Das könnte Ihnen auch gefallen
- Applied Time Series Econometrics: A Practical Guide for Macroeconomic Researchers with a Focus on AfricaVon EverandApplied Time Series Econometrics: A Practical Guide for Macroeconomic Researchers with a Focus on AfricaBewertung: 3 von 5 Sternen3/5 (1)
- Ehab M Aly-TS-JanDokument1 SeiteEhab M Aly-TS-JanEhab IbrahimNoch keine Bewertungen
- QF-105 Time CardDokument1 SeiteQF-105 Time CardSYED ARSHADULLAHNoch keine Bewertungen
- HEPC Time Sheet - ERVIN 1Dokument1 SeiteHEPC Time Sheet - ERVIN 1John Ervin AgenaNoch keine Bewertungen
- Replicon Excel Web Time SheetDokument4 SeitenReplicon Excel Web Time SheetSpreadsheetZONENoch keine Bewertungen
- Timesheet Sidrap Wajo Desember 2023Dokument2 SeitenTimesheet Sidrap Wajo Desember 2023rumahayahmkmi.ibt23Noch keine Bewertungen
- W28 Timesheet BARIA, Jayke J.Dokument10 SeitenW28 Timesheet BARIA, Jayke J.Akira SkyNoch keine Bewertungen
- Timesheet Mês de Setembro - 2022Dokument1 SeiteTimesheet Mês de Setembro - 2022Idiamine Da Alzira SKNoch keine Bewertungen
- Seleccion TimesheetDokument1 SeiteSeleccion TimesheetArjun KNoch keine Bewertungen
- Pay Date Amount Paid Cac No. Punch Date: UrbanDokument1 SeitePay Date Amount Paid Cac No. Punch Date: UrbanShivam SharmaNoch keine Bewertungen
- Casagrande b125Dokument8 SeitenCasagrande b125hamada11Noch keine Bewertungen
- Our Community Car Share Mileage LogDokument1 SeiteOur Community Car Share Mileage LogPatrick BecknellNoch keine Bewertungen
- (Bathroom) : Plano de Casa Económica 6X6Metros Vg-12Dokument1 Seite(Bathroom) : Plano de Casa Económica 6X6Metros Vg-12rodrigo puentesNoch keine Bewertungen
- Personnel Time Sheet Month:: Work Activity Total HrsDokument3 SeitenPersonnel Time Sheet Month:: Work Activity Total HrsnanivenkatgauravNoch keine Bewertungen
- 2024-01-15 - GK - 03 Kontrakan Jati KramatDokument1 Seite2024-01-15 - GK - 03 Kontrakan Jati Kramatnuke.rachmasariNoch keine Bewertungen
- R 407cDokument1 SeiteR 407cAhmadd Soultounii Arex TptuNoch keine Bewertungen
- TER TemplateDokument2 SeitenTER TemplateRheneir MoraNoch keine Bewertungen
- Bond Price With Excel FunctionsDokument6 SeitenBond Price With Excel Functionsapi-3763138Noch keine Bewertungen
- Calculation of Hvap From Experimented DataDokument2 SeitenCalculation of Hvap From Experimented DataDozdiNoch keine Bewertungen
- Gen Claim Form FormatDokument3 SeitenGen Claim Form FormatSITI NAJIBAH BINTI MOHD NORNoch keine Bewertungen
- Completely Clean Timesheet: January 2015: Contractor'S Name: Site Site Name Total HoursDokument1 SeiteCompletely Clean Timesheet: January 2015: Contractor'S Name: Site Site Name Total Hourssukhwinder17021984Noch keine Bewertungen
- FPS Rig Loadings Spreadsheet Disclaimer ExplainedDokument9 SeitenFPS Rig Loadings Spreadsheet Disclaimer Explainedpakbilal1Noch keine Bewertungen
- (Company Name) - Weekly Timesheet Template: 1234 Sesame ST., San Francisco, CA 94129 (123) 456-7890Dokument1 Seite(Company Name) - Weekly Timesheet Template: 1234 Sesame ST., San Francisco, CA 94129 (123) 456-7890sameeh kadourahNoch keine Bewertungen
