Beruflich Dokumente
Kultur Dokumente
Combined Tetanus, Diphtheria, and 5-Component Pertussis Vaccine For Use in Adolescents and Adults
Hochgeladen von
atika sgrtOriginaltitel
Copyright
Verfügbare Formate
Dieses Dokument teilen
Dokument teilen oder einbetten
Stufen Sie dieses Dokument als nützlich ein?
Sind diese Inhalte unangemessen?
Dieses Dokument meldenCopyright:
Verfügbare Formate
Combined Tetanus, Diphtheria, and 5-Component Pertussis Vaccine For Use in Adolescents and Adults
Hochgeladen von
atika sgrtCopyright:
Verfügbare Formate
ORIGINAL CONTRIBUTION
Combined Tetanus, Diphtheria,
and 5-Component Pertussis Vaccine
for Use in Adolescents and Adults
Michael E. Pichichero, MD Context Increasing reports of pertussis among US adolescents, adults, and their in-
Margaret B. Rennels, MD fant contacts have stimulated vaccine development for older age groups.
Kathryn M. Edwards, MD Objective To assess the immunogenicity and reactogenicity of a tetanus-diphtheria
Mark M. Blatter, MD 5-component (pertussis toxoid, filamentous hemagglutinin, pertactin, and fimbriae types
2 and 3) acellular pertussis vaccine (Tdap) in adolescents and adults.
Gary S. Marshall, MD
Design, Setting, and Participants A prospective, randomized, modified double-
Monica Bologa, MD, MS blind, comparative trial was conducted in healthy adolescents and adults aged 11 through
Elaine Wang, MD 64 years from August 2001 to August 2002 at 39 US clinical centers.
Elaine Mills, MD Interventions A single 0.5-mL intramuscular dose of either Tdap or tetanus-
diphtheria vaccine (Td).
I
N 2003, 11 647 CASES OF PERTUS- Main Outcome Measures Antibody titers to diphtheria and tetanus toxoids for
sis, many in adolescents and adults, Tdap and Td were measured in sera collected from subsets of adolescents and adults,
before and 28 days after vaccination. For pertussis antigens, titers in sera from Tdap
were reported to the US Centers for
vaccinees were assessed vs those from infants who received analogous pediatric diph-
Disease Control and Prevention theria-tetanus-acellular pertussis vaccine (DTaP) in a previous efficacy trial. Safety was
(CDC).1,2 Preliminary CDC data for assessed via solicited local and systemic reactions for 14 days and adverse events for
2004 indicate an increase to 18 957 6 months following vaccination.
cases.3 Although increased awareness Results A total of 4480 participants were enrolled. For both Tdap and Td, more than
and improved diagnostic methods may 94% and nearly 100% of vaccinees had protective antibody concentrations of at least
increase reporting, factors such as the 0.1 IU/mL for diphtheria and tetanus, respectively. Geometric mean antibody titers to
variable efficacy of whole-cell pertus- pertussis toxoid, filamentous hemagglutinin, pertactin, and fimbriae types 2 and 3 ex-
sis vaccines previously used in the ceeded (by 2.1 to 5.4 times) levels in infants following immunization at 2, 4, and 6
United States,4,5 undervaccination in months with DTaP. The incidence of solicited local and systemic reactions and ad-
childhood, and waning immunity in verse events was generally similar between the Tdap and Td groups.
adolescents and adults may also ex- Conclusions This Tdap vaccine elicited robust immune responses in adolescents and
plain an increase in incidence. Incom- adults to pertussis, tetanus, and diphtheria antigens, while exhibiting an overall safety
pletely immunized infants and tod- profile similar to that of a licensed Td vaccine. These data support the potential rou-
dlers have the highest susceptibility to tine use of this Tdap vaccine in adolescents and adults.
pertussis, the most severe disease mani- JAMA. 2005;293:3003-3011 www.jama.com
festations, and highest risk of mortal-
ity.6,7 Reported cases of pertussis de- The role of adolescents and adults in Author Affiliations: University of Rochester Medical
cline after completion of the primary the spread of pertussis is critical. Dis- Center, Rochester, NY (Dr Pichichero); University of
infant immunization series and re- ease may be characterized by nonclas- Maryland, Baltimore (Dr Rennels); Vanderbilt Univer-
sity, Nashville, Tenn (Dr Edwards); Primary Physi-
main low until early adolescence, when sical symptoms, making diagnosis more cians Research, Pittsburgh, Pa (Dr Blatter); University
the number of cases increases. Be- difficult, particularly given the limita- of Louisville, Louisville, Ky (Dr Marshall); Sanofi Pas-
teur Limited, Toronto, Ontario (Drs Bologa, Wang, and
cause no booster pertussis vaccine is tions of available diagnostic tests. How- Mills).
