Das könnte Ihnen auch gefallen
- Mccee 1992Dokument10 SeitenMccee 1992Sina JamNama100% (1)
- PLAB Part I Practice Paper 2Dokument22 SeitenPLAB Part I Practice Paper 2khamedNoch keine Bewertungen
- PLAB Part I Paper July 2002 PDFDokument12 SeitenPLAB Part I Paper July 2002 PDFAarif RanaNoch keine Bewertungen
- Fractures: Dr. Pradeep Fernando MS, FRCSDokument31 SeitenFractures: Dr. Pradeep Fernando MS, FRCSrikarzNoch keine Bewertungen
- Lecture LBDokument14 SeitenLecture LBrikarzNoch keine Bewertungen
- Postintern15 07 2014letterDokument2 SeitenPostintern15 07 2014letterrikarzNoch keine Bewertungen
- Hydrocephalus NewDokument21 SeitenHydrocephalus NewrikarzNoch keine Bewertungen
- 01 Pathophysiology & MX of PainDokument37 Seiten01 Pathophysiology & MX of PainrikarzNoch keine Bewertungen
- Management of Nephrotic Syndrome in ChildrenDokument16 SeitenManagement of Nephrotic Syndrome in ChildrensivaNoch keine Bewertungen
- 06.osteoarthritis PradeepDokument29 Seiten06.osteoarthritis PradeeprikarzNoch keine Bewertungen
- ABC TraumaDokument27 SeitenABC TraumarikarzNoch keine Bewertungen
- 04.infections of Bone and JointDokument17 Seiten04.infections of Bone and JointrikarzNoch keine Bewertungen
- An Approach To The Problem of Low Back PainDokument35 SeitenAn Approach To The Problem of Low Back PainrikarzNoch keine Bewertungen
- 04.management of TumoursDokument25 Seiten04.management of TumoursrikarzNoch keine Bewertungen
- Fluid and Electrolyte TherapyDokument39 SeitenFluid and Electrolyte TherapyrikarzNoch keine Bewertungen
- 04.infections of Bone and JointDokument17 Seiten04.infections of Bone and JointrikarzNoch keine Bewertungen
- An Approach To The Problem of Low Back PainDokument35 SeitenAn Approach To The Problem of Low Back PainrikarzNoch keine Bewertungen
- Thrombocytopenia: DR Chamilka JayasingheDokument31 SeitenThrombocytopenia: DR Chamilka JayasingherikarzNoch keine Bewertungen
- Fluid and Electrolyte TherapyDokument39 SeitenFluid and Electrolyte TherapyrikarzNoch keine Bewertungen
- Management of Gastroenteritis in ChildrenDokument14 SeitenManagement of Gastroenteritis in ChildrenrikarzNoch keine Bewertungen
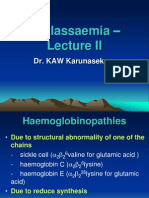
- Thalassaemia - : Dr. KAW KarunasekeraDokument36 SeitenThalassaemia - : Dr. KAW KarunasekerarikarzNoch keine Bewertungen
- 04 Toxic GasesDokument30 Seiten04 Toxic GasesrikarzNoch keine Bewertungen
- Management of Gastroenteritis in ChildrenDokument14 SeitenManagement of Gastroenteritis in ChildrenrikarzNoch keine Bewertungen
- Management of Nephrotic Syndrome in ChildrenDokument16 SeitenManagement of Nephrotic Syndrome in ChildrensivaNoch keine Bewertungen
- Breast FeedingDokument6 SeitenBreast Feedingmaykamen2Noch keine Bewertungen
- Management of A Febrile ChildDokument9 SeitenManagement of A Febrile ChildsivaNoch keine Bewertungen
- Management of Paediatric EmergenciesDokument56 SeitenManagement of Paediatric EmergenciesrikarzNoch keine Bewertungen
- Management of Seizures in ChildrenDokument26 SeitenManagement of Seizures in ChildrenrikarzNoch keine Bewertungen
- Management of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinDokument7 SeitenManagement of Patients With Nephrotic Syndrome: Sophie de Seigneux, Pierre-Yves MartinGarit Hapsari KiranaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Clinical Teams Mental Health ManualDokument18 SeitenClinical Teams Mental Health Manualapi-609422028Noch keine Bewertungen
