Das könnte Ihnen auch gefallen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Reynold A. Nicholson - The Mystics of IslamDokument65 SeitenReynold A. Nicholson - The Mystics of IslamLuminon SamanNoch keine Bewertungen
- B737-3 ATA 23 CommunicationsDokument112 SeitenB737-3 ATA 23 CommunicationsPaul RizlNoch keine Bewertungen
- Medical Parasitology PDFDokument150 SeitenMedical Parasitology PDFYajee Macapallag100% (1)
- Carinthia Katalog DownloadDokument16 SeitenCarinthia Katalog DownloadOperator_010100% (2)
- F24 60manual (New)Dokument14 SeitenF24 60manual (New)Robert CumpaNoch keine Bewertungen
- A History of Pharmacy in PicturesDokument41 SeitenA History of Pharmacy in PicturesPhan Cảnh Trình100% (2)
- Gaffin, Biblical Theology and Westminster StandardsDokument16 SeitenGaffin, Biblical Theology and Westminster StandardstheoarticlesNoch keine Bewertungen
- Python For BiologistsDokument227 SeitenPython For BiologistsSatyadev PolisettiNoch keine Bewertungen
- Tokyo Guidelines 2018Dokument115 SeitenTokyo Guidelines 2018Alik Razi100% (1)
- Pellicon 2 Validation Guide PDFDokument45 SeitenPellicon 2 Validation Guide PDFtakwahs12135Noch keine Bewertungen
- Screening Methods For Natural Products With Antimicrobial Activity A Review of The LiteratureDokument23 SeitenScreening Methods For Natural Products With Antimicrobial Activity A Review of The LiteratureCharbel Acar100% (1)
- Laboratory Id of Arthropod EctoparasitesDokument22 SeitenLaboratory Id of Arthropod EctoparasitesPhan Cảnh TrìnhNoch keine Bewertungen
- Dong Tam Snake FarmDokument6 SeitenDong Tam Snake FarmPhan Cảnh TrìnhNoch keine Bewertungen
- Probiotics For Prevention and Treatment Of.90Dokument12 SeitenProbiotics For Prevention and Treatment Of.90wendaNoch keine Bewertungen
- Diagnostic Malaria UpdateDokument25 SeitenDiagnostic Malaria UpdatePhan Cảnh TrìnhNoch keine Bewertungen
- J. Antimicrob. Chemother. 2003 Arévalo 163 6Dokument4 SeitenJ. Antimicrob. Chemother. 2003 Arévalo 163 6Phan Cảnh TrìnhNoch keine Bewertungen
- TSB Presavation 15% GlycerolDokument1 SeiteTSB Presavation 15% GlycerolPhan Cảnh TrìnhNoch keine Bewertungen
- 4 - CysticercosisDokument18 Seiten4 - CysticercosisPhan Cảnh TrìnhNoch keine Bewertungen
- GiardiasdagsaDokument36 SeitenGiardiasdagsaPhan Cảnh TrìnhNoch keine Bewertungen
- BaiGiang-PT-TKHDT-Thay Binh PDFDokument184 SeitenBaiGiang-PT-TKHDT-Thay Binh PDFPhan Cảnh TrìnhNoch keine Bewertungen
- Cellulose VSVDokument27 SeitenCellulose VSVPhan Cảnh TrìnhNoch keine Bewertungen
- NCCLS 1999 ResumenDokument7 SeitenNCCLS 1999 Resumenlithium manNoch keine Bewertungen
- CandidiasisDokument39 SeitenCandidiasisPhan Cảnh TrìnhNoch keine Bewertungen
- Fungal Biology Lecture 2c (F09)Dokument3 SeitenFungal Biology Lecture 2c (F09)Phan Cảnh TrìnhNoch keine Bewertungen
- 24Dokument5 Seiten24Phan Cảnh TrìnhNoch keine Bewertungen
- Fungal SymbiosisDokument10 SeitenFungal SymbiosisPhan Cảnh TrìnhNoch keine Bewertungen
- Fungal Biology Lecture 1 (F09) - 2Dokument8 SeitenFungal Biology Lecture 1 (F09) - 2Phan Cảnh TrìnhNoch keine Bewertungen
- Role of Sodium Acetate PDFDokument8 SeitenRole of Sodium Acetate PDFPhan Cảnh TrìnhNoch keine Bewertungen
- Detels AgentsDokument29 SeitenDetels AgentsPhan Cảnh TrìnhNoch keine Bewertungen
- Full Record Item 385Dokument7 SeitenFull Record Item 385Phan Cảnh TrìnhNoch keine Bewertungen
- Fungal SymbiosisDokument10 SeitenFungal SymbiosisPhan Cảnh TrìnhNoch keine Bewertungen