currently available for adolescents or ever, adolescents and adults who con- Corresponding Author: Michael E. Pichichero, MD,
University of Rochester Medical Center, Elmwood Pe-
adults, these persons become increas- tract pertussis do experience significant diatric Group, 601 Elmwood Ave, Rochester, NY 14642
ingly vulnerable to the disease.8 morbidity and complications.9,10 De- (michael_pichichero@urmc.rochester.edu).
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, June 22/29, 2005—Vol 293, No. 24 3003
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
layed treatment and increased trans- ciency, malignancy, significant under- phate (0.33 mg aluminum); and 0.6%
mission,8,11 most significantly to un- lying disease, neurological impair- 2-phenoxyethanol per 0.5-mL dose.
vaccinated or undervaccinated infants, ment, or pregnancy. The control vaccine, Td, was a li-
are of concern.12,13 Vaccination of ado- censed product containing 2 Lf of diph-
lescents and adults with acellular per- Trial Design theria toxoid; 5 Lf of tetanus toxoid; 1.5
tussis vaccines might reduce both the This phase 3, randomized, controlled, mg of aluminum phosphate (0.33 mg
morbidity associated with the disease modified double-blind trial was con- aluminum); and 0.01% thimerosal as a
in these populations and transmission ducted at 39 US clinical centers preservative per 0.5-mL dose.
to their household and other contacts, (FIGURE 1). To maintain blinding, study
especially infants. We describe the im- center personnel who administered vac- Laboratory Methods
munogenicity and reactogenicity of a cines did not perform study assess- Antibody assays were performed in a
new 5-component acellular pertussis ments, while those who performed as- blinded manner at the clinical immu-
vaccine combined with tetanus and sessments remained blinded to study nology laboratories of Sanofi Pasteur
diphtheria toxoids (Tdap; Adacel, Sa- vaccines. Study sponsor personnel, who Limited in Toronto, Ontario (for per-
nofi Pasteur Limited, Toronto, On- did not participate further in the trial, tussis antigens) or Sanofi Pasteur Inc in
tario) in adolescents and adults. provided a computer-generated ran- Swiftwater, Pa (for tetanus and diph-
domization list, including designation theria toxoids) using validated meth-
METHODS of random assignments to provide se- ods.14-16 Antipertussis, anti–filamen-
We examined the immunogenicity and rum samples, to a central randomiza- tous hemagglutinin, anti–fimbriae types
reactogenicity of booster doses of Tdap tion center at the CRO. Vaccine allo- 2 and 3, antipertactin IgG, and antiteta-
vs those of licensed tetanus and diph- cation codes were obtained from an nus antibody titers were determined by
theria toxoids adsorbed for adult use interactive voice response system at the an enzyme-linked immunosorbent as-
(Td, Sanofi Pasteur Inc, Swiftwater, Pa). CRO; an allocation code list was pro- say (ELISA) method. Results for pertus-
The trial was conducted following the vided in a sealed envelope by the spon- sis antibodies were calculated in ELISA
principles outlined in the Declaration sor. The success of blinding at each site units per milliliter (EU/mL) by com-
of Helsinki. Written informed con- was evaluated during routine monitor- parison with in-house standard anti-
sent was obtained from participants, ing. Participants were randomized to re- sera of assigned unitage, calibrated to the
their parents, or guardians before study ceive Tdap or Td (3:2 for adolescents; US Human Reference Lots 3 or 4. Per-
procedures were initiated. Written in- 3:1 for adults). To ensure adequate dis- tussis antibody response comparisons
formed assents were obtained for un- tribution across groups, enrollment was were made using serum samples col-
derage adolescents, as required by in- stratified by age (11-13, 14-17, 18-28, lected at 7 months of age, following im-
stitutional review boards (IRBs). 29-48, and 49-64 years; block size was munization at 2, 4, and 6 months of age,
