Das könnte Ihnen auch gefallen
- Hacking for Beginners: Comprehensive Guide on Hacking Websites, Smartphones, Wireless Networks, Conducting Social Engineering, Performing a Penetration Test, and Securing Your Network (2022)Von EverandHacking for Beginners: Comprehensive Guide on Hacking Websites, Smartphones, Wireless Networks, Conducting Social Engineering, Performing a Penetration Test, and Securing Your Network (2022)Noch keine Bewertungen
- How to Write This Book!: You're going to be the author.Von EverandHow to Write This Book!: You're going to be the author.Noch keine Bewertungen
- Annexture A en Annenghsal ADokument11 SeitenAnnexture A en Annenghsal ATsakani Gift MalulekaNoch keine Bewertungen
- Annexture ADokument5 SeitenAnnexture ATsakani Gift MalulekaNoch keine Bewertungen
- Admission Booking Form, Rev. 8Dokument1 SeiteAdmission Booking Form, Rev. 8Eking InNoch keine Bewertungen
- ID Application FormsDokument5 SeitenID Application Formskez leigh AmberNoch keine Bewertungen
- Form6hs (Forelem)Dokument1 SeiteForm6hs (Forelem)dennisNoch keine Bewertungen
- F.ac FormDokument1 SeiteF.ac FormRex PatambangNoch keine Bewertungen
- Ac FormDokument1 SeiteAc FormLK DULLINNoch keine Bewertungen
- PL FormDokument1 SeitePL FormAnonymous F0AqjkNoch keine Bewertungen
- I. Applicant Information: Application For Student WorkerDokument3 SeitenI. Applicant Information: Application For Student WorkerCameronNoch keine Bewertungen
- Official Leave Request Form: For Authorized Personnel Only (Do Not Fill-Out)Dokument2 SeitenOfficial Leave Request Form: For Authorized Personnel Only (Do Not Fill-Out)Team Leader ManagementNoch keine Bewertungen
- Student Leave Application Form: International Institute of Health Management Research, New DelhiDokument1 SeiteStudent Leave Application Form: International Institute of Health Management Research, New Delhinuzi62Noch keine Bewertungen
- ZONE - Adult Release Form 2011Dokument2 SeitenZONE - Adult Release Form 2011Stephen RagsdaleNoch keine Bewertungen
- CDT 138Dokument2 SeitenCDT 138passioncadetNoch keine Bewertungen
- Claim Form AskariDokument1 SeiteClaim Form AskariTahirNoch keine Bewertungen
- 24 Hour ReportDokument2 Seiten24 Hour ReportEduardo AnerdezNoch keine Bewertungen
- 16 Regional Mid-Year Convention Waiver: Registration Proper Shall Be Charged P100.00Dokument1 Seite16 Regional Mid-Year Convention Waiver: Registration Proper Shall Be Charged P100.00AudzkieNoch keine Bewertungen
- St. Paul College Foundation, Inc. Health Services Department Referral Slip (Guidance CounselorDokument3 SeitenSt. Paul College Foundation, Inc. Health Services Department Referral Slip (Guidance CounselorAnonymous g83dcTWNoch keine Bewertungen
- Grateful Mind Enterprise: Client Information FormDokument4 SeitenGrateful Mind Enterprise: Client Information FormArman LuengoNoch keine Bewertungen
- Applicant Application FormDokument6 SeitenApplicant Application FormJocelyn Joy ArcegaNoch keine Bewertungen
- Billing Account FormDokument1 SeiteBilling Account FormGubat District HospitalNoch keine Bewertungen
- Iv InsertionDokument1 SeiteIv InsertionLlys MondejarNoch keine Bewertungen
- Validation Report FormDokument2 SeitenValidation Report FormSansie Joy ManuelNoch keine Bewertungen
- CRM Shopping Centre Liability Insurance Questionnaire: AFS Licence 246622Dokument4 SeitenCRM Shopping Centre Liability Insurance Questionnaire: AFS Licence 246622sanaabougNoch keine Bewertungen
- Application To Rent GL FormDokument2 SeitenApplication To Rent GL Formgeorgelange100% (2)
- Forms LRDokument1 SeiteForms LRRickNoch keine Bewertungen
- 2023 PROJECT COOL BREEZE ApplicationDokument1 Seite2023 PROJECT COOL BREEZE ApplicationLive 5 News100% (3)
