Das könnte Ihnen auch gefallen
- Infant Colic, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandInfant Colic, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- What is IMCI? Integrated Management of Childhood IllnessDokument30 SeitenWhat is IMCI? Integrated Management of Childhood IllnessteabagmanNoch keine Bewertungen
- Imci Case StudyDokument10 SeitenImci Case StudyRhika Mae Flores Valdez100% (1)
- TH ST TH TH ST TH STDokument7 SeitenTH ST TH TH ST TH STPaul Espinosa0% (3)
- Maternity Nursing Review: Fetal Positioning, Signs of Labor, Weight GainDokument116 SeitenMaternity Nursing Review: Fetal Positioning, Signs of Labor, Weight Gainmale nurse0% (1)
- A Case Study Illustrating Nursing AssessmentDokument9 SeitenA Case Study Illustrating Nursing AssessmentRozen ElizaldeNoch keine Bewertungen
- NCM112 Guide to Perioperative Nursing TermsDokument8 SeitenNCM112 Guide to Perioperative Nursing TermsEdson John DemayoNoch keine Bewertungen
- Problems of The PassengerDokument9 SeitenProblems of The PassengerDanah Grace SanchezNoch keine Bewertungen
- National Leprosy Control Program GoalsDokument7 SeitenNational Leprosy Control Program GoalsAbdurrahim MlntdNoch keine Bewertungen
- Pedia Practice Test With AnswersDokument132 SeitenPedia Practice Test With Answersnycjg15100% (2)
- 5b - NCPDokument7 Seiten5b - NCPKelly Camero ÜNoch keine Bewertungen
- ESSENTIAL NEWBORN CAREDokument5 SeitenESSENTIAL NEWBORN CAREJig PirameNoch keine Bewertungen
- Cough, Cold, Fever Care for InfantsDokument3 SeitenCough, Cold, Fever Care for InfantsFranco Obedoza67% (3)
- Nclex 1Dokument18 SeitenNclex 1Arvin Campos0% (1)
- MCN Test BankDokument10 SeitenMCN Test BankMho Pimentel Vanguardia100% (1)
- IMCIDokument2 SeitenIMCIsweet_lily_valleyNoch keine Bewertungen
- Imci-Integrated Management of Childhood Illness - 1992 - 2 Pilot Areas AreDokument18 SeitenImci-Integrated Management of Childhood Illness - 1992 - 2 Pilot Areas Arej0nna_02Noch keine Bewertungen
- Evolution of Nursing ResearchDokument10 SeitenEvolution of Nursing ResearchStar AlvarezNoch keine Bewertungen
- Newborn Delivery: Immediate Care PrinciplesDokument79 SeitenNewborn Delivery: Immediate Care PrinciplesJr CaniaNoch keine Bewertungen
- COMMUNITY AND MEDICAL HEALTH NURSING QUESTIONSDokument6 SeitenCOMMUNITY AND MEDICAL HEALTH NURSING QUESTIONSJonathan Agcaoili KupahuNoch keine Bewertungen
- Pediatric Nursing Pediatric NursingDokument59 SeitenPediatric Nursing Pediatric Nursingmaj100% (2)
- Workplan Rle JuneDokument18 SeitenWorkplan Rle JuneQueeny Anne Apil33% (3)
- IMCIDokument148 SeitenIMCILloyd Rafael EstabilloNoch keine Bewertungen
- EPI - AND - IMCI - Docx Filename - UTF-8''EPI AND IMCIDokument14 SeitenEPI - AND - IMCI - Docx Filename - UTF-8''EPI AND IMCIYvonne Carmel Aguilar SunigaNoch keine Bewertungen
- Pediatric Nursing 1: Points 100 Questions 100 Time Limit 90 MinutesDokument54 SeitenPediatric Nursing 1: Points 100 Questions 100 Time Limit 90 MinutesSean Lloyd RigonNoch keine Bewertungen
- Discharge Planning FinalDokument5 SeitenDischarge Planning FinalRose AnnNoch keine Bewertungen
- Family Nursing Care PlanDokument19 SeitenFamily Nursing Care Planɹǝʍdןnos95% (43)
- 3 Target Setting Vaccine ComputationDokument5 Seiten3 Target Setting Vaccine ComputationPHOEBE ANN ROCHE100% (1)
- Maternal Nursing and Medical-Surgical ItemsDokument29 SeitenMaternal Nursing and Medical-Surgical ItemsRose JoyNoch keine Bewertungen
- OB Power Point Presentation 002Dokument57 SeitenOB Power Point Presentation 002RitamariaNoch keine Bewertungen
- Ncp-Imbalance NutritionDokument2 SeitenNcp-Imbalance NutritionMariko BarbaNoch keine Bewertungen
