Das könnte Ihnen auch gefallen
- Medicine For Children: Homeopathy and Anthroposophic Medicine in Paediatric UseDokument28 SeitenMedicine For Children: Homeopathy and Anthroposophic Medicine in Paediatric UseAbu ShahadatNoch keine Bewertungen
- Well-Child Care in Infancy: Promoting Readiness for LifeVon EverandWell-Child Care in Infancy: Promoting Readiness for LifeNoch keine Bewertungen
- Childhood Antecedents To Adult Cardiovascular Disease (PedRev2012)Dokument13 SeitenChildhood Antecedents To Adult Cardiovascular Disease (PedRev2012)jose matosNoch keine Bewertungen
- Positive Mental Health, Fighting Stigma and Promoting Resiliency for Children and AdolescentsVon EverandPositive Mental Health, Fighting Stigma and Promoting Resiliency for Children and AdolescentsNoch keine Bewertungen
- Health Education WilsonDokument6 SeitenHealth Education WilsonMark RobinsonNoch keine Bewertungen
- Therapist's Guide to Pediatric Affect and Behavior RegulationVon EverandTherapist's Guide to Pediatric Affect and Behavior RegulationNoch keine Bewertungen
- Unit 7 Preventive PediatricsDokument16 SeitenUnit 7 Preventive PediatricsSanthosh.S.U58% (12)
- Lancet 2011 - Papers 1 and 2 PDFDokument31 SeitenLancet 2011 - Papers 1 and 2 PDFpyeohhpyeNoch keine Bewertungen
- Dworkin 2016Dokument11 SeitenDworkin 2016Yunita Gabriela MaduNoch keine Bewertungen
- Preventive 1Dokument4 SeitenPreventive 1Navu Dhaliwal83% (6)
- 262 Gmbidahmetmtoreniyazk: General Issues of Pediatric Service and Child CareDokument28 Seiten262 Gmbidahmetmtoreniyazk: General Issues of Pediatric Service and Child CareKymbat’s LifeNoch keine Bewertungen
- Downs SyndromeDokument69 SeitenDowns Syndromemiqbaljuher100% (1)
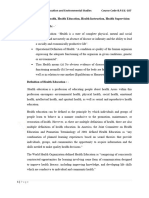
- 1.2 Definition of Health Health Education Health Instruction Health SupervisionDokument4 Seiten1.2 Definition of Health Health Education Health Instruction Health Supervisionbeherasrimanta43Noch keine Bewertungen
- Pediatric Hospital PresentationDokument61 SeitenPediatric Hospital PresentationLindsay Khryss Cendy MadahanNoch keine Bewertungen
- The Science of NeglectDokument20 SeitenThe Science of NeglectdrdrtsaiNoch keine Bewertungen
- Milestones in Public HealthDokument279 SeitenMilestones in Public HealthRick Leung83% (6)
- How To Write A Public Health Research PaperDokument8 SeitenHow To Write A Public Health Research Paperwqbdxbvkg100% (1)
- Developmental Milestones Motor Development - Peds Rev 2010Dokument13 SeitenDevelopmental Milestones Motor Development - Peds Rev 2010Carolina SanchezNoch keine Bewertungen
- Why Study Global Health?: Amatya A, Basel PDokument2 SeitenWhy Study Global Health?: Amatya A, Basel PRika AskiaNoch keine Bewertungen
- Breastfeeding: Updated: June 2017Dokument38 SeitenBreastfeeding: Updated: June 2017Osmely PiñaNoch keine Bewertungen
- Developmental Biology: Understanding Normal and Abnormal DevelopmentDokument17 SeitenDevelopmental Biology: Understanding Normal and Abnormal DevelopmentChetan GopalNoch keine Bewertungen
- Committee Opinion: The Initial Reproductive Health VisitDokument5 SeitenCommittee Opinion: The Initial Reproductive Health VisitM Fathur Arief KurniawanNoch keine Bewertungen
- Paediatric NursingDokument37 SeitenPaediatric NursingbusizooriNoch keine Bewertungen
- The Child-Friendly Healthcare Initiative (CFHI) : Healthcare Provision in Accordance With The UN Convention On The Rights of The ChildDokument13 SeitenThe Child-Friendly Healthcare Initiative (CFHI) : Healthcare Provision in Accordance With The UN Convention On The Rights of The Childvolt_volticsNoch keine Bewertungen
- Handbook of Life Course Health DevelopmentDokument667 SeitenHandbook of Life Course Health DevelopmentCait KantorNoch keine Bewertungen
