Das könnte Ihnen auch gefallen
- Example Electrical Installation Condition ReportDokument6 SeitenExample Electrical Installation Condition Reportapi-292622368100% (1)
- 2021 Handouts and TutorialsDokument414 Seiten2021 Handouts and TutorialsTrúc Ly Cáp thị100% (3)
- TREB Rental ApplicationDokument1 SeiteTREB Rental ApplicationDavid Pylyp0% (1)
- Business Plan For Fisheries Processing and ExportingDokument58 SeitenBusiness Plan For Fisheries Processing and ExportingCarina-Ioana Paraschiv83% (6)
- YV2 AdministrationDokument129 SeitenYV2 Administrationapi-19836714Noch keine Bewertungen
- 1 Republic v. CADokument5 Seiten1 Republic v. CAkjhenyo218502Noch keine Bewertungen
- Rental Application: Residential Form 410Dokument2 SeitenRental Application: Residential Form 410Chris. AguilarNoch keine Bewertungen
- (Toronto) 410 - Rental Application - ResidentialDokument2 Seiten(Toronto) 410 - Rental Application - Residentialcarpediem.kavithaNoch keine Bewertungen
- Rental Application ResidentialDokument1 SeiteRental Application ResidentialKennedy SundayNoch keine Bewertungen
- SSCollectiveAgreementCurrent E PDFDokument145 SeitenSSCollectiveAgreementCurrent E PDFDwight JonesNoch keine Bewertungen
- Ebrahim Al-Sharafi Rental AppDokument2 SeitenEbrahim Al-Sharafi Rental Appbstcpw2snnNoch keine Bewertungen
- Application For Removal of Tax Obligation (S) : Part ADokument3 SeitenApplication For Removal of Tax Obligation (S) : Part AmichaelNoch keine Bewertungen
- (Toronto) 410 - Rental Application - ResidentialDokument2 Seiten(Toronto) 410 - Rental Application - Residentialshernell concessioNoch keine Bewertungen
- Registration Form: A. Personal InformationDokument4 SeitenRegistration Form: A. Personal InformationZulmy RhamadityaNoch keine Bewertungen
- Acc 1152 Dol224 HandbookDokument48 SeitenAcc 1152 Dol224 Handbooksapphire8Noch keine Bewertungen
- Leave Application FormDokument1 SeiteLeave Application Formsucceed mutungamidzwaNoch keine Bewertungen
- Constitution FOR Ecotourism Australia Limited: A Public Company Limited by GuaranteeDokument32 SeitenConstitution FOR Ecotourism Australia Limited: A Public Company Limited by GuaranteejverhoefNoch keine Bewertungen
- Nus Law Evidence My NotesDokument18 SeitenNus Law Evidence My NotesSyed HaiqalNoch keine Bewertungen
- Personal / Appliance / Loan AgreementDokument2 SeitenPersonal / Appliance / Loan AgreementNithya RahulNoch keine Bewertungen
- 5) Seksyen I - BAHAGIAN C - Form CSA2014-Quantity Surveying (Amendment 2018)Dokument65 Seiten5) Seksyen I - BAHAGIAN C - Form CSA2014-Quantity Surveying (Amendment 2018)bkkdennisNoch keine Bewertungen
- O'neill RD - Rental ApplicationDokument2 SeitenO'neill RD - Rental Applicationbestreview7Noch keine Bewertungen
- OD SlipDokument1 SeiteOD Slipvasudeva tNoch keine Bewertungen
- Rental App CurtDokument2 SeitenRental App CurtMaika Projects SupportNoch keine Bewertungen
- Don Xin Nghi Phep Di Du Lich Bang Tieng AnhDokument1 SeiteDon Xin Nghi Phep Di Du Lich Bang Tieng AnhKim ngânNoch keine Bewertungen
- 2016 Application For SabbatticalDokument2 Seiten2016 Application For SabbatticalOlanrewaju AhmedNoch keine Bewertungen
