Das könnte Ihnen auch gefallen
- Radiologic Management of Upper Gastrointestinal BleedingDokument13 SeitenRadiologic Management of Upper Gastrointestinal BleedingshadowlightfoxNoch keine Bewertungen
- Indeterminate Renal Mass ACR Appropriateness CriteriaDokument10 SeitenIndeterminate Renal Mass ACR Appropriateness CriteriaAndrew TaliaferroNoch keine Bewertungen
- American College of Radiology End User License AgreementDokument9 SeitenAmerican College of Radiology End User License AgreementYori PrimandaNoch keine Bewertungen
- Renal Cell Carcinoma Staging (ACR Appropriateness Criteria)Dokument10 SeitenRenal Cell Carcinoma Staging (ACR Appropriateness Criteria)Andrew TaliaferroNoch keine Bewertungen
- Renovascular HypertensionDokument11 SeitenRenovascular HypertensionJoseph GlaserNoch keine Bewertungen
- ACR Appropriateness Criteria For HematuriaDokument8 SeitenACR Appropriateness Criteria For HematuriaAndrew TaliaferroNoch keine Bewertungen
- Chylothorax Treatment PlanningDokument10 SeitenChylothorax Treatment PlanningVianney OlveraNoch keine Bewertungen
- ACR Appropriateness Criteria® Acute Chest Pain - Suspected Pulmonary Embolism.Dokument16 SeitenACR Appropriateness Criteria® Acute Chest Pain - Suspected Pulmonary Embolism.Madalina TalpauNoch keine Bewertungen
- Acute Onset Flank Pain-Suspicion of Stone DiseaseDokument9 SeitenAcute Onset Flank Pain-Suspicion of Stone DiseasecubirojasNoch keine Bewertungen
- Onset Flank PainDokument11 SeitenOnset Flank PainPipitNoch keine Bewertungen
- Infective EndocarditisDokument13 SeitenInfective Endocarditispaquidermo85Noch keine Bewertungen
- Acute Nonspecific Chest Pain-Low Probability of Coronary Artery DiseaseDokument10 SeitenAcute Nonspecific Chest Pain-Low Probability of Coronary Artery Diseasevictor contrerasNoch keine Bewertungen
- Abdominal Aortic Aneurysm Follow-Up (Without Repair)Dokument7 SeitenAbdominal Aortic Aneurysm Follow-Up (Without Repair)victor contrerasNoch keine Bewertungen
- NICE Visual Summary NSTEMI - UADokument1 SeiteNICE Visual Summary NSTEMI - UAdnasdajkdnajfkNoch keine Bewertungen
- Hematology Laboratory PDFDokument3 SeitenHematology Laboratory PDFMariel AbatayoNoch keine Bewertungen
- Ca Treatment Rectal Web AlgorithmDokument17 SeitenCa Treatment Rectal Web AlgorithmPatrick JohnNoch keine Bewertungen
- Abnormal Uterine BleedingDokument12 SeitenAbnormal Uterine Bleedingvictor contrerasNoch keine Bewertungen
- Abdominal Aortic Aneurysm-Interventional Planning and Follow-UpDokument13 SeitenAbdominal Aortic Aneurysm-Interventional Planning and Follow-Upvictor contrerasNoch keine Bewertungen
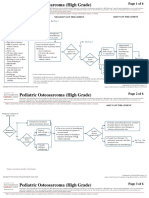
- CA Treatment Osteosarcoma Pedi Web AlgorithmDokument6 SeitenCA Treatment Osteosarcoma Pedi Web AlgorithmyaseenNoch keine Bewertungen
- Adrenal Mass EvaluationDokument19 SeitenAdrenal Mass Evaluationpj rakNoch keine Bewertungen
- Dyspnea-Suspected Cardiac Origin (Ischemia Already Excluded)Dokument20 SeitenDyspnea-Suspected Cardiac Origin (Ischemia Already Excluded)Parth PatilNoch keine Bewertungen
