Das könnte Ihnen auch gefallen
- Aids To The Examination of Peripheral Nervous SystemDokument67 SeitenAids To The Examination of Peripheral Nervous SystemSenthilkumar ThiyagarajanNoch keine Bewertungen
- Nerves and Nerve Injuries: Vol 1: History, Embryology, Anatomy, Imaging, and DiagnosticsVon EverandNerves and Nerve Injuries: Vol 1: History, Embryology, Anatomy, Imaging, and DiagnosticsBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Aids To The Examination of The Peripheral Nervous System 4th Edition 2000Dokument67 SeitenAids To The Examination of The Peripheral Nervous System 4th Edition 2000Dwi Andriyani NimanNoch keine Bewertungen
- Movements and Orthopedic Tests: quick, easy, and reliableVon EverandMovements and Orthopedic Tests: quick, easy, and reliableNoch keine Bewertungen
- Evidence-Based Evaluation & Management of Common Spinal Conditions: A Guide for the Manual PractitionerVon EverandEvidence-Based Evaluation & Management of Common Spinal Conditions: A Guide for the Manual PractitionerBewertung: 5 von 5 Sternen5/5 (1)
- Essential Clinically Applied Anatomy of the Peripheral Nervous System in the LimbsVon EverandEssential Clinically Applied Anatomy of the Peripheral Nervous System in the LimbsNoch keine Bewertungen
- The Clinician's Guidebook to Lumbar Spine Disorders: Diagnosis & TreatmentVon EverandThe Clinician's Guidebook to Lumbar Spine Disorders: Diagnosis & TreatmentNoch keine Bewertungen
- Musculoskeletal Medicine in Primary Care: An Essential Guide for Examination, Diagnosis and ManagementVon EverandMusculoskeletal Medicine in Primary Care: An Essential Guide for Examination, Diagnosis and ManagementBewertung: 4 von 5 Sternen4/5 (2)
- Ultrasound and clinically guided Injection techniques on the musculoskeletal systemVon EverandUltrasound and clinically guided Injection techniques on the musculoskeletal systemNoch keine Bewertungen
- Atlas of EEG in Critical CareVon EverandAtlas of EEG in Critical CareLawrence HirschNoch keine Bewertungen
- Ultrasound Guided Musculoskeletal Procedures in Sports Medicine: A Practical AtlasVon EverandUltrasound Guided Musculoskeletal Procedures in Sports Medicine: A Practical AtlasBewertung: 5 von 5 Sternen5/5 (1)
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesVon EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesBewertung: 1 von 5 Sternen1/5 (1)
- Interventional Pain: A Step-by-Step Guide for the FIPP ExamVon EverandInterventional Pain: A Step-by-Step Guide for the FIPP ExamAgnes R. StogiczaNoch keine Bewertungen
- Interactions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionVon EverandInteractions between the Craniomandibular System and Cervical Spine: The influence of an unilateral change of occlusion on the upper cervical range of motionNoch keine Bewertungen
- Neurologic Examination: An Illustrated Guide to the Neurological ExaminationVon EverandNeurologic Examination: An Illustrated Guide to the Neurological ExaminationBewertung: 2 von 5 Sternen2/5 (1)
- Pain Syndromes in Neurology: Butterworths International Medical ReviewsVon EverandPain Syndromes in Neurology: Butterworths International Medical ReviewsHoward L. FieldsBewertung: 5 von 5 Sternen5/5 (1)
- MODIFIED POSTERIOR APPROACH TO THE HIP JOINTVon EverandMODIFIED POSTERIOR APPROACH TO THE HIP JOINTBewertung: 5 von 5 Sternen5/5 (1)
- AANEM LEWorkbookDokument80 SeitenAANEM LEWorkbooknewguy927Noch keine Bewertungen
- Essential NEUROLOGY for Medicine FinalsVon EverandEssential NEUROLOGY for Medicine FinalsBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Length Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesVon EverandLength Tension Testing Book 1, Lower Quadrant: A Workbook of Manual Therapy TechniquesBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Recent Advances in PhysiotherapyVon EverandRecent Advances in PhysiotherapyCecily PartridgeNoch keine Bewertungen
- Measuring Walking: A Handbook of Clinical Gait AnalysisVon EverandMeasuring Walking: A Handbook of Clinical Gait AnalysisBewertung: 5 von 5 Sternen5/5 (2)