- Motor Claim Form TheftDokument2 SeitenMotor Claim Form TheftSai PrasanthNoch keine Bewertungen
- Purchase-Order-Form SampleDokument1 SeitePurchase-Order-Form SampleArmie Jay Dela Cruz100% (1)
- POSTGRADUATEAPPLICATIONDokument6 SeitenPOSTGRADUATEAPPLICATIONRamin Le MiexNoch keine Bewertungen
- Co Signers Statement2Dokument1 SeiteCo Signers Statement2Pharmastar Int'l Trading Corp.Noch keine Bewertungen
- Breakdown of Wages: Deductions Breakdown of Wages: DeductionsDokument3 SeitenBreakdown of Wages: Deductions Breakdown of Wages: DeductionsDONANoch keine Bewertungen
- Medical Claim Form (Reimbursement Only)Dokument2 SeitenMedical Claim Form (Reimbursement Only)Muhammad Rizwan Tariq100% (1)
- Fax To: Email To: 415-449-3446: Customer Statement of Disputed TransactionDokument2 SeitenFax To: Email To: 415-449-3446: Customer Statement of Disputed TransactionbugzyNoch keine Bewertungen
- Individual Bond ApplicationDokument1 SeiteIndividual Bond ApplicationMarriane Sapitan FlorentinoNoch keine Bewertungen
- FORM 1 - SCC - StatementOfClaimDokument2 SeitenFORM 1 - SCC - StatementOfClaimMarko LopezNoch keine Bewertungen
- Application FormDokument2 SeitenApplication FormJuan LucioNoch keine Bewertungen
- SlipDokument10 SeitenSlipbascula2.pgciNoch keine Bewertungen
- Annual Leave/Vacation Request Form: Signature Over Printed Name Signature Over Printed Name Signature Over Printed NameDokument1 SeiteAnnual Leave/Vacation Request Form: Signature Over Printed Name Signature Over Printed Name Signature Over Printed NamechristianNoch keine Bewertungen
- Emergency Loan ApplicationDokument1 SeiteEmergency Loan ApplicationecyandocNoch keine Bewertungen
- Cord CareDokument1 SeiteCord CareLlys MondejarNoch keine Bewertungen
- ANECDOTALDokument6 SeitenANECDOTALZeporah OrdonNoch keine Bewertungen
- Leave Form ApplicationDokument1 SeiteLeave Form ApplicationCB MARINE PRODUCTSNoch keine Bewertungen
- SICI Cosigner's StatementDokument2 SeitenSICI Cosigner's StatementFei XiaoNoch keine Bewertungen
- Confidential Academic Evaluation Form: Page 1 of 2Dokument2 SeitenConfidential Academic Evaluation Form: Page 1 of 2annelle0219100% (1)
- Annex A - LCS Request For AppointmentDokument2 SeitenAnnex A - LCS Request For Appointmentlei inciongNoch keine Bewertungen
- Adverse Anaesthesia Event FormDokument2 SeitenAdverse Anaesthesia Event FormHarsh100% (1)
- Delivery Slip For Actual Cases: Republic of The Philippines University of Northern Philippines Vigan CityDokument1 SeiteDelivery Slip For Actual Cases: Republic of The Philippines University of Northern Philippines Vigan CityEdelyn FieldadNoch keine Bewertungen
- Day Care / Homebased Monthly Progress Report: For The Month of - 20Dokument2 SeitenDay Care / Homebased Monthly Progress Report: For The Month of - 20adoptifyNoch keine Bewertungen
- SEED Application FormDokument4 SeitenSEED Application FormTeasha Nika PetersNoch keine Bewertungen
- Issue of Duplicate Share CertificatesDokument5 SeitenIssue of Duplicate Share CertificatesMurali KrishnaNoch keine Bewertungen
- Permission To Administer MedicationDokument2 SeitenPermission To Administer MedicationKaify JamilNoch keine Bewertungen
- Employment AppDokument4 SeitenEmployment Appapi-306956549Noch keine Bewertungen
- Biodata Revised As of 11.5.18Dokument1 SeiteBiodata Revised As of 11.5.18S3 INSURANCENoch keine Bewertungen
- Checklist For InspectionDokument1 SeiteChecklist For InspectionYhenzyOj BeatingNoch keine Bewertungen
- Claim FormDokument1 SeiteClaim FormAziz Ahmad0% (1)
- Nurse Process RecordingDokument3 SeitenNurse Process Recordingmmcgee002100% (4)