- Cfhi ManualDokument160 SeitenCfhi Manualapi-246003035Noch keine Bewertungen
- ECD National Strategy Proof Read 13022017 EN PDFDokument37 SeitenECD National Strategy Proof Read 13022017 EN PDFAbdulkadir NuhNoch keine Bewertungen
- Child Life ArticleDokument10 SeitenChild Life ArticleGlody VuangaNoch keine Bewertungen
- Definition of A Pediatrician: Pediatrics April 2015Dokument5 SeitenDefinition of A Pediatrician: Pediatrics April 2015Fiqri VengeanceHanerNoch keine Bewertungen
- Pedia Handout IDokument135 SeitenPedia Handout IMarwahNoch keine Bewertungen
- College of of Midwifery I. Course Name: Early Childhood Care II. Course OverviewDokument43 SeitenCollege of of Midwifery I. Course Name: Early Childhood Care II. Course OverviewmelpayangsNoch keine Bewertungen
- Diseases of Children in The Subtropics and TropicsDokument1.092 SeitenDiseases of Children in The Subtropics and TropicscaptaincandyNoch keine Bewertungen
- Six MinuteDokument112 SeitenSix Minutenavuru5kNoch keine Bewertungen
- Adolescent Medicine PDFDokument292 SeitenAdolescent Medicine PDFpblsvraman100% (1)
- Reproductive Health: 4.1 R H - P SDokument10 SeitenReproductive Health: 4.1 R H - P SMamataMaharanaNoch keine Bewertungen
- Reproductive Health: 4.1 R H - P SDokument10 SeitenReproductive Health: 4.1 R H - P SVikram SkNoch keine Bewertungen
- Ni Hms 596642Dokument29 SeitenNi Hms 596642putrideasNoch keine Bewertungen
- Principles and Practice of Pediatric Sleep MedicineDokument404 SeitenPrinciples and Practice of Pediatric Sleep MedicinemariajonesmilesNoch keine Bewertungen
- Classification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMDokument2 SeitenClassification and Management of Feeding Difficulties in Children HO11-004 - E - With - WMCarlos GonzalezNoch keine Bewertungen
- Impacto Psicossocial Do CancroDokument8 SeitenImpacto Psicossocial Do CancroForasteiro ZenNoch keine Bewertungen
- Unesco - Eolss Sample Chapters: Maternal and Child Health: A Basic Part of Public HealthDokument9 SeitenUnesco - Eolss Sample Chapters: Maternal and Child Health: A Basic Part of Public HealthAlma WrbNoch keine Bewertungen
- The F-Words' in Childhood Disability - I Swear This IsDokument7 SeitenThe F-Words' in Childhood Disability - I Swear This IsPavel Antonovich Cuevas ZhbankovNoch keine Bewertungen
- Pediatric Critical Care Medicine: EditorsDokument269 SeitenPediatric Critical Care Medicine: EditorsCk1NhiKhoa2020 chuyenkhoaNoch keine Bewertungen
- The Problem: (Insert Citation)Dokument52 SeitenThe Problem: (Insert Citation)Trisha100% (1)
- Epidemiological Aspects of Maternal and Child Health and Its Issues Word ContentDokument40 SeitenEpidemiological Aspects of Maternal and Child Health and Its Issues Word ContentNimi Simon100% (2)
- Clinical Guide To Pediatric Sleep, A Diagnosis and Management of Sleep Problems 3rdDokument286 SeitenClinical Guide To Pediatric Sleep, A Diagnosis and Management of Sleep Problems 3rdchucrallah1968Noch keine Bewertungen
- Intro To PHPDokument18 SeitenIntro To PHPHajra MirzaNoch keine Bewertungen
- Viewpoint Article: Childhood Obesity - Looking Back Over 50 Years To Begin To Look ForwardDokument5 SeitenViewpoint Article: Childhood Obesity - Looking Back Over 50 Years To Begin To Look ForwardichalsajaNoch keine Bewertungen
- Unit 1Dokument22 SeitenUnit 1Amosh JowelNoch keine Bewertungen
- Paediatrics Notes-2017 BatchDokument102 SeitenPaediatrics Notes-2017 BatchMohan EthirajanNoch keine Bewertungen
- Health Book For TeachersDokument281 SeitenHealth Book For TeachersRene H. Framcisco, MD100% (2)
