Das könnte Ihnen auch gefallen
- Platelet Protocols: Research and Clinical Laboratory ProceduresVon EverandPlatelet Protocols: Research and Clinical Laboratory ProceduresNoch keine Bewertungen
- Effect of Anesthesia on Liver Function and HemostasisDokument7 SeitenEffect of Anesthesia on Liver Function and Hemostasiswulan reksa fortunaNoch keine Bewertungen
- Edema ParuDokument4 SeitenEdema ParuSri BayaniNoch keine Bewertungen
- MCQ SDokument7 SeitenMCQ Syousef.mohammed1015Noch keine Bewertungen
- OK - Modul Ortho - Bone Cement Implantation SyndromeDokument18 SeitenOK - Modul Ortho - Bone Cement Implantation SyndromeWanditoGayuhUtomoNoch keine Bewertungen
- Anesthetic Management For Laparoscopic Cholecystectomy: Somchai AmornyotinDokument10 SeitenAnesthetic Management For Laparoscopic Cholecystectomy: Somchai AmornyotinAidaDesNoch keine Bewertungen
- Daniel Chappell, Matthias Jacob, Oliver Paul, Laurenz Mehringer, Walter Newman and Bernhard Friedrich BeckerDokument2 SeitenDaniel Chappell, Matthias Jacob, Oliver Paul, Laurenz Mehringer, Walter Newman and Bernhard Friedrich BeckerShamini ShanmugalingamNoch keine Bewertungen
- Bleeding Complications Aw C BypassDokument18 SeitenBleeding Complications Aw C BypassPruthvi RajNoch keine Bewertungen
- Vasoplegic SyndromeDokument41 SeitenVasoplegic SyndromeFaizan Ahmad Ali100% (1)
- 3-Classification of Noreflow PhenomenonDokument4 Seiten3-Classification of Noreflow PhenomenonMohamed KhattabNoch keine Bewertungen
- Moreau Et Al. - 2023 - The Use of Induced Hypothermia in Extracorporeal MDokument13 SeitenMoreau Et Al. - 2023 - The Use of Induced Hypothermia in Extracorporeal Mgavain.ferronsNoch keine Bewertungen
- PIIS0733862720300729Dokument15 SeitenPIIS0733862720300729Hames SeguraNoch keine Bewertungen
- Arterial Tourniquets Anaesthesia Tutorial of The Week 200 11 OCTOBER 2010Dokument7 SeitenArterial Tourniquets Anaesthesia Tutorial of The Week 200 11 OCTOBER 2010tessalaiNoch keine Bewertungen
- Anti CoagulationDokument16 SeitenAnti Coagulationwragnor rosNoch keine Bewertungen
- Mix TestsDokument3 SeitenMix Testsmoisabel acevedoNoch keine Bewertungen
- Vasoplegic Syndrome Following Cardiothoracic Surgery-Review of Pathophysiology and Update of Treatment Options - PMCDokument21 SeitenVasoplegic Syndrome Following Cardiothoracic Surgery-Review of Pathophysiology and Update of Treatment Options - PMCluis orlando bustamante rojasNoch keine Bewertungen
- File HDokument40 SeitenFile HFauzan Mahfuzh MashudiNoch keine Bewertungen
- Chest Disfuncion Pulmonar Despues QX - CVDokument9 SeitenChest Disfuncion Pulmonar Despues QX - CVCarmen HerediaNoch keine Bewertungen
- Pathogenesis FinalDokument23 SeitenPathogenesis FinalpvsvrNoch keine Bewertungen
- AHA Nefropatia Por ContrasteDokument12 SeitenAHA Nefropatia Por ContrasteDenisse Tinajero SánchezNoch keine Bewertungen
- Muscle and Trigger PointDokument1 SeiteMuscle and Trigger PointAdelinaPanaetNoch keine Bewertungen
- Background: EtiologyDokument5 SeitenBackground: Etiologylia lykimNoch keine Bewertungen
- The Pathophysiology of Aortic Cross Clamping 2016 Best Practice Research Clinical AnaesthesiologyDokument13 SeitenThe Pathophysiology of Aortic Cross Clamping 2016 Best Practice Research Clinical AnaesthesiologyPablo Garay LilloNoch keine Bewertungen
- Meccanical SupportDokument19 SeitenMeccanical SupportAttilio Del RossoNoch keine Bewertungen
- Effects of Vasopressin in Septic Shock: Case StudyDokument7 SeitenEffects of Vasopressin in Septic Shock: Case Studyns_karaniaNoch keine Bewertungen
- Overview of Hemostasis and ThrombosisDokument12 SeitenOverview of Hemostasis and ThrombosisMichaella AlmirahNoch keine Bewertungen