- Teaching Plan For Breast FeedingDokument4 SeitenTeaching Plan For Breast FeedingKramSenarevolNoch keine Bewertungen
- CHN and OBDokument91 SeitenCHN and OBJoshua Christian GanNoch keine Bewertungen
- Handouts IMCIDokument5 SeitenHandouts IMCIseigelystic100% (20)
- IMCIDokument3 SeitenIMCIwordlife360Noch keine Bewertungen
- Compre - Maternal Answer KeyDokument8 SeitenCompre - Maternal Answer KeyrabsibalaNoch keine Bewertungen
- MCN SF Chapter 17 QuizDokument3 SeitenMCN SF Chapter 17 QuizKathleen AngNoch keine Bewertungen
- CHNDokument38 SeitenCHNlouie john abila100% (1)
- Administration and Scoring Directions: MMDSTDokument7 SeitenAdministration and Scoring Directions: MMDSTmgerzon100% (2)
- Ob Post TestDokument12 SeitenOb Post TestMho Pimentel VanguardiaNoch keine Bewertungen
- Imci Quiz 1Dokument2 SeitenImci Quiz 1Neptali Cardinal100% (1)
- Nur 1210 Maternal Module #1 Framework For Maternal and Child Health NursingDokument41 SeitenNur 1210 Maternal Module #1 Framework For Maternal and Child Health Nursingaaaaa100% (1)
- Obstetric Sample Questions With RationaleDokument31 SeitenObstetric Sample Questions With RationaleTomzki Cornelio50% (2)
- Idiot's Guide On How To Fail The NleDokument6 SeitenIdiot's Guide On How To Fail The Nlestuffednurse100% (1)
- Name: de Guzman, Cameron Josh B. Section: 2Bsn-ADokument3 SeitenName: de Guzman, Cameron Josh B. Section: 2Bsn-ACameron De GuzmanNoch keine Bewertungen
- Community Health Nursing Exam QuestionsDokument3 SeitenCommunity Health Nursing Exam QuestionsJheanAlphonsineT.MeansNoch keine Bewertungen
- Problem No. 2: Nursing Care of A Family When A Child Needs Diagnostic or Therapeutic ModalitiesDokument20 SeitenProblem No. 2: Nursing Care of A Family When A Child Needs Diagnostic or Therapeutic ModalitiesBrandone Dave ParagosoNoch keine Bewertungen
- Community Health Nursing Chapter 8Dokument6 SeitenCommunity Health Nursing Chapter 8Audrie Allyson GabalesNoch keine Bewertungen
- Family Caseload Presentation Barangay BalagbagDokument6 SeitenFamily Caseload Presentation Barangay BalagbagCharmae NaveaNoch keine Bewertungen
- Nursing Diagnosis For Ante Part Um, Um and PostDokument10 SeitenNursing Diagnosis For Ante Part Um, Um and Postxtn218100% (13)
- IMCI CARE OF THE CHILD Topic 2Dokument10 SeitenIMCI CARE OF THE CHILD Topic 2Hanna Evidente BakalNoch keine Bewertungen
- 1 General Danger SignsDokument33 Seiten1 General Danger SignsAmal AlezabiNoch keine Bewertungen
- Assess and Classify The Sick Child Age 2 Months Up To 5 YearsDokument76 SeitenAssess and Classify The Sick Child Age 2 Months Up To 5 YearsTaniaNoch keine Bewertungen
- Literature Review On Integrated Management of Childhood IllnessDokument4 SeitenLiterature Review On Integrated Management of Childhood Illnesstofonyduv1h2Noch keine Bewertungen
- Pediatric AssessmentDokument16 SeitenPediatric AssessmentWenTzu100% (2)
- IMCIDokument35 SeitenIMCIharutoshippuden0Noch keine Bewertungen
- Oral Exam QuestionsDokument44 SeitenOral Exam Questionseiheme22Noch keine Bewertungen
- 5917365719mod 9 Follow Up RDokument25 Seiten5917365719mod 9 Follow Up RShouvik NathNoch keine Bewertungen
- Imci Cough or DobDokument11 SeitenImci Cough or DobRenz Jian MacasiebNoch keine Bewertungen
- TraumaDokument37 SeitenTraumamgNoch keine Bewertungen
- Surgery - AdrenalsDokument6 SeitenSurgery - AdrenalsmgNoch keine Bewertungen
- ParthenonDokument2 SeitenParthenonmgNoch keine Bewertungen
- OIA Cat MusclesDokument10 SeitenOIA Cat MusclesmgNoch keine Bewertungen
- Dass-21 TemplateDokument2 SeitenDass-21 TemplaterandaifaNoch keine Bewertungen
- Chest Physical Therapy Breathing ExercisesDokument28 SeitenChest Physical Therapy Breathing ExercisesJulia SalvioNoch keine Bewertungen
