Das könnte Ihnen auch gefallen
- The Three Elijah'sDokument35 SeitenThe Three Elijah'sGideon K. MutaiNoch keine Bewertungen
- Treatment of Resistant and Refractory HypertensionDokument21 SeitenTreatment of Resistant and Refractory HypertensionLuis Rodriguez100% (1)
- U.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3Dokument5 SeitenU.S. Preventive Services Task Force (USPSTF) Recommendations - Stats - Medbullets Step 2 - 3mtataNoch keine Bewertungen
- Third-Year OSCE Manual 2019-2020Dokument17 SeitenThird-Year OSCE Manual 2019-2020Agleema AhmedNoch keine Bewertungen
- A Guide To Vegetable GrowingDokument99 SeitenA Guide To Vegetable GrowingGideon K. MutaiNoch keine Bewertungen
- Acute Medicine: Shock: Inadequate Tissue and Organ PerfusionDokument3 SeitenAcute Medicine: Shock: Inadequate Tissue and Organ Perfusionmyat252Noch keine Bewertungen
- 22 Disritmia 2018Dokument60 Seiten22 Disritmia 2018Nur akilaNoch keine Bewertungen
- Part IIDokument64 SeitenPart IIhussainNoch keine Bewertungen
- Case Analysis Tool Worksheet: Squamous Cell CarcinomaDokument4 SeitenCase Analysis Tool Worksheet: Squamous Cell CarcinomaDina KristevaNoch keine Bewertungen
- Orientation To General SurgeryDokument0 SeitenOrientation To General SurgeryIrham TahkikNoch keine Bewertungen
- ECG Interpretation DR - Rawan AlshreemDokument25 SeitenECG Interpretation DR - Rawan AlshreemMarymii Al-sahlawiiNoch keine Bewertungen
- Weekly Clinical Prep Packet 12 REVISEDDokument12 SeitenWeekly Clinical Prep Packet 12 REVISEDMei SarteNoch keine Bewertungen
- St. La Salle Medical Case StudyDokument7 SeitenSt. La Salle Medical Case StudySavage SkylenNoch keine Bewertungen
- Practical Farm BuildingsDokument36 SeitenPractical Farm Buildingssnidely_whiplashNoch keine Bewertungen
- Clinical Skills Handbook 2015 MEDN40060 2Dokument66 SeitenClinical Skills Handbook 2015 MEDN40060 2Wilson KhawNoch keine Bewertungen
- Kathynotes PDFDokument103 SeitenKathynotes PDFvarrakeshNoch keine Bewertungen
- YFT IM Notes 1Dokument100 SeitenYFT IM Notes 1AHMAD ALROWAILYNoch keine Bewertungen
- Source NotesDokument30 SeitenSource NotesChris Jardine Li100% (1)
- GI Signs and SymptomsDokument40 SeitenGI Signs and SymptomsJohnny BeeNoch keine Bewertungen
- How To Make An Oral Case Presentation To Healthcare ColleaguesDokument5 SeitenHow To Make An Oral Case Presentation To Healthcare ColleaguesYuliana Citra AnggraeniNoch keine Bewertungen
- Objectives IMDokument104 SeitenObjectives IMlaraNoch keine Bewertungen
- Gleason System of Grading Prostate CancerDokument2 SeitenGleason System of Grading Prostate CancerGideon K. MutaiNoch keine Bewertungen
- Smhs - Gwu.edu Sample NotesDokument3 SeitenSmhs - Gwu.edu Sample NotesWaqas HaleemNoch keine Bewertungen
- Care Plan Handbook TemplateDokument34 SeitenCare Plan Handbook TemplateBreanna Hopkins100% (1)
- Pediatrics Vaccine and Milestone ReviewDokument31 SeitenPediatrics Vaccine and Milestone ReviewDrSajid BuzdarNoch keine Bewertungen
- Principles of Safe SurgeryDokument19 SeitenPrinciples of Safe SurgeryGideon K. MutaiNoch keine Bewertungen
- ICU Presentation - Systems BasedDokument1 SeiteICU Presentation - Systems BasedBryan NomenNoch keine Bewertungen
- The AOA Guide: How To Succeed Inthe3 Year Clerkships: Example Notes For The MsiiiDokument20 SeitenThe AOA Guide: How To Succeed Inthe3 Year Clerkships: Example Notes For The Msiiinybiker100% (1)
- Internal Medicine Lecture NotesDokument179 SeitenInternal Medicine Lecture NotesZeeshan Ahmed100% (3)
- Introduction History and ExaminationDokument43 SeitenIntroduction History and ExaminationDanyal Hassan100% (1)