- Level of Awareness of Post Partum Mothers On Newborn Screening EssaysDokument4 SeitenLevel of Awareness of Post Partum Mothers On Newborn Screening EssaysJig GamoloNoch keine Bewertungen
- Adolescent HealthDokument3 SeitenAdolescent HealthIJAR JOURNALNoch keine Bewertungen
- 3 Year Paediatric Assignment One: Department NursingDokument12 Seiten3 Year Paediatric Assignment One: Department NursingmekdesNoch keine Bewertungen
- Nast - Pages From P.S. Ocampo Handbook of Well Child Care - 132Dokument11 SeitenNast - Pages From P.S. Ocampo Handbook of Well Child Care - 132einjohnmNoch keine Bewertungen
- 1 - Perspective of Child HealthDokument29 Seiten1 - Perspective of Child Healthamosae909Noch keine Bewertungen
- 1.modern Concepts of Child CareDokument18 Seiten1.modern Concepts of Child Caretanmai noolu100% (1)
- Management of Children With Short Stature: Pediatric Oncall April 2019Dokument9 SeitenManagement of Children With Short Stature: Pediatric Oncall April 2019Rahmadi SartivanNoch keine Bewertungen
- Critical Care Nursing ClinicsDokument133 SeitenCritical Care Nursing ClinicsJune DumdumayaNoch keine Bewertungen
- Formal Language Theory: Refining The Chomsky Hierarchy: Gerhard J Ager & James RogersDokument29 SeitenFormal Language Theory: Refining The Chomsky Hierarchy: Gerhard J Ager & James RogersAna Paula Dantas PassosNoch keine Bewertungen
- Hollywood Edge Premier Edition Sound Effects Vol 1 - 4Dokument327 SeitenHollywood Edge Premier Edition Sound Effects Vol 1 - 4Ana Paula Dantas PassosNoch keine Bewertungen
- Complexity of Natural Languages - ChomskyDokument29 SeitenComplexity of Natural Languages - ChomskyAna Paula Dantas PassosNoch keine Bewertungen
- THX Home Audio Buyer GuideDokument6 SeitenTHX Home Audio Buyer GuideAna Paula Dantas PassosNoch keine Bewertungen
- THX Speaker Layout and Baffle WallDokument4 SeitenTHX Speaker Layout and Baffle WallAna Paula Dantas PassosNoch keine Bewertungen
- THX Certified Studio SpecificationsDokument5 SeitenTHX Certified Studio SpecificationsAna Paula Dantas Passos0% (1)
- As Raízes Do Dolby StereoDokument7 SeitenAs Raízes Do Dolby StereoAna Paula Dantas PassosNoch keine Bewertungen
- Artistic Intuition Within Cassirer S Sys PDFDokument45 SeitenArtistic Intuition Within Cassirer S Sys PDFAna Paula Dantas PassosNoch keine Bewertungen
- DEVELOPMENT-how 12mo Remember ObjectsDokument5 SeitenDEVELOPMENT-how 12mo Remember ObjectsAna Paula Dantas PassosNoch keine Bewertungen
- The Scientist-What Do New Neurons in The Brains of Adults Actually DoDokument8 SeitenThe Scientist-What Do New Neurons in The Brains of Adults Actually DoAna Paula Dantas PassosNoch keine Bewertungen
- Childrens Peer Culture - CorsaroDokument25 SeitenChildrens Peer Culture - CorsaroAna Paula Dantas PassosNoch keine Bewertungen
- SMEDA Montessori School PDFDokument18 SeitenSMEDA Montessori School PDFAna Paula Dantas PassosNoch keine Bewertungen
- Visual SchedulesDokument2 SeitenVisual Schedulesapi-362784633Noch keine Bewertungen
- BBC Learning English Disabled DollDokument4 SeitenBBC Learning English Disabled DollSot MaeNoch keine Bewertungen
- CDP Project ReportDokument10 SeitenCDP Project ReportUday SaiNoch keine Bewertungen
- Questions About Anya - Vineland ExerciseDokument2 SeitenQuestions About Anya - Vineland ExerciseJuliana NovaNoch keine Bewertungen
- Behavioural Assessment Scales For Adult LivingDokument112 SeitenBehavioural Assessment Scales For Adult LivingMeeta MathurNoch keine Bewertungen
- Robert L. Collins v. Shirley S. Chater, Commissioner of Social Security Administration, 108 F.3d 341, 10th Cir. (1997)Dokument3 SeitenRobert L. Collins v. Shirley S. Chater, Commissioner of Social Security Administration, 108 F.3d 341, 10th Cir. (1997)Scribd Government DocsNoch keine Bewertungen