- Hematuria PDFDokument11 SeitenHematuria PDFPipitNoch keine Bewertungen
- Blunt Abdominal TraumaDokument11 SeitenBlunt Abdominal TraumaRahmat SyahiliNoch keine Bewertungen
- Bdzzqlji2#: LsdecrledDokument11 SeitenBdzzqlji2#: LsdecrledKoleen AggabaoNoch keine Bewertungen
- ACR Appropriateness Criteria Pancreatic CystDokument9 SeitenACR Appropriateness Criteria Pancreatic CystSole GonzalezNoch keine Bewertungen
- American College of Radiology ACR Appropriateness CriteriaDokument10 SeitenAmerican College of Radiology ACR Appropriateness CriteriaNovia ChrisnawatiNoch keine Bewertungen
- CA Treatment Leptomeningeal Web AlgorithmDokument5 SeitenCA Treatment Leptomeningeal Web Algorithmsugoiman100% (1)
- ABIM - Allergy - (Medicalstudyzone - Com)Dokument12 SeitenABIM - Allergy - (Medicalstudyzone - Com)sjcemeryNoch keine Bewertungen
- Major Blunt TraumaDokument18 SeitenMajor Blunt TraumaghassanNoch keine Bewertungen
- 374 FullDokument17 Seiten374 FullValentina MerolaNoch keine Bewertungen
- ( Û ) Questionnaire Hospital InformationDokument5 Seiten( Û ) Questionnaire Hospital InformationsjeloNoch keine Bewertungen
- Sample Chapter 9780323354783Dokument11 SeitenSample Chapter 9780323354783Mahmoud ElsheikhNoch keine Bewertungen
- AUA Guideline Testicular CancerDokument1 SeiteAUA Guideline Testicular CancerMarco Túlio La Guardia PiresNoch keine Bewertungen
- DM CHFDokument2 SeitenDM CHFSafa Abdualrahaman Ali HamadNoch keine Bewertungen
- Principles of Medical Laboratory Science: Topic 1 For Prelims (Laboratory) : Phlebotomy: EquipmentDokument10 SeitenPrinciples of Medical Laboratory Science: Topic 1 For Prelims (Laboratory) : Phlebotomy: EquipmentMaria Reyna BacomoNoch keine Bewertungen
- Occupational Lung DiseasesDokument13 SeitenOccupational Lung DiseasesVianney OlveraNoch keine Bewertungen
- 1 MONDAY Jan 31 AfternoonkkDokument5 Seiten1 MONDAY Jan 31 AfternoonkkEricka GenoveNoch keine Bewertungen
- Manejo de Riesgo de Sangrado Antes de Procedimientos InvasivosDokument17 SeitenManejo de Riesgo de Sangrado Antes de Procedimientos InvasivosAdrian CroesNoch keine Bewertungen
- EHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationDokument41 SeitenEHRA Practical Guide On The Use of New Oral Anticoagulants in Patients With Non-Valvular Atrial FibrillationAmelia Maria LasloNoch keine Bewertungen
- Oncology Table SummaryDokument4 SeitenOncology Table SummaryAiah AbenesNoch keine Bewertungen
- Journal Club TemplateDokument5 SeitenJournal Club TemplateAnonymous zyHbTsybDXNoch keine Bewertungen
- 8 - Diagnostic Challenges in SepsisDokument34 Seiten8 - Diagnostic Challenges in Sepsiskoteshwara raoNoch keine Bewertungen
- Surgery2 3 3Dokument12 SeitenSurgery2 3 3KRISJOHN PAUL D. FLORESNoch keine Bewertungen
- Low Back PainDokument10 SeitenLow Back Paindigimon666Noch keine Bewertungen
- ACD Ambulatory GI: Liver DiseaseDokument48 SeitenACD Ambulatory GI: Liver DiseaseNuthahai SimangernNoch keine Bewertungen