- System Duct Pressure Loss CalculationDokument6 SeitenSystem Duct Pressure Loss Calculationthanh_79Noch keine Bewertungen
- ESTADO2Dokument4 SeitenESTADO2joca.civil23Noch keine Bewertungen
- Casa H3 Luciano KrukDokument4 SeitenCasa H3 Luciano KrukTMCoori TorresNoch keine Bewertungen
- TC SummaryDokument1 SeiteTC SummaryAkun GocarNoch keine Bewertungen
- Receipt Digital PaymentDokument1 SeiteReceipt Digital Paymentbagas atmojoNoch keine Bewertungen
- 2007 11 30 KaDokument4 Seiten2007 11 30 Kakiranabid100% (2)
- SummariesDokument3 SeitenSummariesKeithEscanlarTamanalNoch keine Bewertungen
- Urban: Pay Date Cac No. Amount Paid Punch DateDokument1 SeiteUrban: Pay Date Cac No. Amount Paid Punch DateK CHOUDHARYNoch keine Bewertungen
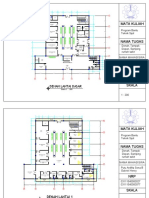
- Mata Kuliah: Denah Lantai DasarDokument6 SeitenMata Kuliah: Denah Lantai DasarsenaNoch keine Bewertungen
- Fun Run Pledges: School Number of Participants PLEDGES (Amount) LGU Private EntitiesDokument4 SeitenFun Run Pledges: School Number of Participants PLEDGES (Amount) LGU Private EntitiesKrishna SoliminianoNoch keine Bewertungen
- Dnorm EnvironmentDokument1 SeiteDnorm EnvironmentMárcioJoséMantauNoch keine Bewertungen
- Floor plan layout with room dimensionsDokument1 SeiteFloor plan layout with room dimensionsDaniela Velez AlvesNoch keine Bewertungen
- MbayeDokument1 SeiteMbayedionguesaliou873Noch keine Bewertungen
- Plano de Planta1Dokument1 SeitePlano de Planta1Christian Jimenez de la CruzNoch keine Bewertungen
- KFCA Electrical Load DeatilDokument4 SeitenKFCA Electrical Load Deatilarainzada807Noch keine Bewertungen
- Trabajo - 1Dokument1 SeiteTrabajo - 1ANGELA LUCIA GAMBOA MEJIANoch keine Bewertungen
- Final SchematicDokument14 SeitenFinal SchematicEmad ZakiNoch keine Bewertungen
- Identiication of Algae Growth KineticsDokument48 SeitenIdentiication of Algae Growth KineticsazmeerprimoNoch keine Bewertungen
- Multifamiliar 6 x15 (2) - ModelDokument1 SeiteMultifamiliar 6 x15 (2) - ModelRamiro ZambranoNoch keine Bewertungen
- Timesheet TemplateDokument1 SeiteTimesheet TemplateAmit RajputNoch keine Bewertungen
- Floor plan measurements layout guideDokument1 SeiteFloor plan measurements layout guideenyel2727Noch keine Bewertungen
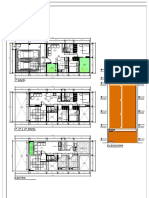
- Denah Lantai 1: Sauna R.MesinDokument1 SeiteDenah Lantai 1: Sauna R.MesinAndy HeaterNoch keine Bewertungen
- Monthly expenses and revenue for a fitness centerDokument1 SeiteMonthly expenses and revenue for a fitness centerAndy HeaterNoch keine Bewertungen
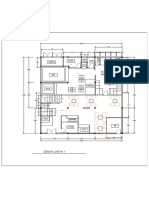
- Denah Rumah 131 m2Dokument1 SeiteDenah Rumah 131 m2ancha3d.enNoch keine Bewertungen
- Free Online Interactive Psychrometric Chart PDFDokument1 SeiteFree Online Interactive Psychrometric Chart PDFMayra SandovalNoch keine Bewertungen
- Credit Note FormatDokument1 SeiteCredit Note FormatMukesh ShahNoch keine Bewertungen
