ATM Accounts or CashKenn yahweexNoch keine Bewertungen
- DNJKFNKDNKLFDokument2 SeitenDNJKFNKDNKLFKenn yahweexNoch keine Bewertungen
- Pancreatic Cancer 1-ACS-tugas DR TeharDokument63 SeitenPancreatic Cancer 1-ACS-tugas DR Teharalyssafairudz21Noch keine Bewertungen
- Journal DR RequirementDokument10 SeitenJournal DR RequirementKenn yahweexNoch keine Bewertungen
- International LawDokument13 SeitenInternational LawKenn yahweexNoch keine Bewertungen
- Journal Ortho RequirementDokument13 SeitenJournal Ortho RequirementKenn yahweexNoch keine Bewertungen
- The Geriatric Depression Scale (GDSDokument2 SeitenThe Geriatric Depression Scale (GDSDiyah RahmawatiNoch keine Bewertungen
- THRADokument8 SeitenTHRAKenn yahweexNoch keine Bewertungen
- Journal Ortho RequirementDokument13 SeitenJournal Ortho RequirementKenn yahweexNoch keine Bewertungen
- DOHStat Health Status-MortalityDokument25 SeitenDOHStat Health Status-MortalityKenn yahweexNoch keine Bewertungen
- Post-Op Pain Management Nursing Care PlanDokument1 SeitePost-Op Pain Management Nursing Care PlanKenn yahweexNoch keine Bewertungen
- IntroductionDokument12 SeitenIntroductionKenn yahweexNoch keine Bewertungen
- Online EnrollDokument19 SeitenOnline EnrollKenn yahweexNoch keine Bewertungen
- Cavendish 2004Dokument18 SeitenCavendish 2004Kenn yahweexNoch keine Bewertungen
- Ascending Polyneuropathic Paralysis) Is An Acute, Rapidly Progressing, and Potentially Fatal Form ofDokument8 SeitenAscending Polyneuropathic Paralysis) Is An Acute, Rapidly Progressing, and Potentially Fatal Form ofKenn yahweexNoch keine Bewertungen
- CHN RXN PaperDokument1 SeiteCHN RXN PaperKenn yahweexNoch keine Bewertungen
- Structure and Function of The Skeletal System: Skeleton Dried Up BodyDokument4 SeitenStructure and Function of The Skeletal System: Skeleton Dried Up BodyKenn yahweexNoch keine Bewertungen
- Patient's ProfileDokument1 SeitePatient's ProfileKenn yahweexNoch keine Bewertungen
- NCPDokument6 SeitenNCPKenn yahweexNoch keine Bewertungen
- Integrating Spirituality Into Nurse Practitioner Practice:: The Importance of Finding The TimeDokument8 SeitenIntegrating Spirituality Into Nurse Practitioner Practice:: The Importance of Finding The TimeKenn yahweexNoch keine Bewertungen
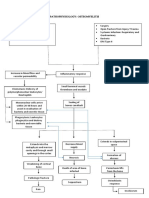
- PathophysiologyDokument2 SeitenPathophysiologyKenn yahweexNoch keine Bewertungen
- Drug StudyDokument11 SeitenDrug StudyKenn yahweexNoch keine Bewertungen
- The Dying Process Death Is Defined AsDokument5 SeitenThe Dying Process Death Is Defined AsKenn yahweexNoch keine Bewertungen
- OsteomyelitisDokument7 SeitenOsteomyelitisKenn yahweexNoch keine Bewertungen
- Introduction To Nursing PharmacologyDokument5 SeitenIntroduction To Nursing PharmacologyJon Adam Bermudez SamatraNoch keine Bewertungen
- Should Medical Marijuana Be Legalized For PatientsDokument4 SeitenShould Medical Marijuana Be Legalized For PatientsBing Cossid Quinones CatzNoch keine Bewertungen
- rút gọnDokument3 Seitenrút gọnUyen VuNoch keine Bewertungen
- How To Maintain Throat HygieneDokument9 SeitenHow To Maintain Throat Hygieneankita singhNoch keine Bewertungen
- Significance of Facebow Transfer: January 2020Dokument6 SeitenSignificance of Facebow Transfer: January 2020Mahmoud Ibrahem maanNoch keine Bewertungen