- DEALERSHIP APPLICATION FORM@KivipPdfDokument6 SeitenDEALERSHIP APPLICATION FORM@KivipPdfOm Prakash SharmaNoch keine Bewertungen
- Agritopia CCRs 12-10-02Dokument57 SeitenAgritopia CCRs 12-10-02Faaria ZainabNoch keine Bewertungen
- Expression of Wish Form: Beneficiary 1 Beneficiary 2Dokument1 SeiteExpression of Wish Form: Beneficiary 1 Beneficiary 2Moon3pellNoch keine Bewertungen
- Law InsolvencyDokument30 SeitenLaw InsolvencyTawanda MahereNoch keine Bewertungen
- The Jambar Policy ManualDokument52 SeitenThe Jambar Policy ManualCassandraTwoeyNoch keine Bewertungen
- Format of Character Certificate by Principal of The Institution Last AttendedDokument1 SeiteFormat of Character Certificate by Principal of The Institution Last Attendedapi-15171922100% (2)
- APPLICATION FOR THE GRANT OR RENEWAL OF A LICENSE TO MANUFACTURE OR PRODUCE AN ALCOHOLIC DRINKd41dDokument2 SeitenAPPLICATION FOR THE GRANT OR RENEWAL OF A LICENSE TO MANUFACTURE OR PRODUCE AN ALCOHOLIC DRINKd41dCalvin kamothoNoch keine Bewertungen
- Hampton Golf HandbookDokument91 SeitenHampton Golf HandbookBryan LuttrellNoch keine Bewertungen
- 2015 11 03 Draft v1 Improved Study Guide ATPJVCDokument139 Seiten2015 11 03 Draft v1 Improved Study Guide ATPJVCDanica Irish RevillaNoch keine Bewertungen
- SLR CONSULTING LIMITED Sub-Consultant's Agreement V3.1Dokument20 SeitenSLR CONSULTING LIMITED Sub-Consultant's Agreement V3.1borrowmanaNoch keine Bewertungen
- S RG 1014 Issue 10 EnabledDokument6 SeitenS RG 1014 Issue 10 EnabledPatrick TongNoch keine Bewertungen
- WENDT ContractDokument41 SeitenWENDT ContractWGRZ-TVNoch keine Bewertungen
- Graduation Internship Report: Foreign Trade University Ho Chi Minh CampusDokument45 SeitenGraduation Internship Report: Foreign Trade University Ho Chi Minh CampusPhạm Huyền TrangNoch keine Bewertungen
- Non-Compliance Report (NCR) : Liconin Limitted CompanyDokument2 SeitenNon-Compliance Report (NCR) : Liconin Limitted CompanyMINH THÁINoch keine Bewertungen
- Format of Application For C Adm O, Air Force Station, .....................................................Dokument3 SeitenFormat of Application For C Adm O, Air Force Station, .....................................................Sunil RAYALASEEMA GRAPHICSNoch keine Bewertungen
- Table of ContentsDokument2 SeitenTable of ContentsKyrie IrvingNoch keine Bewertungen
- HR-104!90!20 Job Application Form For Academic PositionDokument3 SeitenHR-104!90!20 Job Application Form For Academic PositionMohana SundaramNoch keine Bewertungen
- International Student Application Form: Section 1: Course DetailsDokument4 SeitenInternational Student Application Form: Section 1: Course DetailsAbde SsamadNoch keine Bewertungen
- Interactive Voice Response (Ivr) System RFP: Citizens Energy / CITGO Venezuela Heating Oil Program Division (HOP)Dokument25 SeitenInteractive Voice Response (Ivr) System RFP: Citizens Energy / CITGO Venezuela Heating Oil Program Division (HOP)Kathir ChandruNoch keine Bewertungen
- Introductory Statement Form EnglishDokument3 SeitenIntroductory Statement Form EnglishfarukhNoch keine Bewertungen
- Saj Ceramics Human Resources Policy Manual FinalDokument68 SeitenSaj Ceramics Human Resources Policy Manual FinalChris OntitiNoch keine Bewertungen