- Debit Note Format PDFDokument1 SeiteDebit Note Format PDFMukesh ShahNoch keine Bewertungen
- Pay Date Amount Paid Cac No. Punch Date: UrbanDokument1 SeitePay Date Amount Paid Cac No. Punch Date: UrbanMONISH NAYARNoch keine Bewertungen
- Credit Note: Credit Note No Date Name of The ClientDokument1 SeiteCredit Note: Credit Note No Date Name of The ClientMukesh ShahNoch keine Bewertungen
- Kepadatan Nyamuk Anopheles Di Sowi Gunung (UOL)Dokument6 SeitenKepadatan Nyamuk Anopheles Di Sowi Gunung (UOL)den BagusNoch keine Bewertungen
- 04 Ejemplo Corte 2Dokument1 Seite04 Ejemplo Corte 2CrupssNoch keine Bewertungen
- WDL HV D.lobby 220830-DL - LNG Sit.03Dokument1 SeiteWDL HV D.lobby 220830-DL - LNG Sit.03Antonio DumitrescuNoch keine Bewertungen
- Department of AgricultureDokument1 SeiteDepartment of AgricultureVon DeVoirNoch keine Bewertungen
- Invoice Template SideDokument1 SeiteInvoice Template SideAkbar ShariefNoch keine Bewertungen
- Monthly TimesheetDokument2 SeitenMonthly TimesheetashrafhitlerNoch keine Bewertungen
- O&M Vidisha bill details for July 2020Dokument1 SeiteO&M Vidisha bill details for July 2020Anshul ShrivastavaNoch keine Bewertungen
- Index Terms LinksDokument18 SeitenIndex Terms LinksBhaskar NandiNoch keine Bewertungen
- BGR ApplicationFormDokument4 SeitenBGR ApplicationFormsudheerNoch keine Bewertungen
- Health Record Sheet Bhaskar NandiDokument2 SeitenHealth Record Sheet Bhaskar NandiBhaskar NandiNoch keine Bewertungen
- Apdx01Dokument9 SeitenApdx01Bhaskar NandiNoch keine Bewertungen
- Ansys CFDDokument80 SeitenAnsys CFDNikola Boskovic100% (1)
- Silo CapDokument5 SeitenSilo CapOliver SanvictoresNoch keine Bewertungen
- DARCY FRICTION LOSS CALCULATORDokument2 SeitenDARCY FRICTION LOSS CALCULATORBhaskar NandiNoch keine Bewertungen
- Brill Beggs ZDokument3 SeitenBrill Beggs ZtechbhaskarNoch keine Bewertungen
- Amine Sweetening Unit Simplified Design EquationsDokument20 SeitenAmine Sweetening Unit Simplified Design EquationsPragathees Waran100% (1)
- Vertical Silo Costs and Dimensions for Dairy Cattle FeedingTITLE Horizontal Silo and Ag Bag Cost Analysis for Dairy OperationsDokument10 SeitenVertical Silo Costs and Dimensions for Dairy Cattle FeedingTITLE Horizontal Silo and Ag Bag Cost Analysis for Dairy OperationsOliver SanvictoresNoch keine Bewertungen
- ANSYS 14.5 For Win Installation GuideDokument71 SeitenANSYS 14.5 For Win Installation GuideRul's SuchuzNoch keine Bewertungen
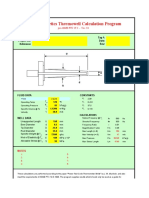
- Thermo-Kinetics Thermowell Calculation Program: Company: Tag #: Project No: Date: RevDokument14 SeitenThermo-Kinetics Thermowell Calculation Program: Company: Tag #: Project No: Date: Revvazzoleralex6884Noch keine Bewertungen
- NSIC - Print Application PDFDokument3 SeitenNSIC - Print Application PDFBhaskar NandiNoch keine Bewertungen
- Silo Design Codes-Limits &inconsistancies-2015 PaperDokument10 SeitenSilo Design Codes-Limits &inconsistancies-2015 PaperAnonymous wWOWz9UnW100% (1)
