Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- 2016 IT - Sheilding Guide PDFDokument40 Seiten2016 IT - Sheilding Guide PDFlazarosNoch keine Bewertungen
- Toh MFS8B 98B 003-11114-3AG1 PDFDokument92 SeitenToh MFS8B 98B 003-11114-3AG1 PDFDmitry NemtsoffNoch keine Bewertungen
- Babe Ruth Saves BaseballDokument49 SeitenBabe Ruth Saves BaseballYijun PengNoch keine Bewertungen
- Chapter 08 - Change in Accounting Policy: Problem 8-1 (AICPA Adapted)Dokument5 SeitenChapter 08 - Change in Accounting Policy: Problem 8-1 (AICPA Adapted)Kimberly Claire AtienzaNoch keine Bewertungen
- DDHDHSDHDokument38 SeitenDDHDHSDHHarlan SiMarmutNoch keine Bewertungen
- Jadwal Jaga Bedah Umum Kelas 1-4 Periode 17 September - Juli - 13 Oktober 2019Dokument2 SeitenJadwal Jaga Bedah Umum Kelas 1-4 Periode 17 September - Juli - 13 Oktober 2019Harlan SiMarmutNoch keine Bewertungen
- Critical Appraisal of The TopicsDokument9 SeitenCritical Appraisal of The TopicsHarlan SiMarmutNoch keine Bewertungen
- Des 18 Jan 19 Chief2b - 1a Edit Tatib-1Dokument3 SeitenDes 18 Jan 19 Chief2b - 1a Edit Tatib-1Harlan SiMarmutNoch keine Bewertungen
- A Nov-Des Edit Tatib 3Dokument2 SeitenA Nov-Des Edit Tatib 3Harlan SiMarmutNoch keine Bewertungen
- 17HospitalsAPLB2BDec Feb19Dokument1 Seite17HospitalsAPLB2BDec Feb19Harlan SiMarmutNoch keine Bewertungen
- Value of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaDokument5 SeitenValue of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaHarlan SiMarmutNoch keine Bewertungen
- C4 Vectors - Vector Lines PDFDokument33 SeitenC4 Vectors - Vector Lines PDFMohsin NaveedNoch keine Bewertungen
- Derebe TekesteDokument75 SeitenDerebe TekesteAbinet AdemaNoch keine Bewertungen
- Project Management TY BSC ITDokument57 SeitenProject Management TY BSC ITdarshan130275% (12)
- Chapter 4 - Basic ProbabilityDokument37 SeitenChapter 4 - Basic Probabilitynadya shafirahNoch keine Bewertungen
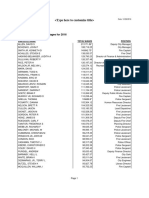
- 2016 W-2 Gross Wages CityDokument16 Seiten2016 W-2 Gross Wages CityportsmouthheraldNoch keine Bewertungen
- Hydro Electric Fire HistoryDokument3 SeitenHydro Electric Fire HistorygdmurfNoch keine Bewertungen
- FinalDokument18 SeitenFinalAkash LadNoch keine Bewertungen
- Contoh Discussion Text Tentang HomeworkDokument8 SeitenContoh Discussion Text Tentang Homeworkg3p35rs6100% (1)
- Frellwits Swedish Hosts FileDokument10 SeitenFrellwits Swedish Hosts FileAnonymous DsGzm0hQf5Noch keine Bewertungen
- Internship Report Format For Associate Degree ProgramDokument5 SeitenInternship Report Format For Associate Degree ProgramBisma AmjaidNoch keine Bewertungen
- Module6 Quiz1Dokument4 SeitenModule6 Quiz1karthik1555Noch keine Bewertungen
- ETAP Power Station ErrorDokument5 SeitenETAP Power Station ErroryogacruiseNoch keine Bewertungen
- SABRE MK-3 CFT Gel SpecDokument1 SeiteSABRE MK-3 CFT Gel Specseregio12Noch keine Bewertungen
- Эквивалентная Схема Мотра Теслы с Thomas2020Dokument7 SeitenЭквивалентная Схема Мотра Теслы с Thomas2020Алексей ЯмаNoch keine Bewertungen
- Elpodereso Case AnalysisDokument3 SeitenElpodereso Case AnalysisUsama17100% (2)
- Understanding PTS Security PDFDokument37 SeitenUnderstanding PTS Security PDFNeon LogicNoch keine Bewertungen
- Myanmar 1Dokument3 SeitenMyanmar 1Shenee Kate BalciaNoch keine Bewertungen
- Syllabus PDFDokument3 SeitenSyllabus PDFBibin Raj B SNoch keine Bewertungen
- Syllabus: What Is Artificial Intelligence? ProblemsDokument66 SeitenSyllabus: What Is Artificial Intelligence? ProblemsUdupiSri groupNoch keine Bewertungen
- EKC 202ABC ManualDokument16 SeitenEKC 202ABC ManualJose CencičNoch keine Bewertungen
- TESTDokument27 SeitenTESTLegal CheekNoch keine Bewertungen
- General Chemistry 2 Q1 Lesson 5 Endothermic and Exotheric Reaction and Heating and Cooling CurveDokument19 SeitenGeneral Chemistry 2 Q1 Lesson 5 Endothermic and Exotheric Reaction and Heating and Cooling CurveJolo Allexice R. PinedaNoch keine Bewertungen
- EGurukul - RetinaDokument23 SeitenEGurukul - RetinaOscar Daniel Mendez100% (1)
- 레벨 테스트Dokument2 Seiten레벨 테스트BNoch keine Bewertungen
- Advertising II Marathi VersionDokument91 SeitenAdvertising II Marathi VersionHarsh Sangani100% (1)
- FpsecrashlogDokument19 SeitenFpsecrashlogtim lokNoch keine Bewertungen