- Seizures in Children CMEDokument43 SeitenSeizures in Children CMEGideon K. Mutai100% (1)
- Needs of New-Born CareDokument27 SeitenNeeds of New-Born CarePruthviNoch keine Bewertungen
- Clinical Examinations Crib Sheet v7Dokument36 SeitenClinical Examinations Crib Sheet v7aparish10100% (1)
- H&P OutlineDokument5 SeitenH&P Outlineginadaislu100% (1)
- Peds Shelf NotesDokument88 SeitenPeds Shelf Notesγιαννης παπαςNoch keine Bewertungen
- Cardiology ConsultsDokument2 SeitenCardiology ConsultsjuweriyNoch keine Bewertungen
- Gynecology and ObstetricsvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvDokument133 SeitenGynecology and ObstetricsvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvvȚurcan IurieNoch keine Bewertungen
- Measurement in ResearchDokument4 SeitenMeasurement in ResearchGideon K. Mutai100% (1)
- Admission NotesDokument16 SeitenAdmission NotesCaisar Dewi MaulinaNoch keine Bewertungen
- MCQ 1. Heart Sound Heart Sound S1 S2Dokument7 SeitenMCQ 1. Heart Sound Heart Sound S1 S2Atirah AaNoch keine Bewertungen
- NCM 109 CMC at Risk PrelimDokument19 SeitenNCM 109 CMC at Risk PrelimBeche May Lumantas100% (1)
- Introduction To Internal Medicine - PPTMDokument30 SeitenIntroduction To Internal Medicine - PPTMAddyNoch keine Bewertungen
- Pediatric Nursing Practice Test Part 1: Essential SkillsDokument19 SeitenPediatric Nursing Practice Test Part 1: Essential SkillsRjNoch keine Bewertungen
- Brain Sheet2011Dokument1 SeiteBrain Sheet2011nursekatieNoch keine Bewertungen
- HX TakingDokument37 SeitenHX TakingAya SalahNoch keine Bewertungen
- RCH Programme IntroductionDokument140 SeitenRCH Programme IntroductionPriya SharmaNoch keine Bewertungen
- Child DevelopmentDokument23 SeitenChild DevelopmentRahifah Mohd TejeriNoch keine Bewertungen
- ALCOHOL Pharmacology: Samuel Murano. Dept. of PharmacologyDokument23 SeitenALCOHOL Pharmacology: Samuel Murano. Dept. of PharmacologyGideon K. MutaiNoch keine Bewertungen
- Keys For A Happy MarriageDokument13 SeitenKeys For A Happy MarriageGideon K. Mutai100% (1)
- Keys For A Happy MarriageDokument13 SeitenKeys For A Happy MarriageGideon K. Mutai100% (1)
- Pedia Exam Set 1Dokument61 SeitenPedia Exam Set 1Yaj Cruzada100% (2)
- Deconstructing The ECG Curve - The Components of The Tracing: Key ConceptsDokument117 SeitenDeconstructing The ECG Curve - The Components of The Tracing: Key ConceptsdrynwhylNoch keine Bewertungen
- Unit-Plan: Submitted By: Ms - Prerna SharmaDokument4 SeitenUnit-Plan: Submitted By: Ms - Prerna SharmaPrernaSharma50% (2)
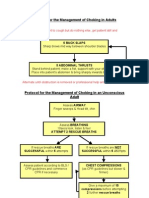
- Protocol For The Management of Choking in AdultsDokument3 SeitenProtocol For The Management of Choking in AdultsSarinah RynaNoch keine Bewertungen
- Lesson Plan On - Essential-NewbornDokument22 SeitenLesson Plan On - Essential-NewbornSwati Sharma100% (1)
- Seminar On Hospitalized ChildDokument17 SeitenSeminar On Hospitalized ChildAsma Saleem100% (1)
- Neonatal Jaundice CmeDokument39 SeitenNeonatal Jaundice CmeGideon K. Mutai100% (1)
- Montessori and ReligionDokument4 SeitenMontessori and ReligionIqra MontessoriNoch keine Bewertungen
- SOAP Presentation 5.19.16 PDFDokument1 SeiteSOAP Presentation 5.19.16 PDFnems92Noch keine Bewertungen
- Aquifer InternalMedicine09 - 55Dokument7 SeitenAquifer InternalMedicine09 - 55JulieNoch keine Bewertungen
- DeVirglio NotesDokument77 SeitenDeVirglio NotesAlvand SehatNoch keine Bewertungen
- Medicine Review 2018 1Dokument470 SeitenMedicine Review 2018 1Norjetalexis Maningo CabreraNoch keine Bewertungen