- Silo CapDokument5 SeitenSilo CapOliver SanvictoresNoch keine Bewertungen
- 343 1410 1 PBDokument5 Seiten343 1410 1 PBBhaskar NandiNoch keine Bewertungen
- Appendix A: Mesh Independence StudyDokument7 SeitenAppendix A: Mesh Independence StudyBhaskar NandiNoch keine Bewertungen
- Daily ReportDokument7 SeitenDaily ReportSol IturriagaNoch keine Bewertungen
- Preprints201608 0008 v1Dokument11 SeitenPreprints201608 0008 v1Bhaskar NandiNoch keine Bewertungen
- Wall Y+strategy For Dealing With Wall Bounded Turbulents Flows PDFDokument6 SeitenWall Y+strategy For Dealing With Wall Bounded Turbulents Flows PDFmatteo_1234Noch keine Bewertungen
- Thermal energy storage materials performance comparisonDokument7 SeitenThermal energy storage materials performance comparisonBhaskar NandiNoch keine Bewertungen
- Thermo-Kinetics Thermowell Calculation Program: Company: Tag #: Project No: Date: RevDokument14 SeitenThermo-Kinetics Thermowell Calculation Program: Company: Tag #: Project No: Date: Revvazzoleralex6884Noch keine Bewertungen
- Computational Fluid Dynamics (CFD) Study Investigating The EffectDokument105 SeitenComputational Fluid Dynamics (CFD) Study Investigating The EffectBhaskar NandiNoch keine Bewertungen
- Simulation of Turbulent Flow Through Porous Media Employing A v2f ModelDokument9 SeitenSimulation of Turbulent Flow Through Porous Media Employing A v2f ModelBhaskar NandiNoch keine Bewertungen
- Computational Fluid Dynamics (CFD) Study Investigating The EffectDokument105 SeitenComputational Fluid Dynamics (CFD) Study Investigating The EffectBhaskar NandiNoch keine Bewertungen
- Macroscopic Modeling of Turbulence in Porous Media Flows: Federico E. Teruel, Rizwan-UddinDokument16 SeitenMacroscopic Modeling of Turbulence in Porous Media Flows: Federico E. Teruel, Rizwan-UddinBhaskar NandiNoch keine Bewertungen
- 3b993cef 4ec6 4844 97ec Cc8cb8e68000 141514Dokument9 Seiten3b993cef 4ec6 4844 97ec Cc8cb8e68000 141514Bhaskar NandiNoch keine Bewertungen
- Mathematical Model of Packed Bed Solar Thermal Energy Storage SimulationDokument8 SeitenMathematical Model of Packed Bed Solar Thermal Energy Storage SimulationBhaskar NandiNoch keine Bewertungen
- Thermo-Kinetics Thermowell Calculation Program: Company: Tag #: Project No: Date: RevDokument14 SeitenThermo-Kinetics Thermowell Calculation Program: Company: Tag #: Project No: Date: Revvazzoleralex6884Noch keine Bewertungen
- Taxi Invoice - Multiple Trips: Service Recipient InformationDokument2 SeitenTaxi Invoice - Multiple Trips: Service Recipient InformationBhaskar NandiNoch keine Bewertungen
- Resolution For AppointmentDokument3 SeitenResolution For Appointmentjerome geoligaoNoch keine Bewertungen
- 20101015121029lecture-7 - (Sem1!10!11) Feminism in MalaysiaDokument42 Seiten20101015121029lecture-7 - (Sem1!10!11) Feminism in Malaysiapeningla100% (1)
- Preliminary Injunction Rules ExplainedDokument12 SeitenPreliminary Injunction Rules ExplainedAna leah Orbeta-mamburamNoch keine Bewertungen
