Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Dynamic model of manipulatorsDokument20 SeitenDynamic model of manipulatorsbalkyderNoch keine Bewertungen
- Linear Thermal Expansion of Solid Materials With A Vitreous Silica DilatometerDokument7 SeitenLinear Thermal Expansion of Solid Materials With A Vitreous Silica Dilatometerluis_may22Noch keine Bewertungen
- Pipeline Corrosion Assessment MethodsDokument21 SeitenPipeline Corrosion Assessment MethodsGilletNoch keine Bewertungen
- OracleDokument23 SeitenOracleriza arifNoch keine Bewertungen
- Hydrocarbons NotesDokument15 SeitenHydrocarbons Notesarjunrkumar2024Noch keine Bewertungen
- Jarless Con Door DriveDokument16 SeitenJarless Con Door DriveRoyal Akash100% (6)
- Create an access point for non-RouterOS laptop clientsDokument8 SeitenCreate an access point for non-RouterOS laptop clientsGorgeus WaffleNoch keine Bewertungen
- Cantors Paradox PDFDokument16 SeitenCantors Paradox PDFColectivo Utopía MoreliaNoch keine Bewertungen
- Network Layer: Computer Networking: A Top Down ApproachDokument83 SeitenNetwork Layer: Computer Networking: A Top Down ApproachMuhammad Bin ShehzadNoch keine Bewertungen
- Example 1 LS Dyna - Bullet Model SimulationDokument6 SeitenExample 1 LS Dyna - Bullet Model Simulationsunil_vrvNoch keine Bewertungen
- Biology - Physics Chemistry MCQS: Gyanm'S General Awareness - November 2014Dokument13 SeitenBiology - Physics Chemistry MCQS: Gyanm'S General Awareness - November 2014santosh.manojNoch keine Bewertungen
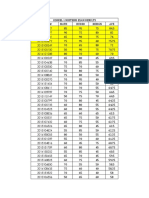
- Midterm Exam Result Ce199-1l 2Q1920Dokument3 SeitenMidterm Exam Result Ce199-1l 2Q1920RA CarpioNoch keine Bewertungen
- Tech Note 14Dokument2 SeitenTech Note 14meteohrNoch keine Bewertungen
- Python - How To Compute Jaccard Similarity From A Pandas Dataframe - Stack OverflowDokument4 SeitenPython - How To Compute Jaccard Similarity From A Pandas Dataframe - Stack OverflowJession DiwanganNoch keine Bewertungen
- Manual de Operacion de Bomba BlackmerDokument20 SeitenManual de Operacion de Bomba BlackmerMorales EduardoNoch keine Bewertungen
- F (X, Y) Sin (Xy) + X LN (Y) Find F at (0, )Dokument9 SeitenF (X, Y) Sin (Xy) + X LN (Y) Find F at (0, )muhammad abrarNoch keine Bewertungen
- Steps For Charm ConfigurationDokument7 SeitenSteps For Charm ConfigurationpoornasapNoch keine Bewertungen
- 10th Term Exams Computer Science PaperDokument2 Seiten10th Term Exams Computer Science PaperMohammad Tariq JavaidNoch keine Bewertungen
- Module 4 - What Is The Required Rate of ReturnDokument2 SeitenModule 4 - What Is The Required Rate of ReturnEthics BAENoch keine Bewertungen
- PF-CIS-Fall 2022 LABDokument4 SeitenPF-CIS-Fall 2022 LABMuhammad FaisalNoch keine Bewertungen
- Capsule Proposal TemplateDokument5 SeitenCapsule Proposal Templatematain elementary SchoolNoch keine Bewertungen
- Records of Intervention On The Findings of Test Results and Other Forms of AssessmentDokument10 SeitenRecords of Intervention On The Findings of Test Results and Other Forms of AssessmentLea May MagnoNoch keine Bewertungen
- Jaguar Land Rover Configuration Lifecycle Management WebDokument4 SeitenJaguar Land Rover Configuration Lifecycle Management WebStar Nair Rock0% (1)
- Smart Dustbin using ArduinoDokument22 SeitenSmart Dustbin using ArduinoEr Dinesh TambeNoch keine Bewertungen
- Line and Circle Drawing AlgorithmsDokument57 SeitenLine and Circle Drawing AlgorithmsMILAN K JAIN B.Tech CSE B 2018-2022Noch keine Bewertungen
- M.E. Comm. SystemsDokument105 SeitenM.E. Comm. SystemsShobana SNoch keine Bewertungen
- CD IK Tools v1.5 Plugin for C4D 9.6Dokument20 SeitenCD IK Tools v1.5 Plugin for C4D 9.6Syed Aal-HussainNoch keine Bewertungen
- Lab Manual MCSE 101Dokument35 SeitenLab Manual MCSE 101Juan JacksonNoch keine Bewertungen
- Rso PDFDokument120 SeitenRso PDFjohn shepardNoch keine Bewertungen
- Microstation V8I Accudraw Basics: Bentley Institute Course GuideDokument80 SeitenMicrostation V8I Accudraw Basics: Bentley Institute Course Guideh_eijy2743Noch keine Bewertungen