Das könnte Ihnen auch gefallen
- Thừa cân, béo phì liên quan đến nhiều loại bệnh tật nguy hiểm-wed HarvardDokument24 SeitenThừa cân, béo phì liên quan đến nhiều loại bệnh tật nguy hiểm-wed HarvardNam NguyenHoangNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 15: MusculoskeletalVon EverandComplementary and Alternative Medical Lab Testing Part 15: MusculoskeletalNoch keine Bewertungen
- Kecenderungan Masalah Muskoloskeletal Pada ObesitasDokument15 SeitenKecenderungan Masalah Muskoloskeletal Pada ObesitasperpesananNoch keine Bewertungen
- Hamann Kirschner Guenther Hofbauer 2012Dokument9 SeitenHamann Kirschner Guenther Hofbauer 2012muhammad fajrinNoch keine Bewertungen
- R245 FullDokument11 SeitenR245 FullYuliana WiralestariNoch keine Bewertungen
- The Role of Diabetes, Obesity, and Metabolic Syndrome in StrokeDokument7 SeitenThe Role of Diabetes, Obesity, and Metabolic Syndrome in StrokeEmir SaricNoch keine Bewertungen
- Current Osteoporosis Reports Volume 11 Issue 1 2013 (Doi 10.1007 - S11914-012-0127-Y) Juliet Compston - Obesity and BoneDokument6 SeitenCurrent Osteoporosis Reports Volume 11 Issue 1 2013 (Doi 10.1007 - S11914-012-0127-Y) Juliet Compston - Obesity and BoneBudhiNoch keine Bewertungen
- Age MenarcheDokument7 SeitenAge MenarchenamiracarolineNoch keine Bewertungen
- Obesity and Women's Health: An Evidence-Based ReviewDokument11 SeitenObesity and Women's Health: An Evidence-Based ReviewJuly ToscanoNoch keine Bewertungen
- Journal of Clinical Gerontology & Geriatrics: Original ArticleDokument6 SeitenJournal of Clinical Gerontology & Geriatrics: Original ArticleDeedee RenovaldiNoch keine Bewertungen
- Complications of Obesity in AdultsDokument5 SeitenComplications of Obesity in AdultsKlinik FiraraNoch keine Bewertungen
- Medical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660Dokument6 SeitenMedical Hazards of Obesity: Ann Intern Med. 1993 119 (7 PT 2) :655-660David WheelerNoch keine Bewertungen
- Joernal 3Dokument13 SeitenJoernal 3Dyra DizhwarNoch keine Bewertungen
- Journal About Stroke (Pat)Dokument4 SeitenJournal About Stroke (Pat)Patricia Kaye Tayag CastroNoch keine Bewertungen
- 1 s2.0 S875632822030048X MainDokument11 Seiten1 s2.0 S875632822030048X MainLourdes MoratoNoch keine Bewertungen
- GoutDokument17 SeitenGoutnadita erischaNoch keine Bewertungen
- Obesity and The Risk of Cryptogenic Ischemic Stroke in Young AdultsDokument25 SeitenObesity and The Risk of Cryptogenic Ischemic Stroke in Young AdultsKhalilullah ArsyiNoch keine Bewertungen
- Higher Body Mass Index Leads To Longer Operative Time in Total Knee ArthroplastyDokument7 SeitenHigher Body Mass Index Leads To Longer Operative Time in Total Knee ArthroplastydermoNoch keine Bewertungen
- Osteo RXDokument27 SeitenOsteo RXHarun NasutionNoch keine Bewertungen
- Eating Behaviors: Ricarda Ohlmer, Corinna Jacobi, Eike FittigDokument4 SeitenEating Behaviors: Ricarda Ohlmer, Corinna Jacobi, Eike FittigAna PasoleaNoch keine Bewertungen
- Bone Metabolism and Fracture Risk in Type 2 Diabetes MellitusDokument12 SeitenBone Metabolism and Fracture Risk in Type 2 Diabetes MellituslusianapsNoch keine Bewertungen
- Metabolic Disorders Related ToDokument13 SeitenMetabolic Disorders Related TovsdeepsNoch keine Bewertungen
- Theburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingDokument12 SeitenTheburdenofosteoarthritis Inolderadults: Gillian A. Hawker,, Lauren K. KingabdulfatahalhemeryNoch keine Bewertungen
