Das könnte Ihnen auch gefallen
- Scope of RegulationDokument6 SeitenScope of RegulationHisham MaassaraniNoch keine Bewertungen
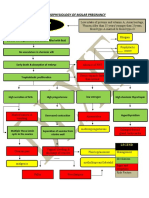
- Partial Mole or Complete Mole: Pathophysiology of Molar PregnancyDokument1 SeitePartial Mole or Complete Mole: Pathophysiology of Molar PregnancyKristian Karl Bautista Kiw-isNoch keine Bewertungen
- Healthcare ProfessionalsDokument30 SeitenHealthcare ProfessionalsAchmad R. MuttaqienNoch keine Bewertungen
- Unit 1 (C) Nursing ProcessDokument43 SeitenUnit 1 (C) Nursing ProcessSumaira NoreenNoch keine Bewertungen
- Jewish Home of CNY Inspection ReportDokument60 SeitenJewish Home of CNY Inspection ReportJames MulderNoch keine Bewertungen
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Neonatal Jaundice: Miriti M.D Master of Clinical Medicine:Accidents and Emerrgency MAY 2018Dokument25 SeitenNeonatal Jaundice: Miriti M.D Master of Clinical Medicine:Accidents and Emerrgency MAY 2018Dennis MiritiNoch keine Bewertungen
- Nursing Care Plan: Subjective Data: Short Term IndependentDokument5 SeitenNursing Care Plan: Subjective Data: Short Term IndependentIrish May SignioNoch keine Bewertungen
- New Born NCPDokument8 SeitenNew Born NCPCarl Vincent Marrion Rejuso100% (1)
- Milestones of Fetal Growth and Development Power PointDokument24 SeitenMilestones of Fetal Growth and Development Power PointCymilo100% (1)
- Nursing Care Plan 1Dokument12 SeitenNursing Care Plan 1Disyme Duron AzuresNoch keine Bewertungen
- OB Care Plan: Assessment DataDokument9 SeitenOB Care Plan: Assessment Dataapi-520841770Noch keine Bewertungen
- Assessment Diagnosis Rationale Planning Intervention Rationale EvaluationDokument2 SeitenAssessment Diagnosis Rationale Planning Intervention Rationale Evaluationbambem aevanNoch keine Bewertungen
- Nursing Care Plan: Nikolai P. Funcion, FSUU-SNDokument5 SeitenNursing Care Plan: Nikolai P. Funcion, FSUU-SNNikolai FuncionNoch keine Bewertungen
- Nursing Care Plan For Labor and Delivery Stages of Labor Diagnosis Intervention Rationale IndependentDokument7 SeitenNursing Care Plan For Labor and Delivery Stages of Labor Diagnosis Intervention Rationale IndependentCLARISSE GEMROSE CUÑADANoch keine Bewertungen
- Role of Research, Leadership and ManagementDokument21 SeitenRole of Research, Leadership and Managementchaitali shankarNoch keine Bewertungen
- Stakeholder Engagement Plan Guide and TemplateDokument3 SeitenStakeholder Engagement Plan Guide and TemplateDan RadaNoch keine Bewertungen
- Nursing Care Plan For Interrupted Breastfeeding NCPDokument3 SeitenNursing Care Plan For Interrupted Breastfeeding NCPSaira SucgangNoch keine Bewertungen
- Maternity Care Plan - Template 1 - 21 - 09Dokument9 SeitenMaternity Care Plan - Template 1 - 21 - 09Steven BerschaminskiNoch keine Bewertungen
- Community Health Nursing Process0Dokument59 SeitenCommunity Health Nursing Process0Mukul Thakur100% (1)
- Care of The Mother, Child and Adolescent (Well Client) Related Learning ExperienceDokument7 SeitenCare of The Mother, Child and Adolescent (Well Client) Related Learning ExperienceIvy VillalobosNoch keine Bewertungen