- Remuneration Bill 01Dokument1 SeiteRemuneration Bill 01Mourian AmanNoch keine Bewertungen
- American Matrimony - SOW - v1.0Dokument20 SeitenAmerican Matrimony - SOW - v1.0AliNoch keine Bewertungen
- CTA Vendor GuideDokument28 SeitenCTA Vendor GuideМаксим ЖулинскийNoch keine Bewertungen
- Melaku Mara (Thesis)Dokument54 SeitenMelaku Mara (Thesis)mift adem100% (1)
- Mgt368 Table of ContentsDokument3 SeitenMgt368 Table of ContentsThe TopTeN CircleNoch keine Bewertungen
- For Candidates With Ordinary Level QualificationDokument3 SeitenFor Candidates With Ordinary Level QualificationS HerathNoch keine Bewertungen
- Salary Sacrifice Share PlanDokument26 SeitenSalary Sacrifice Share PlanIkramNoch keine Bewertungen
- c0426 EstDokument87 Seitenc0426 EstAli BashirNoch keine Bewertungen
- Aero Gear Employee HandbookDokument35 SeitenAero Gear Employee Handbookthomas h.johnsonNoch keine Bewertungen
- Last Pay CertificateDokument2 SeitenLast Pay CertificateJayaprakash Vayakkoth Madham100% (3)
- (Toronto) 410 - Rental Application - Residential 2Dokument2 Seiten(Toronto) 410 - Rental Application - Residential 2lauramartinez2313Noch keine Bewertungen
- MA - Application 2Dokument3 SeitenMA - Application 2dilshaimali030Noch keine Bewertungen
- The Forensic Documentation Sourcebook: The Complete Paperwork Resource for Forensic Mental Health PracticeVon EverandThe Forensic Documentation Sourcebook: The Complete Paperwork Resource for Forensic Mental Health PracticeBewertung: 1 von 5 Sternen1/5 (1)
- Teardowns: Learn How Electronics Work by Taking Them ApartVon EverandTeardowns: Learn How Electronics Work by Taking Them ApartNoch keine Bewertungen
- Animal Welfare Act, No 19 of 2013Dokument26 SeitenAnimal Welfare Act, No 19 of 2013ioanidteNoch keine Bewertungen
- HUAWEI MediaPad T2 7.0 Pro User Guide PLE-701L 01 EnglishDokument41 SeitenHUAWEI MediaPad T2 7.0 Pro User Guide PLE-701L 01 EnglishioanidteNoch keine Bewertungen
- Compressor Troubleshooting GuideDokument40 SeitenCompressor Troubleshooting GuideioanidteNoch keine Bewertungen
- Public Notice WMA OAB 383S IFB 5 18 Technical Assistance For MJTPDokument2 SeitenPublic Notice WMA OAB 383S IFB 5 18 Technical Assistance For MJTPioanidteNoch keine Bewertungen
- Interim Storage Hazardous Waste Facility Inaugurated at La ChaumièreDokument1 SeiteInterim Storage Hazardous Waste Facility Inaugurated at La ChaumièreioanidteNoch keine Bewertungen
- Flows and LoadsDokument1 SeiteFlows and LoadsioanidteNoch keine Bewertungen
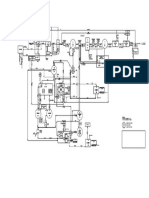
- Process & Flow Diagram PDFDokument1 SeiteProcess & Flow Diagram PDFioanidteNoch keine Bewertungen
- Process & Flow Diagram PDFDokument1 SeiteProcess & Flow Diagram PDFioanidteNoch keine Bewertungen
- Process & Flow DiagramDokument1 SeiteProcess & Flow DiagramioanidteNoch keine Bewertungen
- FERDINAND A. CRUZ vs. JUDGE PRISCILLA MIJARESDokument2 SeitenFERDINAND A. CRUZ vs. JUDGE PRISCILLA MIJARESVincent john NacuaNoch keine Bewertungen
- Law of Tort Including MV Act and Consumer Protection Laws AW5NFykMIvDokument2 SeitenLaw of Tort Including MV Act and Consumer Protection Laws AW5NFykMIvKrishna DemblaNoch keine Bewertungen