- CACCN Certification Study Guide Questions Mar 2010Dokument27 SeitenCACCN Certification Study Guide Questions Mar 2010BrittBrattDubb100% (1)
- Dr. Reviono, DR., SP.P (K) - Update Diagnosis and Management JeroveciDokument20 SeitenDr. Reviono, DR., SP.P (K) - Update Diagnosis and Management JeroveciOlivia DwimaswastiNoch keine Bewertungen
- Parenteral Fluid Therapy: Types of Intravenous SolutionDokument18 SeitenParenteral Fluid Therapy: Types of Intravenous SolutionKathleen Joy Costales Magtanong100% (1)
- Advanced Life Support-2021Dokument130 SeitenAdvanced Life Support-2021JA KarmenNoch keine Bewertungen
- Lecture Secondary TuberculosisDokument78 SeitenLecture Secondary TuberculosisslyfoxkittyNoch keine Bewertungen
- NCM 112-Mod3Dokument19 SeitenNCM 112-Mod3Samantha BolanteNoch keine Bewertungen
- Advanced Ventilation ManagementDokument3 SeitenAdvanced Ventilation ManagementAnka EremiaNoch keine Bewertungen
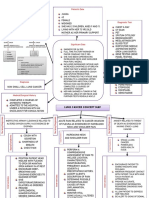
- Lung Cancer Concept Map-Group 2Dokument2 SeitenLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- MSDS Orec OzoneDokument2 SeitenMSDS Orec OzoneHerni SuharniriyantiNoch keine Bewertungen
- Chapter 23 Obstructive Lung Disease Chronic Obstructive Pulmonary DiseaseDokument10 SeitenChapter 23 Obstructive Lung Disease Chronic Obstructive Pulmonary DiseaseZahra Margrette SchuckNoch keine Bewertungen
- Emergency Medicine MCQ AssessmentDokument4 SeitenEmergency Medicine MCQ Assessmenthassanmurtazashah33Noch keine Bewertungen
- COPD GuideDokument69 SeitenCOPD GuideEster Elisabeth WoworNoch keine Bewertungen
- Emergency in Respiratory Medicine HandbookDokument73 SeitenEmergency in Respiratory Medicine HandbookIndra MahaputraNoch keine Bewertungen
- Appeal 2020Dokument79 SeitenAppeal 2020mohammadeidNoch keine Bewertungen
- Veterinary Internal MedicineDokument233 SeitenVeterinary Internal MedicineSulove KoiralaNoch keine Bewertungen
- Health Assessment RLE SAS ANSWERS AND RATIONALEDokument14 SeitenHealth Assessment RLE SAS ANSWERS AND RATIONALEmelocotoncamella100% (2)
- Oxygen Advantage Manual For AthletesDokument31 SeitenOxygen Advantage Manual For AthletesCharles MitchellNoch keine Bewertungen
- Welcome To Abtran - Onsite TrainingDokument16 SeitenWelcome To Abtran - Onsite TrainingJack JonesNoch keine Bewertungen
- Patient Scenario Chapter 20answer SheetDokument6 SeitenPatient Scenario Chapter 20answer SheetcalliemozartNoch keine Bewertungen
- COPD Physiotherapy Management GuideDokument10 SeitenCOPD Physiotherapy Management GuideYamini ChowdaryNoch keine Bewertungen
- Health9 - q1 - Mod4 - Effects of Environmental Issues - v3Dokument22 SeitenHealth9 - q1 - Mod4 - Effects of Environmental Issues - v3HARLEY L. TAN89% (9)
- SFXCS On Site Retreat WaiverDokument1 SeiteSFXCS On Site Retreat WaiverGoldie LascoNoch keine Bewertungen
- Acute Respiratory Distress SyndromeDokument3 SeitenAcute Respiratory Distress Syndromekarenkaren09Noch keine Bewertungen
- Case 4-2021: A 70-Year-Old Woman With Dyspnea On Exertion and Abnormal Findings On Chest ImagingDokument12 SeitenCase 4-2021: A 70-Year-Old Woman With Dyspnea On Exertion and Abnormal Findings On Chest ImagingBruno ConteNoch keine Bewertungen
- Cardiovascular Signs and Symptoms GuideDokument65 SeitenCardiovascular Signs and Symptoms GuideWilliam ApostolNoch keine Bewertungen
- SABER-Nursing Care Plan #1 - JGDokument7 SeitenSABER-Nursing Care Plan #1 - JGJessica MontoyaNoch keine Bewertungen
- Pil 2200016 28112017185241 636474919780156250Dokument4 SeitenPil 2200016 28112017185241 636474919780156250HjkjNoch keine Bewertungen
- Case Study 1 (Pneumonia)Dokument13 SeitenCase Study 1 (Pneumonia)Kate EscotonNoch keine Bewertungen