- EU Rccm.200611-1717ocDokument6 SeitenEU Rccm.200611-1717ocDumitru BiniucNoch keine Bewertungen
- Is There A Relationship Between Periodontal Disease and Causes of Death? A Cross Sectional StudyDokument6 SeitenIs There A Relationship Between Periodontal Disease and Causes of Death? A Cross Sectional StudyYaarit IustainNoch keine Bewertungen
- Hostility and The Metabolic Syndrome in Older Males: The Normative Aging StudyDokument10 SeitenHostility and The Metabolic Syndrome in Older Males: The Normative Aging StudymrclpppNoch keine Bewertungen
- Public Health and The EyeDokument16 SeitenPublic Health and The EyeAngkat Prasetya Abdi NegaraNoch keine Bewertungen
- Enf Tiroidea en El AncianoDokument14 SeitenEnf Tiroidea en El AncianoJuan ZamoraNoch keine Bewertungen
- Disparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsDokument5 SeitenDisparities in Periodontitis Prevalence Among Chronic Kidney Disease PatientsKristelle HernandezNoch keine Bewertungen
- The Metabolic Syndrome in Healthy, Multiethnic Adolescents in Toronto, Ontario: The Use of Fasting Blood Glucose As A Simple IndicatorDokument5 SeitenThe Metabolic Syndrome in Healthy, Multiethnic Adolescents in Toronto, Ontario: The Use of Fasting Blood Glucose As A Simple Indicatordoxy20Noch keine Bewertungen
- Profil Lipid Dan Resiko Kejadian Penyakit Jantung Koroner (PJK) Pada Wanita Menopouse Di Kota MalangDokument12 SeitenProfil Lipid Dan Resiko Kejadian Penyakit Jantung Koroner (PJK) Pada Wanita Menopouse Di Kota MalangDadang KriztantoNoch keine Bewertungen
- Osteoporosis in Older AdultsDokument12 SeitenOsteoporosis in Older AdultsJuan Diego Sandoval RojasNoch keine Bewertungen
- Final PortfolioDokument10 SeitenFinal Portfolioapi-272608990Noch keine Bewertungen
- AbstractDokument1 SeiteAbstractmich__aishkaiNoch keine Bewertungen
- Selección de Resúmenes de Menopausia Semana Del 6 Al 12 de Agosto de 2014Dokument5 SeitenSelección de Resúmenes de Menopausia Semana Del 6 Al 12 de Agosto de 2014rocksurNoch keine Bewertungen
- 168 Essentials of Gerontological Nursing: CancerDokument3 Seiten168 Essentials of Gerontological Nursing: CancerNeoGellinNoch keine Bewertungen
- Selección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014Dokument5 SeitenSelección de Resúmenes de Menopausia Semana Del 10 Al 21 de Septiembre de 2014rocksurNoch keine Bewertungen
- Obesity PBLDokument2 SeitenObesity PBLLeanneNoch keine Bewertungen
- The Association Between Body Mass Index and Osteoporosis in Patients Referred For A Bone Mineral Density ExaminationDokument7 SeitenThe Association Between Body Mass Index and Osteoporosis in Patients Referred For A Bone Mineral Density ExaminationPradnya ParamitaNoch keine Bewertungen
- Musculo-Skeletal Disorders - GoutDokument14 SeitenMusculo-Skeletal Disorders - GoutKyle J. NortonNoch keine Bewertungen
- Nutrition and Vascular DementiaDokument6 SeitenNutrition and Vascular Dementiaapi-150223943Noch keine Bewertungen
- Association of Xanthelasma Palpebrarum (XP) With Cardiovascular Disease (CVD) Risk FactorsDokument6 SeitenAssociation of Xanthelasma Palpebrarum (XP) With Cardiovascular Disease (CVD) Risk Factorssri karuniaNoch keine Bewertungen
- CaídasDokument5 SeitenCaídasRocio ConsueloNoch keine Bewertungen
- Epid 1Dokument4 SeitenEpid 1Annafiatu zakiahNoch keine Bewertungen
- Prevalence of Hypertension Among Obese and Non-Obese Patients With Coronary Artery DiseaseDokument4 SeitenPrevalence of Hypertension Among Obese and Non-Obese Patients With Coronary Artery DiseasePrinceTumbuktooNoch keine Bewertungen