- Protocol PresentationDokument31 SeitenProtocol Presentationapi-527613255Noch keine Bewertungen
- Anticoagulation EndosDokument16 SeitenAnticoagulation EndosDr AhmedNoch keine Bewertungen
- Colorectal Screening AlgorithmDokument12 SeitenColorectal Screening Algorithmsavvy_as_98Noch keine Bewertungen
- Recruitment Checklist: Security Forces Hospital ProgramDokument4 SeitenRecruitment Checklist: Security Forces Hospital ProgramDerick RanaNoch keine Bewertungen
- CreaDokument5 SeitenCreaKouame Francis0% (1)
- Clinical Guideline Suspected Adrenal IncidentalomaDokument3 SeitenClinical Guideline Suspected Adrenal IncidentalomaMica SaeronNoch keine Bewertungen
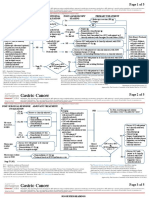
- Ca Treatment Gastric Web AlgorithmDokument5 SeitenCa Treatment Gastric Web AlgorithmEVELYN EZEKWENoch keine Bewertungen
- BSG Trainees Gastroenterology Handbook 2015Dokument32 SeitenBSG Trainees Gastroenterology Handbook 2015Afnan MaaroufNoch keine Bewertungen
- Week 5 Hematology 2 Laboratory Tests For Primary HemostasisDokument15 SeitenWeek 5 Hematology 2 Laboratory Tests For Primary HemostasisKelvssNoch keine Bewertungen
- Form Report Mcu MMS ClinicDokument4 SeitenForm Report Mcu MMS ClinicMisterB TobaNoch keine Bewertungen
- Tranexamic Acid For Lower GI HemorrhageDokument8 SeitenTranexamic Acid For Lower GI HemorrhagekarinalavianiNoch keine Bewertungen
- Table 1: Intial Evaluation On Arrival To ER For All PatientsDokument1 SeiteTable 1: Intial Evaluation On Arrival To ER For All PatientsHetoshima KeiNoch keine Bewertungen
- Diagnosis and Treatment of Early Stage Testicular Cancer: Aua Guideline AlgorithmDokument4 SeitenDiagnosis and Treatment of Early Stage Testicular Cancer: Aua Guideline Algorithmputra imanullahNoch keine Bewertungen
- Periprocedural Anticoagulation Guidelines - UKDokument14 SeitenPeriprocedural Anticoagulation Guidelines - UKjoshNoch keine Bewertungen
- Salvage Therapy for Prostate CancerVon EverandSalvage Therapy for Prostate CancerSanchia S. GoonewardeneNoch keine Bewertungen
- Pediatrics 2007 Weinberger 855 64Dokument10 SeitenPediatrics 2007 Weinberger 855 64Gintar Isnu WardoyoNoch keine Bewertungen
- PhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueDokument14 SeitenPhilHealth Circular No. 0035, s.2013 Annex 10 List of Alternative Documents For Record of Operative or Surgical TechniqueChrysanthus HerreraNoch keine Bewertungen
- M 371Dokument14 SeitenM 371Anonymous h0DxuJTNoch keine Bewertungen
- NUR 200 Lung Cancer Case StudyDokument2 SeitenNUR 200 Lung Cancer Case StudyLarso EngelNoch keine Bewertungen
- Bal 3Dokument12 SeitenBal 3isnanrNoch keine Bewertungen
- Respi DX Procedures Handouts For Asynch ActivityDokument8 SeitenRespi DX Procedures Handouts For Asynch ActivityBamba FloresNoch keine Bewertungen
- Goldenhar Syndrome AnesthesiaDokument4 SeitenGoldenhar Syndrome AnesthesiaTysonNoch keine Bewertungen