Appropriate IRBs approved study docu- 10 for adolescents and 8 for adults). Se- from infant participants in an efficacy
ments at each center. A data and safety rum samples were collected immedi- trial using analogous pediatric diphthe-
monitoring board monitored study data ately prior to and 28 to 42 days follow- ria-tetanus 5-component-acellular per-
throughout. A contract research orga- ing study vaccination from randomly tussis vaccine (DTaP; Daptacel, Sanofi
nization (CRO) performed some study selected participant subsets represent- Pasteur Limited).4 The infant serum
monitoring under the supervision of the ing 50% of Tdap recipients, 75% of ado- samples from this reference trial were
sponsor. lescent Td recipients, and 100% of adult concurrently tested in the same labora-
Td recipients. Participants were ob- tory, under the same conditions, and us-
Participants served for 30 minutes following vacci- ing the same assay as samples from ado-
Eligible participants were between 11 nation for immediate reactions; re- lescents and adults. Antitetanus titers
and 64 years of age, in good health, with ports of solicited local and systemic were calculated by comparison with an
a temperature of less than 38.0°C. Ex- reactions were collected for 14 days fol- international standard, Lot TE-3, avail-
clusion criteria included receipt of any lowing vaccination. Unsolicited ad- able from the World Health Organiza-
pertussis, diphtheria, or tetanus- verse event reports were collected for tion (WHO). Antidiphtheria antibody
containing vaccines within 5 years; di- 6 months. responses were measured by the ability
agnosis of pertussis within 2 years; al- of test sera to protect Vero cells from a
lergy or sensitivity to any vaccine Study Vaccines diphtheria toxin challenge. Results were
component, including previous vac- Tdap contained 2.5 µg of pertussis tox- reported by comparison with a cali-
cine reactions; acute respiratory ill- oid; 5 µg of filamentous hemaggluti- brated WHO reference serum and were
ness; daily use of oral nonsteroidal, anti- nin ; 3 µg of pertactin; 5 µg of fimbriae determined by the highest serum dilu-
inflammatory drugs; receipt of blood types 2 and 3; 2 Limit of flocculation tion that allowed cell metabolism in the
products or immunoglobulins within (Lf) of diphtheria toxoid; 5 Lf of teta- presence of the challenge dose of diph-
3 months; and any immunodefi- nus toxoid; 1.5 mg of aluminum phos- theria toxin.
3004 JAMA, June 22/29, 2005—Vol 293, No. 24 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
Safety and Reactogenicity cumference (at the midpoint between weakness, tiredness or decrease in en-
Outcome Measures shoulder and elbow of the injected ergy level, and sore or swollen joints
Immediate reaction data were re- limb) and systemic solicited reactions were recorded daily on a study-
corded in the clinic. Local solicited re- of fever (temperature ⱖ38°C), vomit- provided diary card for 14 days. Unso-
actions of erythema, swelling, pain, ing, headache, diarrhea, nausea, chills, licited adverse events were recorded for
axillary node swelling, and limb cir- rash, generalized body ache or muscle 14 days. Erythema, swelling, and fe-
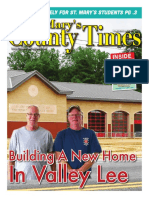
Figure 1. Flow of Patients Through the Trial
A Safety Population
Adolescents Adults
(Age 11-17 y) (Age 18-64 y)
2053 Randomized 2427 Randomized
1232 Assigned to Receive Tdap 821 Assigned to Receive Td 1821 Assigned to Receive Tdap 606 Assigned to Receive Td
1213 Received Vaccine as Assigned 815 Received Vaccine as Assigned 1804 Received Vaccine as Assigned 599 Received Vaccine as Assigned
7 Vaccine Unverifiable 3 Vaccine Unverifiable 14 Vaccine Unverifiable 6 Vaccine Unverifiable
12 Did Not Receive Vaccine 3 Did Not Receive Vaccine 3 Did Not Receive Vaccine 1 Did Not Receive Vaccine
29 Excluded (Site Excluded) 23 Excluded (Site Excluded) 52 Excluded (Site Excluded) 26 Excluded (Site Excluded)
2 Withdrew 1 Withdrew 1 Withdrew 0 Withdrew
0 Protocol Violation 0 Protocol Violation 1 Protocol Violation 1 Protocol Violation