- Form For Change of Biographical Details at SecDokument1 SeiteForm For Change of Biographical Details at SecSinothile ZondiNoch keine Bewertungen
- Lic402. Surety BondDokument1 SeiteLic402. Surety BondBONDCK88507Noch keine Bewertungen
- 6.1 Government of Pakistan's Treasury Bills: PeriodsDokument13 Seiten6.1 Government of Pakistan's Treasury Bills: PeriodsKidsNoch keine Bewertungen
- Cognos LearningDokument12 SeitenCognos LearningsygladiatorNoch keine Bewertungen
- Leaflet Lokotrack - st4.8 Product - Spread 4524 12 21 en Agg HiresDokument2 SeitenLeaflet Lokotrack - st4.8 Product - Spread 4524 12 21 en Agg Hiresjadan tupuaNoch keine Bewertungen
- United Nations Organization Irrevocable Payment OrderDokument1 SeiteUnited Nations Organization Irrevocable Payment OrderYuenNoch keine Bewertungen
- Housing Architecture: Literature Case StudiesDokument4 SeitenHousing Architecture: Literature Case StudiesJennifer PaulNoch keine Bewertungen
- 4512 152 76612Dokument32 Seiten4512 152 76612Yolanda PeñaNoch keine Bewertungen
- Ang Mundo Sa Mata NG Isang Ofw: Camarines Sur Polytechnic CollegesDokument3 SeitenAng Mundo Sa Mata NG Isang Ofw: Camarines Sur Polytechnic CollegesLuna KimNoch keine Bewertungen
- Economics 1st Edition Acemoglu Solutions ManualDokument17 SeitenEconomics 1st Edition Acemoglu Solutions Manualkennethluongwetwu2100% (25)
- Money MarketDokument67 SeitenMoney MarketAvinash Veerendra TakNoch keine Bewertungen
- Cordova, Monique C. BSA 4-1Dokument4 SeitenCordova, Monique C. BSA 4-1Mon CuiNoch keine Bewertungen
- F15F16Dokument1 SeiteF15F16MinamPeruNoch keine Bewertungen
- I. Balance Sheet DEC 31ST, 2014 DEC 31ST, 2015Dokument1 SeiteI. Balance Sheet DEC 31ST, 2014 DEC 31ST, 2015WawerudasNoch keine Bewertungen
- IOCL Oct-22 GPTDokument1 SeiteIOCL Oct-22 GPTV.S.SharmaNoch keine Bewertungen
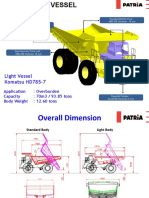
- Patria Light Vessel HD 785-7Dokument9 SeitenPatria Light Vessel HD 785-7bayu enasoraNoch keine Bewertungen
- 0Dokument5 Seiten0Nicco Ortiz50% (2)
- Electronic Challan .1.9Dokument27 SeitenElectronic Challan .1.9Soumya BisoiNoch keine Bewertungen
- The Philippine Administrative SystemDokument10 SeitenThe Philippine Administrative SystemDan YuNoch keine Bewertungen
- Siemens CDODokument2 SeitenSiemens CDOkmuiccNoch keine Bewertungen
- Endless BountyDokument14 SeitenEndless BountyAnonymous C0q7LDwSNoch keine Bewertungen
- CS Harley - May 2013Dokument16 SeitenCS Harley - May 2013Neil CalvinNoch keine Bewertungen
- Trainers Manual For Sustainable Cocoa GhanaDokument199 SeitenTrainers Manual For Sustainable Cocoa GhanaKookoase Krakye100% (1)
- Social Innovation Camp - A Toolkit For TroublemakersDokument26 SeitenSocial Innovation Camp - A Toolkit For TroublemakersUNDP in Europe and Central Asia100% (1)
- BRAC Bank Limited - Cards P@y Flex ProgramDokument3 SeitenBRAC Bank Limited - Cards P@y Flex Programaliva78100% (2)
- QTN No 213468Dokument4 SeitenQTN No 213468ZakNoch keine Bewertungen
- Forbo Marmoleum Click Techn - Specs PDFDokument1 SeiteForbo Marmoleum Click Techn - Specs PDFDoutor InácioNoch keine Bewertungen
- Foreign Trade Policy 2009-2014Dokument112 SeitenForeign Trade Policy 2009-2014shruti_siNoch keine Bewertungen
- Macedonian Diplomatic Bulletin No. 51-52Dokument16 SeitenMacedonian Diplomatic Bulletin No. 51-52Republic of Macedonia - Ministry of Foreign AffairsNoch keine Bewertungen
- Conversations in Colombia, S. Gudeman and A. RiveraDokument217 SeitenConversations in Colombia, S. Gudeman and A. RiveraAnonymous OeCloZYzNoch keine Bewertungen
- 미국 회계 용어Dokument20 Seiten미국 회계 용어jenifferNoch keine Bewertungen
- Clemente v. Court of AppealsDokument1 SeiteClemente v. Court of AppealsAnjNoch keine Bewertungen