- Practica 2 Fletcher-Sandersjööa A. Is COVID-19 Associated Thrombosis - ComplementoDokument7 SeitenPractica 2 Fletcher-Sandersjööa A. Is COVID-19 Associated Thrombosis - Complementogenne222 solanoNoch keine Bewertungen
- What Is The Mechanism of Flow-Mediated Arterial DilatationDokument6 SeitenWhat Is The Mechanism of Flow-Mediated Arterial Dilatationhassenesalam18Noch keine Bewertungen
- Coagulopathy SepsisDokument12 SeitenCoagulopathy SepsismariaagustinaswNoch keine Bewertungen
- сократимость томскDokument8 Seitenсократимость томскepgNoch keine Bewertungen
- Circulatory DisordersDokument60 SeitenCirculatory DisordersBrhanu belayNoch keine Bewertungen
- Essentials of Anticoagulation in Hemodialysis: Core CurriculumDokument12 SeitenEssentials of Anticoagulation in Hemodialysis: Core CurriculumKavidu KeshanNoch keine Bewertungen
- Basics of ECMO Part 2Dokument6 SeitenBasics of ECMO Part 2corinna.ongaigui.gsbmNoch keine Bewertungen
- Management of Shock in TraumaDokument4 SeitenManagement of Shock in TraumaVictor Manuel Gutierrez AraujoNoch keine Bewertungen
- Dresetal Weaningthecardiacpatient COCC2014Dokument9 SeitenDresetal Weaningthecardiacpatient COCC2014JorgeNoch keine Bewertungen
- History, Indications, and Complications of ECMODokument6 SeitenHistory, Indications, and Complications of ECMOYasmin AbdelmajiedNoch keine Bewertungen
- No-Reflow Phenomenon: DR - Surinder S HansraDokument17 SeitenNo-Reflow Phenomenon: DR - Surinder S HansrasshansraNoch keine Bewertungen
- Question BankDokument6 SeitenQuestion Bankkoang lual gachNoch keine Bewertungen
- Massive TransfusionDokument75 SeitenMassive TransfusionGetaye SimachewNoch keine Bewertungen
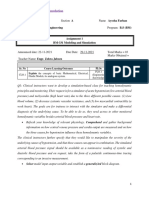
- Assignment 1 BM-331 Modeling and SimulationDokument6 SeitenAssignment 1 BM-331 Modeling and SimulationeraNoch keine Bewertungen
- Controlled Hypotensive AnesthesiaDokument24 SeitenControlled Hypotensive AnesthesiaSuresh Kumar100% (1)
- GP Exam Compiled 1st BiDokument136 SeitenGP Exam Compiled 1st BiCherry RahimaNoch keine Bewertungen
- 2018 Cardiovascular Failure and WeaningDokument10 Seiten2018 Cardiovascular Failure and WeaningftclaudioalbuquerqueNoch keine Bewertungen
- Disseminated Intravascular Coagulopathy DICDokument24 SeitenDisseminated Intravascular Coagulopathy DICMassimiliano MalerbaNoch keine Bewertungen
- Minimizing Catecholamines and Optimizing PerfusionDokument7 SeitenMinimizing Catecholamines and Optimizing PerfusionClaudia Nicol Navarrete CastagnoliNoch keine Bewertungen
- Coagulation Disorders in ICUDokument72 SeitenCoagulation Disorders in ICUMadhusudan H C Gowda100% (1)
- Dr AdeelDokument31 SeitenDr Adeelphilipswright74Noch keine Bewertungen
- Thorax 2003 Lordan 814 9Dokument7 SeitenThorax 2003 Lordan 814 9Ari KuncoroNoch keine Bewertungen
- Acute Renal Failure and Sepsis: Review ArticleDokument11 SeitenAcute Renal Failure and Sepsis: Review Articlehemer6666986Noch keine Bewertungen
- Chapter 4 - Cardiac Surgical PharmacologyDokument38 SeitenChapter 4 - Cardiac Surgical PharmacologybunzaiNoch keine Bewertungen
- COAgulopatia en TraumaDokument10 SeitenCOAgulopatia en TraumaDARWIN LUNANoch keine Bewertungen
- Chapter 1: ECMO: History and DevelopmentDokument6 SeitenChapter 1: ECMO: History and DevelopmentYasmin AbdelmajiedNoch keine Bewertungen
- Thrombolytic TherapyDokument37 SeitenThrombolytic TherapySani sunilNoch keine Bewertungen
- Permeability Role of Protein Kinase C in Bradykinin-Induced Increases in MicrovascularDokument10 SeitenPermeability Role of Protein Kinase C in Bradykinin-Induced Increases in MicrovasculararibniminnakNoch keine Bewertungen