- Medication To Manage Abortion and MiscarriageDokument8 SeitenMedication To Manage Abortion and MiscarriageNisaNoch keine Bewertungen
- Elevated BilirubinDokument5 SeitenElevated BilirubinNovita ApramadhaNoch keine Bewertungen
- Full Body To Body Massage Centre in MG Road Gurgaon Delhi NCRDokument11 SeitenFull Body To Body Massage Centre in MG Road Gurgaon Delhi NCRFlip Body SpaNoch keine Bewertungen
- Buletin Farmasi 1/2014Dokument14 SeitenBuletin Farmasi 1/2014afiq83100% (1)
- Penatalaksanaan Penyakit Infeksi Tropik Dengan Ko-Infeksi Covid-19 - Assoc - Prof.dr - Dr. Kurnia Fitri Jamil, M.kes, SP - Pd-Kpti, FinasimDokument33 SeitenPenatalaksanaan Penyakit Infeksi Tropik Dengan Ko-Infeksi Covid-19 - Assoc - Prof.dr - Dr. Kurnia Fitri Jamil, M.kes, SP - Pd-Kpti, FinasimFikri FachriNoch keine Bewertungen
- Complications of 3rd TrimesterDokument49 SeitenComplications of 3rd TrimesterMA. JYRELL BONITONoch keine Bewertungen
- Infectiile Grave Extensive Ale Partilor MoiDokument49 SeitenInfectiile Grave Extensive Ale Partilor MoiLoredana BoghezNoch keine Bewertungen
- Expression of MDM2 and p16 in AngiomyolipomaDokument7 SeitenExpression of MDM2 and p16 in AngiomyolipomaTiago TavaresNoch keine Bewertungen
- Understanding the Benefits of Physical ActivitiesDokument17 SeitenUnderstanding the Benefits of Physical ActivitiesRealisan DulnuanNoch keine Bewertungen
- Remote Area Nursing Emergency GuidelinesDokument325 SeitenRemote Area Nursing Emergency Guidelineslavinia_dobrescu_1Noch keine Bewertungen
- 13 - Adverse Drug Reactions CausesDokument4 Seiten13 - Adverse Drug Reactions CausesRojas Evert AlonsoNoch keine Bewertungen
- PWAT (Panographic Wound Assesment Tool) RevisedDokument4 SeitenPWAT (Panographic Wound Assesment Tool) RevisedYunie ArmyatiNoch keine Bewertungen
- Vaccine Safety E Course Manual PDFDokument207 SeitenVaccine Safety E Course Manual PDFLeonita DwiNoch keine Bewertungen
- Unipex Onepager CapixylDokument1 SeiteUnipex Onepager CapixylalbertitorubinNoch keine Bewertungen
- US Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreDokument4 SeitenUS Elsevier Health Bookshop - Mosby, Saunders, Netter & MoreWilmer Zambrano GuerreroNoch keine Bewertungen
- ICU Accomplishment Report and Improvement PlanDokument5 SeitenICU Accomplishment Report and Improvement PlanMikhaelEarlSantosTacordaNoch keine Bewertungen
- NCM101 Health Assessment ExaminationDokument11 SeitenNCM101 Health Assessment ExaminationJonah R. Merano100% (1)
- A Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostDokument6 SeitenA Descriptive Study To Assess The Knowledge Regarding Management of Hyperemesis Gravidarum Among PostIJRASETPublicationsNoch keine Bewertungen
- List of Empanelled Hospitals in CGHS NagpurDokument58 SeitenList of Empanelled Hospitals in CGHS NagpurRajatNoch keine Bewertungen
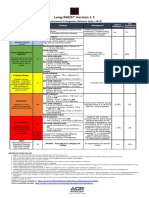
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Dokument1 SeiteLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNoch keine Bewertungen
- Artikel IlmiahDokument12 SeitenArtikel IlmiahAsti NurchasanahNoch keine Bewertungen
- Week 29 - DRRRDokument5 SeitenWeek 29 - DRRRMira VeranoNoch keine Bewertungen