16 Lost to Follow-up 12 Lost to Follow-up 80 Lost to Follow-up 23 Lost to Follow-up
1166 Completed 6-mo Safety Follow-up 779 Completed 6-mo Safety Follow-up 1670 Completed 6-mo Safety Follow-up 549 Completed 6-mo Safety Follow-up
1184 Included in Primary Safety Analysis 792 Included in Primary Safety Analysis 1752 Included in Primary Safety Analysis 573 Included in Primary Safety Analysis
29 Excluded From Primary Analysis 23 Excluded From Primary Analysis 52 Excluded From Primary Analysis 26 Excluded From Primary Analysis
(Site Excluded) (Site Excluded) (Site Excluded) (Site Excluded)
B Immunogenicity Population
Adolescents Adults
(Age 11-17 y) (Age 18-64 y)
2053 Randomized 2427 Randomized
606 of 1232 Assigned to Receive Tdap 608 of 821 Assigned to Receive Td 908 of 1821 Assigned to Receive Tdap 599 of 606 Assigned to Receive Td
Randomly Selected to Participate Randomly Selected to Participate Randomly Selected to Participate Randomly Selected to Participate
in Immunogenicity Study in Immunogenicity Study in Immunogenicity Study in Immunogenicity Study
602 Received Vaccine as Assigned 605 Received Vaccine as Assigned 901 Received Vaccine as Assigned 593 Received Vaccine as Assigned
3 Vaccine Unverifiable 3 Vaccine Unverifiable 7 Vaccine Unverifiable 6 Vaccine Unverifiable
1 Did Not Receive Vaccine 0 Did Not Receive Vaccine 0 Did Not Receive Vaccine 0 Did Not Receive Vaccine
17 Site Excluded 20 Site Excluded 29 Site Excluded 26 Site Excluded
58 Protocol Violations 69 Protocol Violations 129 Protocol Violations 57 Protocol Violations
39 Visit Out of Window 53 Visit Out of Window 105 Visit Out of Window 47 Visit Out of Window
15 Vaccination Error 12 Vaccination Error 7 Vaccination Error 3 Vaccination Error
3 Other Protocol Violations 2 Other Protocol Violations 17 Other Protocol Violations 7 Other Protocol Violations
1 Specimen Handling Error 2 Specimen Handling Error 0 Specimen Handling Error 0 Specimen Handling Error
585 Included in Primary Immunogenicity 585 Included in Primary Immunogenicity 872 Included in Primary Immunogenicity 567 Included in Primary Immunogenicity
Analysis Analysis Analysis Analysis
18 Excluded 20 Excluded 29 Excluded 26 Excluded
1 Not Vaccinated 0 Not Vaccinated 0 Not Vaccinated 0 Not Vaccinated
17 Site Excluded 20 Site Excluded 29 Site Excluded 26 Site Excluded
527 Included in Per Protocol 516 Included in Per Protocol 743 Included in Per Protocol 510 Included in Per Protocol
Immunogenicity Analysis Immunogenicity Analysis Immunogenicity Analysis Immunogenicity Analysis
76 Excluded 89 Excluded 158 Excluded 83 Excluded
18 Excluded From Primary Analysis 20 Excluded From Primary Analysis 29 Excluded From Primary Analysis 26 Excluded From Primary Analysis
58 Protocol Violations 69 Protocol Violations 129 Protocol Violations 57 Protocol Violations
A, Participant disposition and safety population. B, Participant disposition and immunogenicity population.
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, June 22/29, 2005—Vol 293, No. 24 3005
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
Statistical Analysis defined cut-off value and a 2-fold in-
Table 1. Demographic Characteristics
of the Safety Population* Planned enrollment was 4400 partici- crease if the prevaccination titer was
No. (%) pants, 1000 in each adolescent age stra- greater than the cut-off value. The cut-
tum (11-13, 14-17 years) and 800 in off prevaccination values were based on
Tdap Td each adult age stratum (18-28, 29-48, earlier clinical trial results: 2.56 IU/mL
Adolescents (n = 1184) (n = 792) and 49-64 years). The overall popula- for diphtheria, 2.7 IU/mL for tetanus, 85
Age, mean 13.8 (1.79) 13.8 (1.84)
(SD), y
tion for serum analysis was based on a EU/mL for pertussis toxoid, 170 EU/mL
11-13 599 (50.6) 405 (51.1)
sample size of 200 participants per stra- for filamentous hemagglutinin, 115
14-17 585 (49.4) 387 (48.9) tum for adults receiving Td and 300 per EU/mL for pertactin, and 285 EU/mL for
Sex stratum for adolescents in each treat- fimbriae types 2 and 3.