- Advances in Understanding Ischemic Acute Kidney Injury: Minireview Open AccessDokument6 SeitenAdvances in Understanding Ischemic Acute Kidney Injury: Minireview Open AccessJack AukiónNoch keine Bewertungen
- Hemorrhagic Shock FixDokument21 SeitenHemorrhagic Shock FixNurul Rezki Fitriani AzisNoch keine Bewertungen
- Pembimbing: Dr. R. Vito Mahendra E, M.Si Med, SP.B M. Adri Kurniawan 30101306981Dokument31 SeitenPembimbing: Dr. R. Vito Mahendra E, M.Si Med, SP.B M. Adri Kurniawan 30101306981Adek AhmadNoch keine Bewertungen
- Neurogenic Pulmonary Edema - StatPearls - NCBI BookshelfDokument1 SeiteNeurogenic Pulmonary Edema - StatPearls - NCBI Bookshelfkud4l14rNoch keine Bewertungen
- Contusions May Coalesce To Form An Intracerebral Hematoma. TBI/ICH - HTMLDokument17 SeitenContusions May Coalesce To Form An Intracerebral Hematoma. TBI/ICH - HTMLEsterida SimanjuntakNoch keine Bewertungen
- Path Physiologies of The Cardiovascular SystemDokument34 SeitenPath Physiologies of The Cardiovascular Systemmara5140Noch keine Bewertungen
- Bone Cement Implantation SyndromeDokument5 SeitenBone Cement Implantation SyndromeBagas WidhiarsoNoch keine Bewertungen
- JurnalDokument4 SeitenJurnalBagas WidhiarsoNoch keine Bewertungen
- ReferencesDokument2 SeitenReferencesBagas WidhiarsoNoch keine Bewertungen
- Contact Person Draft RevisiDokument3 SeitenContact Person Draft RevisiBagas WidhiarsoNoch keine Bewertungen
- Log Book Hand Peb 17Dokument6 SeitenLog Book Hand Peb 17Bagas WidhiarsoNoch keine Bewertungen
- OTA Open Fracture ClassificationDokument1 SeiteOTA Open Fracture ClassificationPanda PavNoch keine Bewertungen
- Ankle Fracture Treatment OptionsDokument19 SeitenAnkle Fracture Treatment OptionsBagas WidhiarsoNoch keine Bewertungen
- Log Book MST November 2016Dokument5 SeitenLog Book MST November 2016Bagas WidhiarsoNoch keine Bewertungen
- LOG BOOK OPERASI STASE HAND JANUARI 2017 , DR TITO SUMARWOTO, Sp.OT (KDokument6 SeitenLOG BOOK OPERASI STASE HAND JANUARI 2017 , DR TITO SUMARWOTO, Sp.OT (KBagas WidhiarsoNoch keine Bewertungen
- A Case of Pulmonary Metastasis of Recurrent Giant Cell Tumor of BoneDokument1 SeiteA Case of Pulmonary Metastasis of Recurrent Giant Cell Tumor of BoneBagas WidhiarsoNoch keine Bewertungen
- Phalanx FractureDokument46 SeitenPhalanx FractureBagas WidhiarsoNoch keine Bewertungen
- Log Book Operasi Mei16Dokument2 SeitenLog Book Operasi Mei16Bagas WidhiarsoNoch keine Bewertungen
- 97042.15metatarsals S95 S98Dokument4 Seiten97042.15metatarsals S95 S98Bagas WidhiarsoNoch keine Bewertungen
- ACJointQx IMANAJKDokument11 SeitenACJointQx IMANAJKBagas WidhiarsoNoch keine Bewertungen
- 1043apdf SfjdasfhsdDokument8 Seiten1043apdf SfjdasfhsdBagas WidhiarsoNoch keine Bewertungen
- DASH (Disabilities of The Arm, Shoulder and Hand)Dokument3 SeitenDASH (Disabilities of The Arm, Shoulder and Hand)Chriss ChristinaNoch keine Bewertungen
- 97042.1TOC I IVDokument4 Seiten97042.1TOC I IVBagas WidhiarsoNoch keine Bewertungen
- Weaver Dunn ProcedureDokument3 SeitenWeaver Dunn ProcedureBagas WidhiarsoNoch keine Bewertungen
- Tibial HemimeliaDokument2 SeitenTibial HemimeliaBagas WidhiarsoNoch keine Bewertungen
- OTA Open Fracture ClassificationDokument1 SeiteOTA Open Fracture ClassificationPanda PavNoch keine Bewertungen
- PETA PASIEN BEDAH ANAK Rabu 24 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafDokument1 SeitePETA PASIEN BEDAH ANAK Rabu 24 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafBagas WidhiarsoNoch keine Bewertungen
- Peta Pasien Bedah Anak Sabtu 20 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafDokument1 SeitePeta Pasien Bedah Anak Sabtu 20 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafBagas WidhiarsoNoch keine Bewertungen