- Prevalence of Chronic Health ConditionsDokument27 SeitenPrevalence of Chronic Health ConditionsЯковлев АлександрNoch keine Bewertungen
- Make The Most Out of Your Child's PWD I.D by Familiarizing Yourself With The Benefits That Come With It. Learn More About The Updated List For 2017, HereDokument17 SeitenMake The Most Out of Your Child's PWD I.D by Familiarizing Yourself With The Benefits That Come With It. Learn More About The Updated List For 2017, HereChito Zoleta Jr.Noch keine Bewertungen
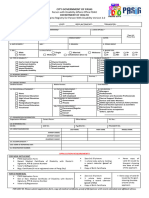
- PWDApplication FormDokument2 SeitenPWDApplication FormJames LorenzoNoch keine Bewertungen
- Dental Management of Children With Special Health Care Needs (SHCN) - A ReviewDokument16 SeitenDental Management of Children With Special Health Care Needs (SHCN) - A ReviewkurniatyNoch keine Bewertungen
- Challenges Faced Children With Disability and Their Families11Dokument10 SeitenChallenges Faced Children With Disability and Their Families11Samira HassanNoch keine Bewertungen
- Developmental MilestonesDokument22 SeitenDevelopmental MilestonesSillmark Bacason100% (3)
- NameDokument5 SeitenNameJuveylyn Cabachete0% (1)
- Asd Sensory - Carti Despre AutismDokument4 SeitenAsd Sensory - Carti Despre Autismioan_paul_puha100% (2)
- Personal Details: The Respondent's Email (Fabiars.100.stud@cdd - Edu.ph) Was Recorded On Submission of This FormDokument23 SeitenPersonal Details: The Respondent's Email (Fabiars.100.stud@cdd - Edu.ph) Was Recorded On Submission of This FormRYAN FABIANoch keine Bewertungen
- Description: Tags: Appendix-A-Pt1Dokument252 SeitenDescription: Tags: Appendix-A-Pt1anon-909384Noch keine Bewertungen
- Handicapped ChildDokument67 SeitenHandicapped ChildAhsan Ul Kayum BhuiyanNoch keine Bewertungen
- What's New With DSM 5? (Formerly Known As DSM V) : 1 Credit Continuing Education CourseDokument15 SeitenWhat's New With DSM 5? (Formerly Known As DSM V) : 1 Credit Continuing Education CourseTodd Finnerty44% (9)
- Clinical Characteristics of Intellectual Disabilities - Mental Disorders and Disabilities Among Low-Income Children - NCBI BookshelfDokument6 SeitenClinical Characteristics of Intellectual Disabilities - Mental Disorders and Disabilities Among Low-Income Children - NCBI BookshelfArhatya MarsasinaNoch keine Bewertungen
- ED 101 Module 11 Infants and ToddlersDokument37 SeitenED 101 Module 11 Infants and ToddlersCreamy VanillaNoch keine Bewertungen
- DysgraphiaDokument10 SeitenDysgraphiaNajiha ZainalNoch keine Bewertungen
- Typology of Learners With Special Needs: Learning OutcomesDokument58 SeitenTypology of Learners With Special Needs: Learning OutcomesEzraNoch keine Bewertungen
- Prof-Ed3-3 MODULE 6 EVALDokument3 SeitenProf-Ed3-3 MODULE 6 EVALDesame Bohol Miasco SanielNoch keine Bewertungen
- Camp ScheduleDokument160 SeitenCamp ScheduleadityavalmikiNoch keine Bewertungen
- CH 1Dokument3 SeitenCH 1api-241345040Noch keine Bewertungen
- KVS TGT 2016 Typing (English) - Watermark - pdf-78Dokument12 SeitenKVS TGT 2016 Typing (English) - Watermark - pdf-78Rishabh SaxenqNoch keine Bewertungen
- Review of Related Literature: La Consolacion College Manila Mendiola, ManilaDokument18 SeitenReview of Related Literature: La Consolacion College Manila Mendiola, ManilaEarl CecilioNoch keine Bewertungen
- Adapt and Validation Leisure InventoryDokument10 SeitenAdapt and Validation Leisure InventoryALBA AZA HERNÁNDEZNoch keine Bewertungen
- Inclusion WorksDokument94 SeitenInclusion WorksAlvaro MejiaNoch keine Bewertungen