- Fungal SymbiosisDokument10 SeitenFungal SymbiosisPhan Cảnh TrìnhNoch keine Bewertungen
- Tinh An Toan Cua B. Subtilis Va B. AmyloliquefaciensDokument4 SeitenTinh An Toan Cua B. Subtilis Va B. AmyloliquefaciensPhan Cảnh TrìnhNoch keine Bewertungen
- Announcement Student Video Contest Final enDokument2 SeitenAnnouncement Student Video Contest Final enPhan Cảnh TrìnhNoch keine Bewertungen
- e17161456783ae14e723abc766afb45fDokument11 Seitene17161456783ae14e723abc766afb45fPhan Cảnh TrìnhNoch keine Bewertungen
- Azure Machine Learning StudioDokument17 SeitenAzure Machine Learning StudioNurain IsmailNoch keine Bewertungen
- BITS Pilani: Determination of Extreme Pressure, Wear Preventive Characteristics of Lubricants Using Four Ball TesterDokument10 SeitenBITS Pilani: Determination of Extreme Pressure, Wear Preventive Characteristics of Lubricants Using Four Ball Testerakash chNoch keine Bewertungen
- Eco Exercise 3answer Ans 1Dokument8 SeitenEco Exercise 3answer Ans 1Glory PrintingNoch keine Bewertungen
- Parameters Identification of Induction Motor Model BasedDokument10 SeitenParameters Identification of Induction Motor Model Basedretrueke1170Noch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakaMel DaNoch keine Bewertungen
- Ecall Vs NG EcallDokument6 SeitenEcall Vs NG EcallTrần Văn DũngNoch keine Bewertungen
- Model Detailed Project Report: Animal Feed Making UnitDokument19 SeitenModel Detailed Project Report: Animal Feed Making UnitShashi ShekharNoch keine Bewertungen
- Youth Camp Registration Form-2022Dokument1 SeiteYouth Camp Registration Form-2022FlerkNoch keine Bewertungen
- Manual of Sensorless Brushless Motor Speed Controller: Pentium SeriesDokument4 SeitenManual of Sensorless Brushless Motor Speed Controller: Pentium Seriesfosavo5839Noch keine Bewertungen
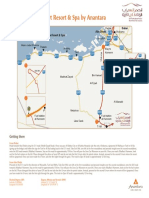
- Qasr Al Sarab Desert Resort Location Map June2012Dokument1 SeiteQasr Al Sarab Desert Resort Location Map June2012Anant GârgNoch keine Bewertungen
- Karl MarxDokument4 SeitenKarl Marxeirvine noah isidroNoch keine Bewertungen
- Valdez, Shenny RoseDokument3 SeitenValdez, Shenny Roseyeng botzNoch keine Bewertungen
- BIO 201 Chapter 11 LectureDokument34 SeitenBIO 201 Chapter 11 LectureDrPearcyNoch keine Bewertungen
- Phrasal Verbs Related To HealthDokument2 SeitenPhrasal Verbs Related To HealthKnuckles El Naco Narco LechugueroNoch keine Bewertungen
- 1 Circuit TheoryDokument34 Seiten1 Circuit TheoryLove StrikeNoch keine Bewertungen
- Asco Series 238 ASCO Pilot Operated Solenoid Valves (Floating Diaphragm)Dokument2 SeitenAsco Series 238 ASCO Pilot Operated Solenoid Valves (Floating Diaphragm)Khyle Laurenz DuroNoch keine Bewertungen
- Diagnosis of TrypanosomiasisDokument82 SeitenDiagnosis of TrypanosomiasisDrVijayata Choudhary100% (1)
- Homeo Treatment of Eye Diseases and AllergiesDokument17 SeitenHomeo Treatment of Eye Diseases and AllergiesZia AbbasiNoch keine Bewertungen
- Test09 Eoc Algebra2 ReducedDokument33 SeitenTest09 Eoc Algebra2 ReducedkristymadimikeNoch keine Bewertungen
- Resume: Satyam KumarDokument3 SeitenResume: Satyam KumarEr Satyam Kumar KrantiNoch keine Bewertungen
- Birla MEEP Op ManualDokument43 SeitenBirla MEEP Op ManualAshok ChettiyarNoch keine Bewertungen
- ARK - Intel® Core™ I3-370m Processor (3M Cache, 2Dokument3 SeitenARK - Intel® Core™ I3-370m Processor (3M Cache, 2Delzi Guindra AdriNoch keine Bewertungen
- Clocks (New) PDFDokument5 SeitenClocks (New) PDFAbhay DabhadeNoch keine Bewertungen