- Care of Mother, Child, and Adolescents (Well Clients) NCM - 107 Nursing Care Plan Assessment Diagnosis Plan Intervention EvaluationDokument4 SeitenCare of Mother, Child, and Adolescents (Well Clients) NCM - 107 Nursing Care Plan Assessment Diagnosis Plan Intervention EvaluationSophia Caisip100% (1)
- Nursing Care Plans - NurseryDokument4 SeitenNursing Care Plans - NurserySusie PadaoanNoch keine Bewertungen
- Postpartum Care Plan New BornDokument10 SeitenPostpartum Care Plan New BornUche Edwards-ShahidNoch keine Bewertungen
- NCP Case 1Dokument6 SeitenNCP Case 1boomer SeargeNoch keine Bewertungen
- PREECLAMPSIA Case ScenarioDokument2 SeitenPREECLAMPSIA Case Scenariosabao kizuiteNoch keine Bewertungen
- Neonatal JaundiceDokument12 SeitenNeonatal JaundiceJustine NyangaresiNoch keine Bewertungen
- Activity Intolerance R/T Increased Energy Demands Due To Disease Condition and Increased Fetal Nutrient UptakeDokument8 SeitenActivity Intolerance R/T Increased Energy Demands Due To Disease Condition and Increased Fetal Nutrient UptakeAbdelmar SusulanNoch keine Bewertungen
- NCP - Preeclampsia (A)Dokument6 SeitenNCP - Preeclampsia (A)Ronel ResurricionNoch keine Bewertungen
- Dysfunctional Uterine Bleeding (DUB)Dokument1 SeiteDysfunctional Uterine Bleeding (DUB)Bheru LalNoch keine Bewertungen
- Discharge PlanningDokument2 SeitenDischarge PlanningAthena Irish LastimosaNoch keine Bewertungen
- Personal-Soc Interpretation: Tower of 4 CubesDokument15 SeitenPersonal-Soc Interpretation: Tower of 4 CubesteuuuuNoch keine Bewertungen
- Nursing Diagnosis Rationale Goals/ Objectives Nursing Intervention S Rational E EvaluationDokument21 SeitenNursing Diagnosis Rationale Goals/ Objectives Nursing Intervention S Rational E EvaluationJoanne Bernadette Aguilar100% (1)
- Week 2 NCM 107Dokument21 SeitenWeek 2 NCM 107raise concern100% (1)
- NCP Example Pre EclampsiaDokument6 SeitenNCP Example Pre EclampsiaChristian Joseph OpianaNoch keine Bewertungen
- Unit 1: Introduction To Community Health Nursing Chapter 1: Fundamental Concepts of Community Health NursingDokument140 SeitenUnit 1: Introduction To Community Health Nursing Chapter 1: Fundamental Concepts of Community Health NursingChevelle Valenciano-GaanNoch keine Bewertungen
- PRELIMS 219 Q - uPDATEDDokument8 SeitenPRELIMS 219 Q - uPDATEDAloha ItsmeNoch keine Bewertungen
- SDL4Dokument2 SeitenSDL4Juviely PremacioNoch keine Bewertungen
- Bottle FeedingDokument2 SeitenBottle Feedingseigelystic100% (5)
- Case (Acute Gastroenteritis) Group 4Dokument36 SeitenCase (Acute Gastroenteritis) Group 4EljhayrosNoch keine Bewertungen
- Atrial Septal Defect - 7 Year OldDokument1 SeiteAtrial Septal Defect - 7 Year OldMSNoch keine Bewertungen
- Labor Nursing Care Plan 1Dokument4 SeitenLabor Nursing Care Plan 1Anna Mae DollenteNoch keine Bewertungen
- Case StudyDokument19 SeitenCase Studywella goNoch keine Bewertungen
- NCP Episiotomy WoundDokument3 SeitenNCP Episiotomy WoundJP2001Noch keine Bewertungen
- NCP - Diabetes Mellitus Prepregnancy/GestationalDokument13 SeitenNCP - Diabetes Mellitus Prepregnancy/GestationalClaudine Christophe100% (1)