- Public Hearing on Bluehouse ProjectDokument2 SeitenPublic Hearing on Bluehouse ProjectChristjohn VillaluzNoch keine Bewertungen
- HUREM 11quiz1Dokument2 SeitenHUREM 11quiz1Juanito Libron JrNoch keine Bewertungen
- Values and Ethics - Subroto BagchiDokument5 SeitenValues and Ethics - Subroto BagchiManoj KumarNoch keine Bewertungen
- BPI V Far East MolassesDokument4 SeitenBPI V Far East MolassesYodh Jamin OngNoch keine Bewertungen
- Supreme Court upholds dismissal of worker for serious misconductDokument2 SeitenSupreme Court upholds dismissal of worker for serious misconductJoseNoch keine Bewertungen
- Black CatDokument2 SeitenBlack CatEduardo GarciaNoch keine Bewertungen
- ANFFl LYERS2012Dokument2 SeitenANFFl LYERS2012Clifford ImsonNoch keine Bewertungen
- Bullying en La SecundariaDokument272 SeitenBullying en La SecundariaGiancarlo Castelo100% (1)
- IHL 1 BALLB ProjectDokument16 SeitenIHL 1 BALLB Projectabcde fghikjNoch keine Bewertungen
- Mississippi Freedom Caucus LetterDokument2 SeitenMississippi Freedom Caucus LetterBreitbart NewsNoch keine Bewertungen
- Delphia Yacht Model d40 PDFDokument10 SeitenDelphia Yacht Model d40 PDFBf IpanemaNoch keine Bewertungen
- Perspectives Test 1Dokument5 SeitenPerspectives Test 1ΒΡΕΦΟΝΗΠΙΑΚΟΣ ΝΕΑΣ ΚΥΔΩΝΙΑΣ50% (2)
- Crimpro Codal BreakdownDokument13 SeitenCrimpro Codal BreakdownsobranggandakoNoch keine Bewertungen
- DAP AN VA HDC tiếng AnhDokument3 SeitenDAP AN VA HDC tiếng AnhDương Thanh VânNoch keine Bewertungen
- Jissen Issue 6Dokument92 SeitenJissen Issue 6Antoine Hoang100% (1)
- Sps. Firme vs. Bukal Enterprises and Development CorporationDokument12 SeitenSps. Firme vs. Bukal Enterprises and Development CorporationdanieNoch keine Bewertungen
- Bulk Sales Law Not Violated by Foundry Shop SaleDokument2 SeitenBulk Sales Law Not Violated by Foundry Shop SaleTukne SanzNoch keine Bewertungen
- DSNLU Provisional Admission List 2020Dokument3 SeitenDSNLU Provisional Admission List 2020SAI CHAITANYA YEPURINoch keine Bewertungen
- Re. Balia and San Francisco RlyDokument2 SeitenRe. Balia and San Francisco RlyJnine McNamaraNoch keine Bewertungen
- RICS APC - M006 - Conflict AvoidanceDokument24 SeitenRICS APC - M006 - Conflict Avoidancebrene88100% (13)
- BG, SBLC, Rwa LeaseDokument23 SeitenBG, SBLC, Rwa LeaseJosephNoch keine Bewertungen
- Republic Vs LacapDokument17 SeitenRepublic Vs LacapAyaanniieeNoch keine Bewertungen
- Case Digest For Marcos V CADokument1 SeiteCase Digest For Marcos V CAMicah GimeloNoch keine Bewertungen
- Lectures 8 & 9: Protection of CreditorsDokument36 SeitenLectures 8 & 9: Protection of CreditorsYeung Ching TinNoch keine Bewertungen
- 50 Reasons Why Jesus Came To Die SherwinDokument28 Seiten50 Reasons Why Jesus Came To Die SherwinNori Nori KunNoch keine Bewertungen
- Ebook - PDF - Tim Harding - Two Knights Defence Part II - ChessDokument13 SeitenEbook - PDF - Tim Harding - Two Knights Defence Part II - ChessPR0T0Noch keine Bewertungen
- Research Essay FinalDokument10 SeitenResearch Essay Finalapi-534813185Noch keine Bewertungen