- Cervical Radiculopathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandCervical Radiculopathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Intra-Operative Monitoring: A Comprehensive ApproachVon EverandIntra-Operative Monitoring: A Comprehensive ApproachNoch keine Bewertungen
- Durrant Myelopathy - Radiculopathy.and - Peripheral.entrapment - Syndromes PDFDokument395 SeitenDurrant Myelopathy - Radiculopathy.and - Peripheral.entrapment - Syndromes PDFsurnameNoch keine Bewertungen
- Anatomy for problem solving in sports medicine: The KneeVon EverandAnatomy for problem solving in sports medicine: The KneeBewertung: 3.5 von 5 Sternen3.5/5 (3)
- Comparative Kinesiology of the Human Body: Normal and Pathological ConditionsVon EverandComparative Kinesiology of the Human Body: Normal and Pathological ConditionsSalih AnginNoch keine Bewertungen
- Aicardi’s Diseases of the Nervous System in Childhood, 4th EditionVon EverandAicardi’s Diseases of the Nervous System in Childhood, 4th EditionAlexis ArzimanoglouNoch keine Bewertungen
- Innovative NeuromodulationVon EverandInnovative NeuromodulationJeffrey ArleNoch keine Bewertungen
- Orthopaedic Management in Cerebral Palsy, 2nd EditionVon EverandOrthopaedic Management in Cerebral Palsy, 2nd EditionHelen Meeks HorstmannBewertung: 3 von 5 Sternen3/5 (2)
- Pediatric Brain Stimulation: Mapping and Modulating the Developing BrainVon EverandPediatric Brain Stimulation: Mapping and Modulating the Developing BrainAdam KirtonNoch keine Bewertungen
- ACFrOgCQoS 8vusEkJ5naUqf0VaiLqAOGXIBMd9DGkNkrYbScqPgbzgpsPpIMAv1RXhsxOnjPh34IDbAypkIW udLxG6DcvF6bb5lf aXqRBjiJvDAyXfdTMdvNozVsDokument1.200 SeitenACFrOgCQoS 8vusEkJ5naUqf0VaiLqAOGXIBMd9DGkNkrYbScqPgbzgpsPpIMAv1RXhsxOnjPh34IDbAypkIW udLxG6DcvF6bb5lf aXqRBjiJvDAyXfdTMdvNozVsMarlon Pereira100% (3)
- Visually Memorable Neuroanatomy for BeginnersVon EverandVisually Memorable Neuroanatomy for BeginnersBewertung: 5 von 5 Sternen5/5 (1)
- Minimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachVon EverandMinimally Invasive Surgery for Chronic Pain Management: An Evidence-Based ApproachGiorgio PietramaggioriNoch keine Bewertungen
- Aids To The Examination of The Peripheral Nervous System - 5th Ed - 2010 PDFDokument73 SeitenAids To The Examination of The Peripheral Nervous System - 5th Ed - 2010 PDFClaudia MendozaNoch keine Bewertungen
- Functional Movement Disorder: Kathrin Lafaver Carine W. Maurer Timothy R. Nicholson David L. Perez EditorsDokument455 SeitenFunctional Movement Disorder: Kathrin Lafaver Carine W. Maurer Timothy R. Nicholson David L. Perez Editors李世民100% (3)
- Hand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachVon EverandHand Conditions and Examinations: a Rheumatologic and Orthopaedic ApproachNoch keine Bewertungen
- Advanced Techniques in Musculoskeletal Medicine & Physiotherapy - Using Minimally Invasive Therapies in Practice PDFDokument544 SeitenAdvanced Techniques in Musculoskeletal Medicine & Physiotherapy - Using Minimally Invasive Therapies in Practice PDFMuhammad Zaib100% (1)
- Basic Principles of Peripheral Nerve DisordersDokument288 SeitenBasic Principles of Peripheral Nerve DisordersJosé Ramírez100% (1)
- Neuropuncture™ Case Studies and Clinical Applications: Volume 1Von EverandNeuropuncture™ Case Studies and Clinical Applications: Volume 1Noch keine Bewertungen
- An Insider's Guide to Orthopedic Surgery: A Physical Therapist Shares the Keys to a Better RecoveryVon EverandAn Insider's Guide to Orthopedic Surgery: A Physical Therapist Shares the Keys to a Better RecoveryBewertung: 4 von 5 Sternen4/5 (1)
- Intracranial AneurysmsVon EverandIntracranial AneurysmsAndrew J. RingerNoch keine Bewertungen
- Tech RGNL 1 Nerve Conduction Studies KatirjiDokument52 SeitenTech RGNL 1 Nerve Conduction Studies KatirjiSinduja Jayaraj100% (1)
- Tarsal Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandTarsal Tunnel Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Vestibular DisorderDokument417 SeitenVestibular DisorderDEEKSHA ABROLNoch keine Bewertungen