- CASE STUDY Acute Pain Related To Laceration 1Dokument29 SeitenCASE STUDY Acute Pain Related To Laceration 1Maria Jessica Dumdum100% (1)
- Discharge PlanDokument9 SeitenDischarge PlanRheynel NietesNoch keine Bewertungen
- NCPDokument4 SeitenNCPMarielle SorianoNoch keine Bewertungen
- School of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Dokument3 SeitenSchool of Health and Allied Health Sciences Nursing Department Self-Directed Learning (Nur 146 - Clinical Area)Duchess Juliane Jose MirambelNoch keine Bewertungen
- Case Pres AutosavedDokument21 SeitenCase Pres AutosavedJaysellePuguonTabijeNoch keine Bewertungen
- Case-Study FinalDokument39 SeitenCase-Study Finalcoosa liquorsNoch keine Bewertungen
- Filipino Cultures, Values, and Practices in Relation To Childbearing and ChildrearingDokument5 SeitenFilipino Cultures, Values, and Practices in Relation To Childbearing and ChildrearingCheriss RollanNoch keine Bewertungen
- Weekly Course Learning Objectives (Postpartum)Dokument4 SeitenWeekly Course Learning Objectives (Postpartum)Reyna Mee AhiyasNoch keine Bewertungen
- Teaching PlanDokument1 SeiteTeaching PlanUnis OwtwoNoch keine Bewertungen
- Reflective Journal 1Dokument4 SeitenReflective Journal 1api-365605511Noch keine Bewertungen
- ConjunctivitisDokument16 SeitenConjunctivitisClark LopezNoch keine Bewertungen
- Viernes, Jemalyn BSN 2-3 Assessment Diagnosis Planning Implementation Rationale EvaluationDokument8 SeitenViernes, Jemalyn BSN 2-3 Assessment Diagnosis Planning Implementation Rationale EvaluationJeMalyn VieRnesNoch keine Bewertungen
- Case Study PIHDokument26 SeitenCase Study PIHChen OmbrosaNoch keine Bewertungen
- Labor Nursing Care PlansDokument58 SeitenLabor Nursing Care PlansMuhamad AriNoch keine Bewertungen
- GonorrheaDokument2 SeitenGonorrheaLeizel ApolonioNoch keine Bewertungen
- CHN Case Analysis Case ScenarioDokument7 SeitenCHN Case Analysis Case ScenarioNathalie kate petallarNoch keine Bewertungen
- PRS Ear Instillation - GlovaDokument3 SeitenPRS Ear Instillation - GlovaAndrea Colleen GlovaNoch keine Bewertungen
- Roxipan (Oxytocin) - Drug StudyDokument4 SeitenRoxipan (Oxytocin) - Drug StudyIzza DeloriaNoch keine Bewertungen
- 10 Nurses Proper Professional EtiquetteDokument1 Seite10 Nurses Proper Professional EtiquetteReva stevanaNoch keine Bewertungen
- University of Northern PhilippinesDokument6 SeitenUniversity of Northern PhilippinesCatherine PradoNoch keine Bewertungen
- Manangan, Eugene B. - FDAR Boggy UterusDokument2 SeitenManangan, Eugene B. - FDAR Boggy UterusGin MananganNoch keine Bewertungen
- Discharge PlanDokument3 SeitenDischarge PlanDranlie LagdamenNoch keine Bewertungen
- NURS 2020H Community Based Nursing PracticeDokument7 SeitenNURS 2020H Community Based Nursing Practiceapi-400554289Noch keine Bewertungen
- ReflectionDokument4 SeitenReflectionapi-400554289Noch keine Bewertungen
- 2020 PosterDokument1 Seite2020 Posterapi-400554289Noch keine Bewertungen