- SELESAI The EndDokument1 SeiteSELESAI The EndBagas WidhiarsoNoch keine Bewertungen
- Mapping Bedah Anak 170914Dokument1 SeiteMapping Bedah Anak 170914Bagas WidhiarsoNoch keine Bewertungen
- Radial RadialisDokument1 SeiteRadial RadialisBagas WidhiarsoNoch keine Bewertungen
- SELESAI The EndDokument1 SeiteSELESAI The EndBagas WidhiarsoNoch keine Bewertungen
- PETA PASIEN BEDAH ANAK Jumat 26 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafDokument1 SeitePETA PASIEN BEDAH ANAK Jumat 26 September 2014 BGSL Bed Nama Umur CM Mrs Diagnosa OP STT S Plan Ket Lab StafBagas WidhiarsoNoch keine Bewertungen
- Seminar & Workshop Total Hip Arthroplasty: Skill Lab Rso Prof DR R Soeharso Sabtu, 1 November 2014Dokument1 SeiteSeminar & Workshop Total Hip Arthroplasty: Skill Lab Rso Prof DR R Soeharso Sabtu, 1 November 2014Bagas WidhiarsoNoch keine Bewertungen
- Optician ChartDokument5 SeitenOptician ChartBagas WidhiarsoNoch keine Bewertungen
- Photosensitizing Agents and Their Applications in PhototherapyDokument26 SeitenPhotosensitizing Agents and Their Applications in PhototherapyMagesh SNoch keine Bewertungen
- Rapyuta Robotics PVT LTD - GMC Renewal Quote - 28th Dec2022Dokument1 SeiteRapyuta Robotics PVT LTD - GMC Renewal Quote - 28th Dec2022nagarajgnairyNoch keine Bewertungen
- 16 Feb Afternoon - MedicineDokument13 Seiten16 Feb Afternoon - MedicineDrToby KhanNoch keine Bewertungen
- 2024 - ĐỀ 4Dokument10 Seiten2024 - ĐỀ 4ellypham1357Noch keine Bewertungen
- Dimension Exl 200 Tech SpecsDokument2 SeitenDimension Exl 200 Tech SpecsOo Kenx OoNoch keine Bewertungen
- GASTROINTESTINAL DRUGS FOR ULCERS AND REFLUXDokument11 SeitenGASTROINTESTINAL DRUGS FOR ULCERS AND REFLUXRhealyn LegaspiNoch keine Bewertungen
- Neuromuscular Therapy Techniques for Stroke and MS RehabilitationDokument11 SeitenNeuromuscular Therapy Techniques for Stroke and MS RehabilitationWenzy Razzie cruzNoch keine Bewertungen
- NEET Biology Through MCQDokument587 SeitenNEET Biology Through MCQAnanth Dharanidharan100% (1)
- Hepatitis B: Submitted To: DR Gul Shahnaz Presenter: Sameen Abbas M.Phil 2 SemesterDokument28 SeitenHepatitis B: Submitted To: DR Gul Shahnaz Presenter: Sameen Abbas M.Phil 2 SemesterNaina MehmoodNoch keine Bewertungen
- CRH Radiology Policies and ProceduresDokument60 SeitenCRH Radiology Policies and ProceduresAbdul Saeed Shah100% (1)
- TS Report en WebdownloadDokument175 SeitenTS Report en WebdownloadMartin NardoNoch keine Bewertungen
- Salivation PDFDokument5 SeitenSalivation PDFmehdi mafakheri100% (1)
- SEMINAR-Clinical Microbiology: Topic-Human Immuno-Deficiency Virus (HIV)Dokument54 SeitenSEMINAR-Clinical Microbiology: Topic-Human Immuno-Deficiency Virus (HIV)sushant_dharNoch keine Bewertungen
- Medicine in Allen: Sensitive TouchDokument38 SeitenMedicine in Allen: Sensitive TouchAyeshik ChakrabortyNoch keine Bewertungen
- Book Eczema PsoriazisDokument457 SeitenBook Eczema Psoriazisdaniel bNoch keine Bewertungen
- Pharmacology ReviewerDokument21 SeitenPharmacology ReviewerCzairalene QuinzonNoch keine Bewertungen
- Faecal AnalysisDokument83 SeitenFaecal AnalysisJoseph SabidoNoch keine Bewertungen
- Borderline Personality Disorder, Bipolar Disorder, Depression, Attention ... Narcissistic Personality Disorder, Diferential Diagnostic, KernbergDokument23 SeitenBorderline Personality Disorder, Bipolar Disorder, Depression, Attention ... Narcissistic Personality Disorder, Diferential Diagnostic, KernbergjuaromerNoch keine Bewertungen
- Nettle Rash Symptoms, Causes, TreatmentDokument2 SeitenNettle Rash Symptoms, Causes, TreatmentArdave Laurente100% (1)
- Dementia Presentation Feb 19Dokument28 SeitenDementia Presentation Feb 19Rhu Pugo, La UnionNoch keine Bewertungen