- Aquifer InternalMedicine11 - 45Dokument8 SeitenAquifer InternalMedicine11 - 45JulieNoch keine Bewertungen
- SketchyPath ChecklistDokument1 SeiteSketchyPath ChecklistFajar Raza100% (1)
- Step 1 Checklist for Biochemistry, Genetics and DevelopmentDokument11 SeitenStep 1 Checklist for Biochemistry, Genetics and DevelopmentHasan Khan RoudbaryNoch keine Bewertungen
- Theme 4 - HTN in The OSCEDokument1 SeiteTheme 4 - HTN in The OSCEShannon RamsumairNoch keine Bewertungen
- Interview Questions 2016 Draft Version 7-18-16Dokument6 SeitenInterview Questions 2016 Draft Version 7-18-16Sisca Dwi AgustinaNoch keine Bewertungen
- General Population (No Diabetes or CKD) Diabetes or CKD PresentDokument1 SeiteGeneral Population (No Diabetes or CKD) Diabetes or CKD PresentMuthia ArsilNoch keine Bewertungen
- Personal Statement - FinalDokument2 SeitenPersonal Statement - Finalapi-383932502Noch keine Bewertungen
- Shock PresentationDokument20 SeitenShock Presentationrosalyn sugayNoch keine Bewertungen
- Examination of The Central Nervous SystemDokument3 SeitenExamination of The Central Nervous Systemkenners100% (13)
- Pharmacology Exam4 ReviewDokument8 SeitenPharmacology Exam4 ReviewNatalia BortellNoch keine Bewertungen
- Developmental MilestonesDokument1 SeiteDevelopmental MilestonesStephen BryanNoch keine Bewertungen
- Victorias New ResumeDokument2 SeitenVictorias New Resumeapi-513192361Noch keine Bewertungen
- Gastroenterology AscitesDokument2 SeitenGastroenterology AscitesNour SamadNoch keine Bewertungen
- Medicine - Lab Coat PocketsDokument1 SeiteMedicine - Lab Coat Pocketsskeebs23Noch keine Bewertungen
- Step1 6week DIT StudyPlan 3 PDFDokument2 SeitenStep1 6week DIT StudyPlan 3 PDFSubika HaiderNoch keine Bewertungen
- Test 33: Surgery - Rheumatology/Orthopedics & SportsDokument8 SeitenTest 33: Surgery - Rheumatology/Orthopedics & Sportskabal321Noch keine Bewertungen
- Family Medicine PresentationDokument53 SeitenFamily Medicine PresentationNancy BaggaNoch keine Bewertungen
- Medical Student CV TemplateDokument3 SeitenMedical Student CV Templatepro sanNoch keine Bewertungen
- CCT - CCI Code of EthicsDokument2 SeitenCCT - CCI Code of EthicsAvanca LouisNoch keine Bewertungen
- Paeds Handbook Class2021 1568487638Dokument30 SeitenPaeds Handbook Class2021 1568487638kafosidNoch keine Bewertungen
- Diabetes and Hiv: Dr. Kiprono Mutai, Olenguruone Sub-County HospDokument9 SeitenDiabetes and Hiv: Dr. Kiprono Mutai, Olenguruone Sub-County HospGideon K. MutaiNoch keine Bewertungen
- Asthma in Children CMEDokument37 SeitenAsthma in Children CMEGideon K. MutaiNoch keine Bewertungen
- Know Your IQDokument1 SeiteKnow Your IQGideon K. MutaiNoch keine Bewertungen
- Genital Tract TraumaDokument18 SeitenGenital Tract TraumaGideon K. MutaiNoch keine Bewertungen
- CMNH-Obstetric Emergencies - March 2016Dokument46 SeitenCMNH-Obstetric Emergencies - March 2016Gideon K. MutaiNoch keine Bewertungen
- R S K - S G: OAD Igns of Enya A Tudy UideDokument10 SeitenR S K - S G: OAD Igns of Enya A Tudy UideGideon K. MutaiNoch keine Bewertungen
- Occupational and EnvironmentalDokument117 SeitenOccupational and EnvironmentalGideon K. MutaiNoch keine Bewertungen
- Role of Partogram in Preventing Prolonged Labour PDFDokument4 SeitenRole of Partogram in Preventing Prolonged Labour PDFGideon K. MutaiNoch keine Bewertungen
- Bacillary Dysentery (Shigellosis) : Dept. of Infectious Disease Wang JingyanDokument20 SeitenBacillary Dysentery (Shigellosis) : Dept. of Infectious Disease Wang JingyanOrlando Carlos Ricaldi VictorioNoch keine Bewertungen