- 2021 San Beda Red Book Remedial Law-UnlockedDokument390 Seiten2021 San Beda Red Book Remedial Law-UnlockedPaolo OngsiakoNoch keine Bewertungen
- Juvenile Justice Week 2Dokument12 SeitenJuvenile Justice Week 2api-293974479Noch keine Bewertungen
- PurchaseReceipt 230804020042 VendorDokument3 SeitenPurchaseReceipt 230804020042 VendorLiesa StoneNoch keine Bewertungen
- The Interface Between National Land Law and Kalinga Land LawDokument37 SeitenThe Interface Between National Land Law and Kalinga Land LawAD ANTHONY CRISOSTOMONoch keine Bewertungen
- GST Ramu PatelDokument3 SeitenGST Ramu PatelGyamar TangaNoch keine Bewertungen
- B7 - FLP WORKSHOP 1 - Term 2, Week 4Dokument15 SeitenB7 - FLP WORKSHOP 1 - Term 2, Week 4Winston RuhayanaNoch keine Bewertungen
- The Lawyer and The ClientDokument30 SeitenThe Lawyer and The ClientSherlyn Paran Paquit-Selda100% (1)
- Oblicon-Finals (Answer Key)Dokument4 SeitenOblicon-Finals (Answer Key)KimberlyNoch keine Bewertungen
- Jurisprudence ProjectDokument15 SeitenJurisprudence Projectdiptajit dasNoch keine Bewertungen
- IjkaDokument3 SeitenIjkaTeleboy YusonNoch keine Bewertungen
- Revised Manual For Prosecutors 2008 PDFDokument331 SeitenRevised Manual For Prosecutors 2008 PDFHermay BanarioNoch keine Bewertungen
- People of The Philippines vs. Jeffrey Marcos y Anduyan - CR - HC-12455 - 02162021Dokument19 SeitenPeople of The Philippines vs. Jeffrey Marcos y Anduyan - CR - HC-12455 - 02162021viktor samuel fontanillaNoch keine Bewertungen
- Landshire Food Svs Inc v. Coghill 709 S.W.2d 509Dokument6 SeitenLandshire Food Svs Inc v. Coghill 709 S.W.2d 509Thalia SandersNoch keine Bewertungen
- Take Home Test (Final Assessment) 5.2.2021Dokument4 SeitenTake Home Test (Final Assessment) 5.2.2021Zafry TahirNoch keine Bewertungen
- MslimLaw ProjectDokument21 SeitenMslimLaw ProjectRazor RockNoch keine Bewertungen
- Charanjit v. State of Punjab, (2013) 11 SCC 163Dokument8 SeitenCharanjit v. State of Punjab, (2013) 11 SCC 163Sundaram OjhaNoch keine Bewertungen
- Investigative Assistance Request Re Pres. Moise Assassination - Embassy of HaitiDokument1 SeiteInvestigative Assistance Request Re Pres. Moise Assassination - Embassy of HaitiFrancis Liendo EcharryNoch keine Bewertungen
- Cost Insurance Freight PresentationDokument11 SeitenCost Insurance Freight PresentationGumisiriza BrintonNoch keine Bewertungen
- SP 066Dokument1 SeiteSP 066Nguyen Hong HaNoch keine Bewertungen
- 1 - 6 - 1 - Form For Renewal of Arms LicenseDokument8 Seiten1 - 6 - 1 - Form For Renewal of Arms LicenseTanmayesh KohliNoch keine Bewertungen
- Elements of A Trust - Graphic IllustrationDokument68 SeitenElements of A Trust - Graphic Illustrationsigma66Noch keine Bewertungen
- 2 Rem1 SyllabusDokument18 Seiten2 Rem1 SyllabusChristy SanguyuNoch keine Bewertungen
- Case Digests 010619Dokument9 SeitenCase Digests 010619Andrea IvanneNoch keine Bewertungen
- Digest - Tecson v. COMELECDokument4 SeitenDigest - Tecson v. COMELECJD CensonNoch keine Bewertungen
- Questionnaire Power of The StateDokument10 SeitenQuestionnaire Power of The StateBryan BorjeNoch keine Bewertungen
- Vermen Realty v. CA, 224 SCRA 549Dokument9 SeitenVermen Realty v. CA, 224 SCRA 549Christia Sandee SuanNoch keine Bewertungen