- Prestigi0us BiochemistryDokument30 SeitenPrestigi0us Biochemistrybovey69015Noch keine Bewertungen
- A Novel Technique For Pudendal Nerve BlockDokument4 SeitenA Novel Technique For Pudendal Nerve Blockmohs2007100% (1)
- Health Promotion and Disease Prevention in the ElderlyDokument1 SeiteHealth Promotion and Disease Prevention in the ElderlyBeverly PagcaliwaganNoch keine Bewertungen
- CPT ComprehensiveDokument14 SeitenCPT Comprehensivesha100% (1)
- Indian Herbs Cooking GuideDokument37 SeitenIndian Herbs Cooking Guidehitesh mendirattaNoch keine Bewertungen
- Plant Based Diet A Way To Healthier Life: September 2020Dokument9 SeitenPlant Based Diet A Way To Healthier Life: September 2020MihryazdNoch keine Bewertungen
- Venipuncture Techniques and ProceduresDokument66 SeitenVenipuncture Techniques and ProceduresAngelica Camille B. AbaoNoch keine Bewertungen
- Male infertility evaluation: what you need to knowDokument1 SeiteMale infertility evaluation: what you need to knowa jNoch keine Bewertungen
- Asthma Lesson PlanDokument26 SeitenAsthma Lesson PlanBharat Singh BanshiwalNoch keine Bewertungen
- Uganda Participatory Poverty Assessment Report 2000Dokument193 SeitenUganda Participatory Poverty Assessment Report 2000FabioNoch keine Bewertungen
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (13)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 3.5 von 5 Sternen3.5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (402)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNoch keine Bewertungen
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 5 von 5 Sternen5/5 (78)
- Techniques Exercises And Tricks For Memory ImprovementVon EverandTechniques Exercises And Tricks For Memory ImprovementBewertung: 4.5 von 5 Sternen4.5/5 (40)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisVon EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisBewertung: 4 von 5 Sternen4/5 (1)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (169)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 5 von 5 Sternen5/5 (4)
- The Ultimate Guide To Memory Improvement TechniquesVon EverandThe Ultimate Guide To Memory Improvement TechniquesBewertung: 5 von 5 Sternen5/5 (34)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (327)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsVon EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNoch keine Bewertungen
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingVon EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingBewertung: 5 von 5 Sternen5/5 (4)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (253)
- The Happiness Trap: How to Stop Struggling and Start LivingVon EverandThe Happiness Trap: How to Stop Struggling and Start LivingBewertung: 4 von 5 Sternen4/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (41)
- The Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityVon EverandThe Stress-Proof Brain: Master Your Emotional Response to Stress Using Mindfulness and NeuroplasticityBewertung: 4.5 von 5 Sternen4.5/5 (109)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingVon EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingBewertung: 3.5 von 5 Sternen3.5/5 (33)
- The Tennis Partner: A Doctor's Story of Friendship and LossVon EverandThe Tennis Partner: A Doctor's Story of Friendship and LossBewertung: 4.5 von 5 Sternen4.5/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- Summary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisVon EverandSummary: Limitless: Upgrade Your Brain, Learn Anything Faster, and Unlock Your Exceptional Life By Jim Kwik: Key Takeaways, Summary and AnalysisBewertung: 5 von 5 Sternen5/5 (8)