- PAPER (ENG) - Bai C., Et Al., 2013 GRE-CHN) Application of Flexible Bronchoscopy in Inhalation Lung InjuryDokument5 SeitenPAPER (ENG) - Bai C., Et Al., 2013 GRE-CHN) Application of Flexible Bronchoscopy in Inhalation Lung InjuryAldo Hip NaranjoNoch keine Bewertungen
- Olympus - Clean BF 160Dokument1 SeiteOlympus - Clean BF 160Eduardo ArreguinNoch keine Bewertungen
- Bronchoscopy For A Foreign Body in A ChildDokument19 SeitenBronchoscopy For A Foreign Body in A ChildsileNoch keine Bewertungen
- EndosDokument50 SeitenEndosBMT100% (3)
- Karl StorzDokument84 SeitenKarl StorzWaleed HashimNoch keine Bewertungen
- Awake Tracheal Intubation 2022Dokument8 SeitenAwake Tracheal Intubation 2022Gloria Stefany Fernandez CabreraNoch keine Bewertungen
- Surgical Management of Tracheal Compression Caused by Mediastinal Goiter: Is Extracorporeal Circulation Requisite钥Dokument3 SeitenSurgical Management of Tracheal Compression Caused by Mediastinal Goiter: Is Extracorporeal Circulation Requisite钥Indra W SaputraNoch keine Bewertungen
- BRONCHOSDokument6 SeitenBRONCHOSrajnishpathak648Noch keine Bewertungen
- Classification of MD PDFDokument167 SeitenClassification of MD PDFyagnaashi9092Noch keine Bewertungen
- AC200613 Full Answer KeyDokument26 SeitenAC200613 Full Answer KeySuganya BalachandranNoch keine Bewertungen
- Academy of Life Underwriting - ALU 101 - Basic Life Insurance Underwriting - Textbook For 2022 Exam Cycle (2021)Dokument359 SeitenAcademy of Life Underwriting - ALU 101 - Basic Life Insurance Underwriting - Textbook For 2022 Exam Cycle (2021)KALPESH SHAHNoch keine Bewertungen
- AirwayDokument36 SeitenAirwayRoger CorottoNoch keine Bewertungen
- EndoscopeDokument12 SeitenEndoscopemamjoud mustaphaNoch keine Bewertungen
- FUNDA Part 1Dokument5 SeitenFUNDA Part 1Jo Hn Vengz100% (1)
- Answer Key: Introduction To Clinical CodingDokument101 SeitenAnswer Key: Introduction To Clinical Codingthamizh555100% (1)
- Eye, E.N.T. & Dental AnaesthesiaDokument22 SeitenEye, E.N.T. & Dental AnaesthesiawellawalalasithNoch keine Bewertungen
- Hemoptysis - Case Presentation and DiscussionDokument52 SeitenHemoptysis - Case Presentation and DiscussionPGHC100% (1)
- Muhammad Rashid, Humaira Saleem, Saeed Bin Ayaz, Ijaz-Un-Nabi, Rashida Hussain, Faisal ManzoorDokument7 SeitenMuhammad Rashid, Humaira Saleem, Saeed Bin Ayaz, Ijaz-Un-Nabi, Rashida Hussain, Faisal ManzoorEMIRZA NUR WICAKSONONoch keine Bewertungen
- (B-0270) Day Surgery Procedure UnitDokument22 Seiten(B-0270) Day Surgery Procedure UnitAhmad Gamal Elden MAhanyNoch keine Bewertungen
- HemoptysisDokument21 SeitenHemoptysisdicky wahyudi100% (2)
- Thoracic SurgeryDokument178 SeitenThoracic SurgeryArthur Pendragon100% (1)
- Comparison OF Bronchoalveolar Lavage Cytology and Biopsy in Lung MalignancyDokument5 SeitenComparison OF Bronchoalveolar Lavage Cytology and Biopsy in Lung MalignancyDyahSavitriKusumoningtyasNoch keine Bewertungen
- Anesthesia For Patients With Mediastinal MassesDokument10 SeitenAnesthesia For Patients With Mediastinal MassesFityan Aulia RahmanNoch keine Bewertungen