- Biomechanics of the Spine: Basic Concepts, Spinal Disorders and TreatmentsVon EverandBiomechanics of the Spine: Basic Concepts, Spinal Disorders and TreatmentsFabio GalbuseraBewertung: 2 von 5 Sternen2/5 (1)
- The Choroid Plexus and Cerebrospinal Fluid: Emerging Roles in CNS Development, Maintenance, and Disease ProgressionVon EverandThe Choroid Plexus and Cerebrospinal Fluid: Emerging Roles in CNS Development, Maintenance, and Disease ProgressionJosh NemanNoch keine Bewertungen
- Carpal TunnelDokument10 SeitenCarpal TunnelasimulhaqNoch keine Bewertungen
- Posterior Triangle of The NeckDokument6 SeitenPosterior Triangle of The NeckMuhammad Imran QureshiNoch keine Bewertungen
- Double-Crush Syndrome - A Critical AnalysisDokument9 SeitenDouble-Crush Syndrome - A Critical AnalysisCelina Tam Ching LamNoch keine Bewertungen
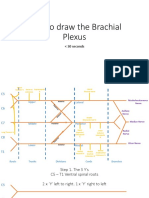
- How To Draw The Brachial PlexusDokument16 SeitenHow To Draw The Brachial PlexusHNoch keine Bewertungen
- Nasa Khan MRCS A Notes 2018 PDFDokument834 SeitenNasa Khan MRCS A Notes 2018 PDFWaqas Haleem100% (5)
- Ultrasound Guided Interscalene BrachialDokument10 SeitenUltrasound Guided Interscalene BrachialAnesthesiology FKUBNoch keine Bewertungen
- Lab Quiz#2Dokument4 SeitenLab Quiz#2Kimberly RamocanNoch keine Bewertungen
- Pembekalan BPI Sem 5Dokument40 SeitenPembekalan BPI Sem 5Mukhtar Ali MuktiNoch keine Bewertungen
- Analec B3 Brachial PlexusDokument2 SeitenAnalec B3 Brachial PlexusCaesar Anthony Dequito SamsonNoch keine Bewertungen
- Patient Positioning and AnaesthesiaDokument24 SeitenPatient Positioning and AnaesthesiaGrishma KothariNoch keine Bewertungen
- Master Anatomy ChartDokument21 SeitenMaster Anatomy ChartMonica Moya100% (5)
- MCEM Anatomy MCQ PDFDokument44 SeitenMCEM Anatomy MCQ PDFUgeshwaran Aristotle Reddy100% (1)
- Surgical Anatomy of The Neck: Nerves: Head & Neck Surgery CourseDokument46 SeitenSurgical Anatomy of The Neck: Nerves: Head & Neck Surgery CourseΑΘΑΝΑΣΙΟΣ ΚΟΥΤΟΥΚΤΣΗΣNoch keine Bewertungen
- Biomechanics NotesDokument21 SeitenBiomechanics Notesstarlight9394100% (1)
- Compa Horse and Human - NervesDokument12 SeitenCompa Horse and Human - NervesJames SumagaysayNoch keine Bewertungen
- Upper Limb Anatomy Quiz: Questions AnswersDokument5 SeitenUpper Limb Anatomy Quiz: Questions Answersapi-246259817Noch keine Bewertungen
- Rope Bottom GuideDokument20 SeitenRope Bottom GuideGabriela Maia67% (3)
- Anatomy and Physiology MnemonicsDokument7 SeitenAnatomy and Physiology MnemonicsLalajimNoch keine Bewertungen
- 03 Soft TissueDokument21 Seiten03 Soft TissueMajid Khan0% (1)
- Anatomy ShortcutDokument73 SeitenAnatomy ShortcutHARSHNoch keine Bewertungen
- The Roots Value of Each Branch Is Given in BracketsDokument8 SeitenThe Roots Value of Each Branch Is Given in BracketsAneela PervezNoch keine Bewertungen
- An Anatomical Study On Various Types of Suprascapular Notch, Its Relation With Glenoid Cavity and Morphometry of Scapula in South Indian PopulationDokument5 SeitenAn Anatomical Study On Various Types of Suprascapular Notch, Its Relation With Glenoid Cavity and Morphometry of Scapula in South Indian PopulationRaviprasanna K HNoch keine Bewertungen
- 0 MnemonicsDokument133 Seiten0 MnemonicsAlex Ivan Chen TejadaNoch keine Bewertungen
- 4 AxillaDokument31 Seiten4 AxillaRamesh KumarNoch keine Bewertungen
- Ulnar Nerve AnatomyDokument7 SeitenUlnar Nerve AnatomyOciel AcostaNoch keine Bewertungen
- (BCA HSB) Anatomy of The Upper Extremities (Dr. Gomez) Mimikyu X MustKnotes 2022Dokument15 Seiten(BCA HSB) Anatomy of The Upper Extremities (Dr. Gomez) Mimikyu X MustKnotes 2022Noreen Hannah GabrielNoch keine Bewertungen
- AXILLADokument56 SeitenAXILLAAxel ElisesNoch keine Bewertungen
- ShoulderDokument13 SeitenShoulderRaziv Maulana UsmanNoch keine Bewertungen
- Table Summary For Gross Anatomy of Upper LimbDokument20 SeitenTable Summary For Gross Anatomy of Upper Limbafifah zabidiNoch keine Bewertungen
- Brachial Plexus InjuryDokument14 SeitenBrachial Plexus InjuryYugaraj ThangaveluNoch keine Bewertungen