Das könnte Ihnen auch gefallen
- NonalcoholicFattyLiverDisease2012 25762 FTPDokument19 SeitenNonalcoholicFattyLiverDisease2012 25762 FTPbudi_26690Noch keine Bewertungen
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 3Dokument1 SeiteExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 3CunCunAlAndraNoch keine Bewertungen
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 2Dokument1 SeiteExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 2CunCunAlAndraNoch keine Bewertungen
- Expansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 1Dokument1 SeiteExpansion Tank Design Guide, How To Size and Select An Expansion Tank For A Chilled Water System 1CunCunAlAndraNoch keine Bewertungen
- Process Plant Layout - Seán Moran 3-4Dokument2 SeitenProcess Plant Layout - Seán Moran 3-4CunCunAlAndraNoch keine Bewertungen
- Evaporative Condenser Engineering Manual: Technical ResourcesDokument18 SeitenEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimNoch keine Bewertungen
- Evaporative Condenser Engineering Manual: Technical ResourcesDokument18 SeitenEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimNoch keine Bewertungen
- Safety Data Sheet for FAME (Fatty Acid Methyl EsterDokument14 SeitenSafety Data Sheet for FAME (Fatty Acid Methyl EsterCunCunAlAndraNoch keine Bewertungen
- Evaporative Condenser Engineering Manual: Technical ResourcesDokument18 SeitenEvaporative Condenser Engineering Manual: Technical ResourcesMohamed IbrahimNoch keine Bewertungen
- RCOG Guidelines - Gestational Trophoblastic DiseaseDokument12 SeitenRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- Process Plant Layout - Seán Moran 1-2Dokument2 SeitenProcess Plant Layout - Seán Moran 1-2CunCunAlAndra100% (1)
- Management Gathering 0718 - Distribution - v5 CoverDokument1 SeiteManagement Gathering 0718 - Distribution - v5 CoverCunCunAlAndraNoch keine Bewertungen
- Consulting Business ModelDokument1 SeiteConsulting Business ModelCunCunAlAndraNoch keine Bewertungen
- GF Signet 515 2536 Manual02Dokument1 SeiteGF Signet 515 2536 Manual02CunCunAlAndraNoch keine Bewertungen
- Kjae-68-101 Transfusion-Related Acute Lung InjuryDokument5 SeitenKjae-68-101 Transfusion-Related Acute Lung InjuryCunCunAlAndraNoch keine Bewertungen
- GF Signet 515 2536 Manual01Dokument1 SeiteGF Signet 515 2536 Manual01CunCunAlAndraNoch keine Bewertungen
- 1348493956.2409obstetrics Handbook PDFDokument48 Seiten1348493956.2409obstetrics Handbook PDFdrng48Noch keine Bewertungen
- Pitri - GI.Pemicu 4. GE+ Tifus AbdominalisDokument154 SeitenPitri - GI.Pemicu 4. GE+ Tifus AbdominalisCunCunAlAndraNoch keine Bewertungen
- Early Liver TransplantationDokument11 SeitenEarly Liver TransplantationCunCunAlAndraNoch keine Bewertungen
- Gastro Enter Oh Epa ToDokument29 SeitenGastro Enter Oh Epa TodeliaintanNoch keine Bewertungen
- Daftar Obat AnesDokument44 SeitenDaftar Obat AnesCunCunAlAndraNoch keine Bewertungen
- RCOG Guidelines - Gestational Trophoblastic DiseaseDokument12 SeitenRCOG Guidelines - Gestational Trophoblastic Diseasemob3100% (1)
- Problem 5 Git: Ivan MichaelDokument68 SeitenProblem 5 Git: Ivan MichaelCunCunAlAndraNoch keine Bewertungen
- MAPAX1Dokument2 SeitenMAPAX1CunCunAlAndraNoch keine Bewertungen
- RicoDokument62 SeitenRicoCunCunAlAndraNoch keine Bewertungen
- RicoDokument62 SeitenRicoCunCunAlAndraNoch keine Bewertungen
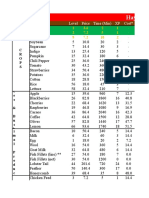