- 1community Health NursingDokument27 Seiten1community Health NursingAsal SalahNoch keine Bewertungen
- Updated Resume 11 19Dokument2 SeitenUpdated Resume 11 19api-454845978Noch keine Bewertungen
- Voh 11Dokument19 SeitenVoh 11Siphiwe Christopher MathebulaNoch keine Bewertungen
- Seasonal CalendarDokument5 SeitenSeasonal CalendarVdrpkNoch keine Bewertungen
- Task-1 LO-1: Company BackgroundDokument20 SeitenTask-1 LO-1: Company BackgroundDuaa AsjadNoch keine Bewertungen
- Epidemiological Study of Scabies Among School Children PDFDokument8 SeitenEpidemiological Study of Scabies Among School Children PDFnoman IOBMNoch keine Bewertungen
- An Evidence Based Case Study To Identify The Role of Bothrops Lanceolatus As A Homeopathic AnticoagulantDokument6 SeitenAn Evidence Based Case Study To Identify The Role of Bothrops Lanceolatus As A Homeopathic AnticoagulantEditor IJTSRDNoch keine Bewertungen
- Barriers To Health Technology AssessmentDokument8 SeitenBarriers To Health Technology AssessmentHilton D. CalawenNoch keine Bewertungen
- Lesson 1 The Stuart Stress Adaptation ModelDokument50 SeitenLesson 1 The Stuart Stress Adaptation ModelMaria Victoria A. PraxidesNoch keine Bewertungen
- DSWD Programs and ServicesDokument12 SeitenDSWD Programs and ServicesKathryn Krystal R Lanuza100% (2)
- Teaching Philosophy Assignment Patricia AnyasoDokument6 SeitenTeaching Philosophy Assignment Patricia Anyasoodunze1Noch keine Bewertungen
- SOPDokument2 SeitenSOPNIGEL SAANANoch keine Bewertungen
- 4f4f3d97-3c1c-49d9-8f67-7c1bd1d9f142Dokument416 Seiten4f4f3d97-3c1c-49d9-8f67-7c1bd1d9f142AhmedNadeemNoch keine Bewertungen
- MCN FINALS MergedDokument193 SeitenMCN FINALS MergedNeru RoriNoch keine Bewertungen
- HallucinationDokument16 SeitenHallucinationirmaNoch keine Bewertungen
- Jospt 2021 10199Dokument4 SeitenJospt 2021 10199Jacinta SeguraNoch keine Bewertungen
- Covid Vaccinbe BibDokument2 SeitenCovid Vaccinbe Bibapi-549087954Noch keine Bewertungen
- Newcastle - Ottawa Quality Assessment Scale Adapted For Cross-Sectional/ Case-Control Studies Review: Chronic Pain and EEG PatternsDokument1 SeiteNewcastle - Ottawa Quality Assessment Scale Adapted For Cross-Sectional/ Case-Control Studies Review: Chronic Pain and EEG PatternsCamilaNoch keine Bewertungen
- NCMA112: History of Health EducationDokument11 SeitenNCMA112: History of Health EducationAngelica LegaspiNoch keine Bewertungen
- Laporan Persediaan Agustus 2022Dokument11 SeitenLaporan Persediaan Agustus 2022nurulNoch keine Bewertungen
- Super Top Up Health Plan IIMKAADokument3 SeitenSuper Top Up Health Plan IIMKAAcharankviNoch keine Bewertungen
- MD Microbiology Dissertation TopicsDokument8 SeitenMD Microbiology Dissertation TopicsWriteMyPaperCheapUK100% (1)
- FNP ResumeDokument4 SeitenFNP Resumeapi-569838480Noch keine Bewertungen
- Julie Matthews Practical Nutrition Steps To Better Health Learning BehaviorDokument10 SeitenJulie Matthews Practical Nutrition Steps To Better Health Learning BehaviorAlina MilitaruNoch keine Bewertungen
- Case Study Report EnterprenshipDokument6 SeitenCase Study Report EnterprenshipTedros BelaynehNoch keine Bewertungen
- Drug and Alcohol Awareness ClassDokument71 SeitenDrug and Alcohol Awareness ClassRinkish DalliahNoch keine Bewertungen
- Removing Gallstones NaturallyDokument113 SeitenRemoving Gallstones NaturallyCorinne Cinco-Cadavis0% (1)
- Assessment Questions (Assessment Criteria)Dokument2 SeitenAssessment Questions (Assessment Criteria)sujanaNoch keine Bewertungen