- Being A Better Being.Dokument5 SeitenBeing A Better Being.Gideon K. MutaiNoch keine Bewertungen
- Presented by Abhinay BhugooDokument32 SeitenPresented by Abhinay BhugooGideon K. MutaiNoch keine Bewertungen
- OSCE Pediatrics Observed Stations - Dr.D.Y.patil CME Aug 2012Dokument54 SeitenOSCE Pediatrics Observed Stations - Dr.D.Y.patil CME Aug 2012Gideon K. MutaiNoch keine Bewertungen
- EMBRYOLOGY CrammerDokument21 SeitenEMBRYOLOGY CrammeranotherlifestoryNoch keine Bewertungen
- RA Case Study: Joint Pain DiagnosisDokument17 SeitenRA Case Study: Joint Pain DiagnosisGideon K. MutaiNoch keine Bewertungen
- Epilepsy GuidelinesDokument75 SeitenEpilepsy GuidelinesGideon K. MutaiNoch keine Bewertungen
- DKA Guidelines for Managing Diabetic KetoacidosisDokument13 SeitenDKA Guidelines for Managing Diabetic KetoacidosisZaiem Akmal ZarkasiNoch keine Bewertungen
- Parent Handbook: Lilypad Learning CenterDokument27 SeitenParent Handbook: Lilypad Learning CenterPrabha GuptaNoch keine Bewertungen
- Ncma219 Lec MidtermDokument51 SeitenNcma219 Lec MidtermMacababbad Joshua MiguelNoch keine Bewertungen
- Anne Carpentier - Stages of Child Development - From Conception Onward PDFDokument33 SeitenAnne Carpentier - Stages of Child Development - From Conception Onward PDFGogutaNoch keine Bewertungen
- NEWBORN CARE QuizDokument2 SeitenNEWBORN CARE QuizLUISA CARANTESNoch keine Bewertungen
- Vitamin K 11 21 16Dokument13 SeitenVitamin K 11 21 16api-345397204Noch keine Bewertungen
- 295SDokument133 Seiten295SSania M. ChoudhryNoch keine Bewertungen
- Chapter 4 Physical Development in InfancyDokument41 SeitenChapter 4 Physical Development in InfancyLikith Kumar LikithNoch keine Bewertungen
- Advice Ideals and Rural Prairie Motherhood 1920-1929Dokument27 SeitenAdvice Ideals and Rural Prairie Motherhood 1920-1929William WanjohiNoch keine Bewertungen
- Pattern of Diseases and Care Outcomes of Neonates Admitted in Special Care Baby Unit of University College Hospital, Ibadan, Nigeria From 2007 To 2011.Dokument10 SeitenPattern of Diseases and Care Outcomes of Neonates Admitted in Special Care Baby Unit of University College Hospital, Ibadan, Nigeria From 2007 To 2011.IOSRjournalNoch keine Bewertungen
- Baby Registry ChecklistDokument2 SeitenBaby Registry ChecklistHanna Rafaela Ferreira Dalla PriaNoch keine Bewertungen
- Psychology of Infants as Learners - Developmental Milestones & ConceptsDokument4 SeitenPsychology of Infants as Learners - Developmental Milestones & ConceptsChristian Joni Salamante GregorioNoch keine Bewertungen
- NCM 33 Framework For Maternal and Child Health Nursing: ST ST RD ND TH TH RD TH TH THDokument5 SeitenNCM 33 Framework For Maternal and Child Health Nursing: ST ST RD ND TH TH RD TH TH THSherika Mariz Moreno GuarinNoch keine Bewertungen
- NeoReviews November 2022Dokument82 SeitenNeoReviews November 2022Raymundo AvilaNoch keine Bewertungen
- FINASLIDEMASTERALDokument42 SeitenFINASLIDEMASTERALClaudette Carylle IgnacioNoch keine Bewertungen
- Medical Devices and Ehealth SolutionsDokument76 SeitenMedical Devices and Ehealth SolutionsEliana Caceres TorricoNoch keine Bewertungen
- Meconium Stained LiquorDokument4 SeitenMeconium Stained LiquorYwagar YwagarNoch keine Bewertungen
- Iycf AsiaDokument68 SeitenIycf AsiaYahye CMNoch keine Bewertungen
- Punzalan, Joshua Mitchell L. Case-Scenarios-NICUDokument2 SeitenPunzalan, Joshua Mitchell L. Case-Scenarios-NICUJM PunzalanNoch keine Bewertungen
- Emotional Development in ChildrenDokument5 SeitenEmotional Development in ChildrenCharlemyne Quevedo LachanceNoch keine Bewertungen