- Gravina Et Al. - 2018 - A Literature Review of Organizational Behavior Management Interventions in Human Service Settings From 1990 To 2-AnnotatedDokument51 SeitenGravina Et Al. - 2018 - A Literature Review of Organizational Behavior Management Interventions in Human Service Settings From 1990 To 2-AnnotatedIgorBaptistaNoch keine Bewertungen
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Von EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Bewertung: 3 von 5 Sternen3/5 (1)
- The 7 Habits of Highly Effective People: The Infographics EditionVon EverandThe 7 Habits of Highly Effective People: The Infographics EditionBewertung: 4 von 5 Sternen4/5 (2475)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionVon EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionBewertung: 4 von 5 Sternen4/5 (404)
- The Age of Magical Overthinking: Notes on Modern IrrationalityVon EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityBewertung: 4 von 5 Sternen4/5 (32)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedVon EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedBewertung: 4.5 von 5 Sternen4.5/5 (82)
- The Comfort of Crows: A Backyard YearVon EverandThe Comfort of Crows: A Backyard YearBewertung: 4.5 von 5 Sternen4.5/5 (23)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsVon EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsBewertung: 4 von 5 Sternen4/5 (4)
- The Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsVon EverandThe Garden Within: Where the War with Your Emotions Ends and Your Most Powerful Life BeginsNoch keine Bewertungen
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDVon EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDBewertung: 5 von 5 Sternen5/5 (3)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsVon EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNoch keine Bewertungen
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeVon EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeBewertung: 2 von 5 Sternen2/5 (1)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesVon EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesBewertung: 4.5 von 5 Sternen4.5/5 (1412)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsVon EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsBewertung: 4.5 von 5 Sternen4.5/5 (170)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsVon EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsBewertung: 5 von 5 Sternen5/5 (1)
- The Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeVon EverandThe Twentysomething Treatment: A Revolutionary Remedy for an Uncertain AgeBewertung: 4.5 von 5 Sternen4.5/5 (2)
- The Obesity Code: Unlocking the Secrets of Weight LossVon EverandThe Obesity Code: Unlocking the Secrets of Weight LossBewertung: 4 von 5 Sternen4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaVon EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisVon EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Von EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Bewertung: 4.5 von 5 Sternen4.5/5 (110)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisVon EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisBewertung: 4.5 von 5 Sternen4.5/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessVon EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessBewertung: 4.5 von 5 Sternen4.5/5 (328)
- Why We Die: The New Science of Aging and the Quest for ImmortalityVon EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityBewertung: 4.5 von 5 Sternen4.5/5 (6)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeVon EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeBewertung: 4.5 von 5 Sternen4.5/5 (254)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainVon EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainBewertung: 4 von 5 Sternen4/5 (95)