- NURS 2021H Clinical Course Mid-Term Evaluation Progress Course Objective Evidence/Indicators Midterm Evidence/Indicators Final Student: StudentDokument14 SeitenNURS 2021H Clinical Course Mid-Term Evaluation Progress Course Objective Evidence/Indicators Midterm Evidence/Indicators Final Student: Studentapi-400554289Noch keine Bewertungen
- Care PlanDokument3 SeitenCare Planapi-400554289Noch keine Bewertungen
- Psych Videbeck 19Dokument1 SeitePsych Videbeck 19aum311Noch keine Bewertungen
- Exam in MS1 Cope 2nd ExamDokument5 SeitenExam in MS1 Cope 2nd ExamIbrahim RegachoNoch keine Bewertungen
- Salem Hospital Plan of Correction 7-28-11Dokument2 SeitenSalem Hospital Plan of Correction 7-28-11Statesman JournalNoch keine Bewertungen
- Mental Health Nursing Unit 1Dokument9 SeitenMental Health Nursing Unit 1PihuNoch keine Bewertungen
- COPA Model For Competence Quality and Patient SafetyDokument8 SeitenCOPA Model For Competence Quality and Patient SafetyVidya Jayasekaran JNoch keine Bewertungen
- RN or BSN Supervisor or RN Manager or Nurse LeaderDokument2 SeitenRN or BSN Supervisor or RN Manager or Nurse Leaderapi-77971483Noch keine Bewertungen
- Pediatric1 PDFDokument34 SeitenPediatric1 PDFNagomi Hanison0% (1)
- Unit 7 Problem Solving Critical Thinking Creativity and Decision MakingpptDokument127 SeitenUnit 7 Problem Solving Critical Thinking Creativity and Decision Makingpptermais hailuNoch keine Bewertungen
- Labor Law Cases. Set 4.Dokument95 SeitenLabor Law Cases. Set 4.Kiko CorpuzNoch keine Bewertungen
- Learning Disabilities CSTFDokument91 SeitenLearning Disabilities CSTFSandra Gabriela L. OliveiraNoch keine Bewertungen
- Ethical Double Effect ASSIGNMENTDokument5 SeitenEthical Double Effect ASSIGNMENTKrea kristalleteNoch keine Bewertungen
- The Relationship Between Adversity Quotient and CaDokument11 SeitenThe Relationship Between Adversity Quotient and CaAgung PrasetyaNoch keine Bewertungen
- Vol 1 50 TEST IIDokument11 SeitenVol 1 50 TEST IIMaria Zm LatonNoch keine Bewertungen
- Aneka Payne Resume ExcellentDokument2 SeitenAneka Payne Resume Excellentapi-313046203Noch keine Bewertungen
- Easterann K ResumeDokument6 SeitenEasterann K Resumeapi-237186471Noch keine Bewertungen
- A Study of Knowledge & Awareness Regarding HIV / AIDS Among Nursing StudentsDokument5 SeitenA Study of Knowledge & Awareness Regarding HIV / AIDS Among Nursing StudentsenggridNoch keine Bewertungen
- 13 Medical FirstAidDokument14 Seiten13 Medical FirstAidMohammed MinhajNoch keine Bewertungen
- 1 - Understanding Medical TerminologyDokument26 Seiten1 - Understanding Medical TerminologyTia apriliaNoch keine Bewertungen
- Practice Nurse Vacancy Oct 2019Dokument2 SeitenPractice Nurse Vacancy Oct 2019M LubisNoch keine Bewertungen
- ADNEP 8th Joint Annual Convention of PADE and ADNEPDokument2 SeitenADNEP 8th Joint Annual Convention of PADE and ADNEPPhilippineNursingDirectory.com100% (1)
- Outline of Dissertation On ObesityDokument16 SeitenOutline of Dissertation On ObesityLavarn PillaiNoch keine Bewertungen
- Contemporary Nursing Issues Trends and Management 5th Edition Cherry Test BankDokument10 SeitenContemporary Nursing Issues Trends and Management 5th Edition Cherry Test BankChristopherBrownkzntc95% (19)