- Abstract: Elderly, Hypertension, Body Mass Index, Waist Circumference and HipDokument10 SeitenAbstract: Elderly, Hypertension, Body Mass Index, Waist Circumference and Hiprachelia87Noch keine Bewertungen
- Womenshealth & NutritionDokument5 SeitenWomenshealth & Nutritionbragaru.vladNoch keine Bewertungen
- Effect of Obesity 2Dokument14 SeitenEffect of Obesity 2eyaa0aliaNoch keine Bewertungen
- Fat and Lean Masses in Youths With Down Syndrome: Gender DifferencesDokument9 SeitenFat and Lean Masses in Youths With Down Syndrome: Gender DifferencesyenrilisnaNoch keine Bewertungen
- The Association Between Insomnia and Cardiovascular DiseasesDokument8 SeitenThe Association Between Insomnia and Cardiovascular Diseasesnouval_iqbalNoch keine Bewertungen
- Screening For Osteoporosis: Clinical PracticeDokument8 SeitenScreening For Osteoporosis: Clinical PracticeGayuh PrastyaNoch keine Bewertungen
- Indikator Risiko Diabetes Dan Hipertensi Pada Orang Dewasa Di IndonesiaDokument17 SeitenIndikator Risiko Diabetes Dan Hipertensi Pada Orang Dewasa Di IndonesiaNovry DodyNoch keine Bewertungen
- Selección de Resúmenes de Menopausia Semana Del 30 de Julio Al 5 de Agosto de 2014Dokument3 SeitenSelección de Resúmenes de Menopausia Semana Del 30 de Julio Al 5 de Agosto de 2014rocksurNoch keine Bewertungen
- Final Research PaperDokument16 SeitenFinal Research Paperapi-593862121Noch keine Bewertungen
- Smoking CaannabisDokument9 SeitenSmoking CaannabisEliza DNNoch keine Bewertungen
- Aipm 15 82Dokument6 SeitenAipm 15 82Isini sehansa amarathungaNoch keine Bewertungen
- Obesity & Osteoarthritis PDFDokument9 SeitenObesity & Osteoarthritis PDFTaufik Ramadhan BiyaNoch keine Bewertungen
- Metabolically Healthy Obese Women at Risk For Heart DiseaseDokument8 SeitenMetabolically Healthy Obese Women at Risk For Heart DiseaseGhinaAlmasNurafinaNoch keine Bewertungen
- 6187 DD 01Dokument4 Seiten6187 DD 01Angkat Prasetya Abdi NegaraNoch keine Bewertungen
- Who Imt Girls 5-19Dokument1 SeiteWho Imt Girls 5-19Rifky F NaratamaNoch keine Bewertungen
- Who Imt Boys 5-19 TahunDokument1 SeiteWho Imt Boys 5-19 TahunRifky F Naratama100% (1)
- Gizi Indonesia: Journal of The Indonesian Nutrition AssociationDokument12 SeitenGizi Indonesia: Journal of The Indonesian Nutrition AssociationRifky F NaratamaNoch keine Bewertungen
- 2 - 5 Tahun Laki-Laki PDFDokument1 Seite2 - 5 Tahun Laki-Laki PDFRifky F NaratamaNoch keine Bewertungen
- Homoeopathic Drug Pictures PDFDokument718 SeitenHomoeopathic Drug Pictures PDFNimesh PatelNoch keine Bewertungen
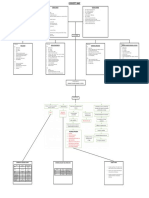
- IM-CAP Concept MapDokument1 SeiteIM-CAP Concept MapTrisNoch keine Bewertungen
- Integrated Comprehensive Test IiiDokument14 SeitenIntegrated Comprehensive Test IiiGhee Lardizabal0% (1)
- Common Prescribed DrugsDokument33 SeitenCommon Prescribed DrugsGlessica You50% (4)
- Orbit (Kankis)Dokument42 SeitenOrbit (Kankis)Jel JelitaaaNoch keine Bewertungen
- DRNB Medical Gastroenterology Paper1Dokument4 SeitenDRNB Medical Gastroenterology Paper1Srinivas PingaliNoch keine Bewertungen
- Bio Project-Small PoxDokument5 SeitenBio Project-Small Poxapi-494770168Noch keine Bewertungen
- In MemoriamDokument6 SeitenIn MemoriamChristopher PhillipsNoch keine Bewertungen
- Activity IntoleranceDokument4 SeitenActivity IntoleranceShermane Criszen F. SallanNoch keine Bewertungen