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- Hay Day Price Profit AnalysisDokument112 SeitenHay Day Price Profit AnalysisCunCunAlAndraNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5782)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- FMcase 2Dokument27 SeitenFMcase 2Ryan Townsend100% (3)
- ISONIAZIDDokument2 SeitenISONIAZIDPoet POet PoEtNoch keine Bewertungen
- CTG NewDokument23 SeitenCTG NewLola Putri100% (1)
- Tril-P Pain Relief Tablets Marketing PlanDokument19 SeitenTril-P Pain Relief Tablets Marketing PlanNauman AkramNoch keine Bewertungen
- Anaesthesia For Medical Students-Review QuestionsDokument20 SeitenAnaesthesia For Medical Students-Review QuestionsJohnny Lee100% (6)
- Clinical Psychology For TraineesDokument301 SeitenClinical Psychology For TraineesRoxana Dragomirescu91% (23)
- Holistic Healing  " Sujok Therapy (PDFDokument24 SeitenHolistic Healing  " Sujok Therapy (PDFDraghici Valentin80% (5)
- ReferensiDokument126 SeitenReferensiFatchul ChoiriNoch keine Bewertungen
- Aminopilyn Injeksi Berthyco Atropin Injeksi Benocetam (Piracetam) Bisolvon InjeksiDokument4 SeitenAminopilyn Injeksi Berthyco Atropin Injeksi Benocetam (Piracetam) Bisolvon InjeksiGina SakinahNoch keine Bewertungen
- English Language SBA 2022Dokument10 SeitenEnglish Language SBA 2022Le-Tshe FontanelleNoch keine Bewertungen
- Ijpp 2006Dokument356 SeitenIjpp 2006G Venkatesh100% (1)
- Ijsred V2i1p17Dokument9 SeitenIjsred V2i1p17IJSREDNoch keine Bewertungen
- Get Pregnant Naturally eBookDokument189 SeitenGet Pregnant Naturally eBookGede Adél-JúliaNoch keine Bewertungen
- Mass Vs Niche TourismDokument4 SeitenMass Vs Niche TourismRaymondGeNoch keine Bewertungen
- Chap4 Hemodynamics F2Dokument12 SeitenChap4 Hemodynamics F2Twinkle Salonga100% (3)
- Pharma Midterms CnsDokument67 SeitenPharma Midterms CnsAL-NAZAERNoch keine Bewertungen
- Limitations of Autograft and Allograft New Synthetic Solutions PDFDokument10 SeitenLimitations of Autograft and Allograft New Synthetic Solutions PDFSantiago VázquezNoch keine Bewertungen
- Meridian Flush Empowerments Levels 3&4 Manual PDFDokument8 SeitenMeridian Flush Empowerments Levels 3&4 Manual PDFJoyce Lozano100% (2)
- Nurs 5023 - Soap 5Dokument5 SeitenNurs 5023 - Soap 5api-308904543100% (2)
- Quick Cleanse 15 Day DetoxDokument44 SeitenQuick Cleanse 15 Day DetoxAnonymous YtbUfrXYNoch keine Bewertungen
- Book Report "Why Zebra's Don't Get Ulcer's"Dokument7 SeitenBook Report "Why Zebra's Don't Get Ulcer's"api-242679829Noch keine Bewertungen
- Journal Course Evidence Based Use of Nonopioid Analgesics August 2018Dokument7 SeitenJournal Course Evidence Based Use of Nonopioid Analgesics August 2018DesywinNoch keine Bewertungen
- Exam 1 Notes PDFDokument21 SeitenExam 1 Notes PDFMargauxNoch keine Bewertungen
- Pregestational ConditionsDokument46 SeitenPregestational ConditionsSheryl M. Ablao50% (2)
- Persistence Market ResearchDokument8 SeitenPersistence Market Researchapi-302003482Noch keine Bewertungen
- MRI Implementation in Gynecologic and Prostate HDR Brachytherapy - Considerations From Simulation To TreatmentDokument72 SeitenMRI Implementation in Gynecologic and Prostate HDR Brachytherapy - Considerations From Simulation To TreatmentJose NetoNoch keine Bewertungen
- JWCE Catalog 2013Dokument10 SeitenJWCE Catalog 2013jsalas85Noch keine Bewertungen
- Diuretics Pharmacology 79 88Dokument6 SeitenDiuretics Pharmacology 79 88Neha RoyNoch keine Bewertungen
- Anesth ThesisDokument11 SeitenAnesth ThesisAkshay HariNoch keine Bewertungen
- Minor Periodontal Surgery in OrthoDokument6 SeitenMinor Periodontal Surgery in OrthoJuanCarlosViverosCórdovaNoch keine Bewertungen