- Flu Vaccine: Information For People at RiskDokument8 SeitenFlu Vaccine: Information For People at Riskkovi mNoch keine Bewertungen
- A Vegan PowerDokument3 SeitenA Vegan PowerashankarNoch keine Bewertungen
- Yoga and MeditationDokument28 SeitenYoga and MeditationVivek VashisthNoch keine Bewertungen
- Occupational Health Pre-Employment Health Assessment Form March 08Dokument4 SeitenOccupational Health Pre-Employment Health Assessment Form March 08queenmombi100% (2)
- Raynaud's DiseaseDokument8 SeitenRaynaud's DiseaseDana del PilarNoch keine Bewertungen
- University of Kerbala College of Medicine Department of Pediatrics Clerkship Log-Book (Years 4) 2020-2021Dokument57 SeitenUniversity of Kerbala College of Medicine Department of Pediatrics Clerkship Log-Book (Years 4) 2020-2021صفا أحمد هاشم جبار 4Noch keine Bewertungen
- Nursing Pharmacology COMPLETEDokument40 SeitenNursing Pharmacology COMPLETEMonique Leonardo100% (8)
- MeaslesDokument23 SeitenMeaslesSaad MotawéaNoch keine Bewertungen
- Ncp-Ineffective Breathing PatternDokument4 SeitenNcp-Ineffective Breathing PatternRoxanne Ganayo Claver100% (1)
- Alternative Fibromyalgia Pain Management SuggestionsDokument4 SeitenAlternative Fibromyalgia Pain Management SuggestionsCinda CrawfordNoch keine Bewertungen
- High Risk Pregnancy HB TranxDokument11 SeitenHigh Risk Pregnancy HB TranxangeliquepastranaNoch keine Bewertungen
- Healing Siddha Medicine-LibreDokument4 SeitenHealing Siddha Medicine-LibreVijay ShanmugasundaramNoch keine Bewertungen
- SJ 5Dokument3 SeitenSJ 5ray72roNoch keine Bewertungen
- DreamsDokument52 SeitenDreamsNill SalunkeNoch keine Bewertungen
- Cure For All DiseasesDokument4 SeitenCure For All DiseasesNiquezNoch keine Bewertungen
- DRUG STUDY Bronchitis CorsigaDokument8 SeitenDRUG STUDY Bronchitis CorsigaKasandra Dawn Moquia BerisoNoch keine Bewertungen
- Lactational Mastitis Puerperal 2020Dokument12 SeitenLactational Mastitis Puerperal 2020bgNoch keine Bewertungen
- Case PresentationDokument14 SeitenCase PresentationFatema RavatNoch keine Bewertungen
- Nursing Care of DiarrheaDokument30 SeitenNursing Care of DiarrheayustiNoch keine Bewertungen
- Mental Health Problems Among Elderly in India: A Social Work Study and Its InterventionDokument16 SeitenMental Health Problems Among Elderly in India: A Social Work Study and Its Interventionayu fitrianiNoch keine Bewertungen
- Ramadan and Diabetes MCB DiabetesUK LeafletDokument4 SeitenRamadan and Diabetes MCB DiabetesUK LeafletChris MulyoNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (42)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4.5 von 5 Sternen4.5/5 (6)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceVon EverandTo Explain the World: The Discovery of Modern ScienceBewertung: 3.5 von 5 Sternen3.5/5 (51)
- Critical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsVon EverandCritical Thinking: How to Effectively Reason, Understand Irrationality, and Make Better DecisionsBewertung: 4.5 von 5 Sternen4.5/5 (39)
- The Marshmallow Test: Mastering Self-ControlVon EverandThe Marshmallow Test: Mastering Self-ControlBewertung: 4.5 von 5 Sternen4.5/5 (60)
- Dark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingVon EverandDark Psychology: Learn To Influence Anyone Using Mind Control, Manipulation And Deception With Secret Techniques Of Dark Persuasion, Undetected Mind Control, Mind Games, Hypnotism And BrainwashingBewertung: 4 von 5 Sternen4/5 (1138)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)