Female 598 (50.5) 392 (49.5) ment group and for adults receiving Baseline variables were compared be-
Male 586 (49.5) 400 (50.5) Tdap. Assuming 10% attrition, the tween groups using the analysis of vari-
Race/ethnicity† power to test each individual immu- ance technique for continuous vari-
White 1023 (86.4) 673 (85.0)
nogenicity hypothesis was at least ables and the 2 test or Fisher exact test
Black 111 (9.4) 73 (9.2)
80%. The sample size for safety had suf- for categorical variables.
Hispanic 15 (1.3) 24 (3.0)
ficient power to rule out 2-fold in- Percentages of participants with im-
Asian 16 (1.4) 8 (1.0)
creases of fever occurring at a rate of mediate, local, or systemic reactions and
Other 19 (1.6) 14 (1.8)
3% in the control group among 11- to those with adverse events or serious ad-
Adults (n = 1752) (n = 573)
17-year-olds. All sample size calcula- verse events were tabulated. For the
Age, mean 39.3 (13.65) 39.5 (13.32)
(SD), y tions were performed using nQuery ver- primary safety analysis of erythema,
18-28 587 (33.5) 189 (33.0) sion 3.0 (Statistical Solutions, Sagus, swelling, pain, and fever, Tdap was con-
29-48 584 (33.3) 189 (33.0) Mass) or in-house SAS version 8.2 (SAS sidered to be at least as safe as Td if the
49-64 581 (33.2) 195 (34.0) Institute Inc, Cary, NC). Statistical upper bound of the 95% CI of the be-
Sex analyses were performed by Red River tween-vaccine difference in event rates
Female 1136 (64.8) 353 (61.6) Statistics Inc of Shreveport, La, and in- was less than 10%. A post-hoc analy-
Male 616 (35.2) 220 (38.4) dependently by biostatistians at the Uni- sis for differences in subgroups of vac-
Race/ethnicity† versity of Rochester Medical Center, cinees by sex was performed, as were
White 1489 (85.0) 486 (84.8)
Rochester, NY. post-hoc analyses of rate ratios, with
Black 167 (9.5) 57 (9.9)
Hispanic 52 (3.0) 20 (3.5)
For tetanus and diphtheria, anti- 95% CIs, for erythema, swelling, pain,
Asian 25 (1.4) 6 (1.0)
body levels of at least 0.1 IU/mL are and fever.
Other 19 (1.1) 4 (0.7)
widely accepted as protective and are All participants randomized to pro-
Abbreviations: Td, tetanus-diphtheria vaccine; Tdap, tetanus-
thus a primary outcome measure.15,16 vide sera before and after vaccination
diphtheria 5-component acellular pertussis vaccine. Consistent with the US Food and Drug who met protocol criteria were in-
*Demographic parameters were similar in both vaccine
groups for the immunogenicity population. Administration (FDA) standards regard- cluded in the per-protocol immunoge-
†Self-reported. ing demonstration of noninferiority of nicity analysis. The planned modified
new combination products vs licensed intention-to-treat analysis for safety was
or individual products, Tdap was con- to include all participants who re-
ver were rated as mild, moderate, or se- sidered to be at least as immunogenic as ceived study vaccine, with a corrected
vere, based on size (0-9 mm, 10-34 mm, Td if the lower bound of a 95% confi- allocation for participants who re-
or ⱖ35 mm) or temperature (38.0°C- dence interval (CI) around the differ- ceived the wrong vaccine in error. Data
38.7°C, 38.8°C-39.4°C, or ⱖ39.5°C). ences in seroprotection rates in partici- for adolescents (aged 11-17 years) and
Pain was rated as mild to severe, based pants vaccinated with Tdap or Td was adults (aged 18-64 years) were evalu-
on the level of incapacitation experi- greater than –10%. For pertussis, Tdap ated separately. No values were im-
enced. After the initial 14-day period, would be considered at least as immu- puted to replace missing data; no ad-
any adverse event that required a medi- nogenic as DTaP if the lower bound of justments were made for multiplicity.
cal contact—including change of the 95% CI around the postvaccination For solicited events, denominators in-
medication, telephone call, office visit, geometric mean titer (GMT) ratio for clude participants for whom data were
emergency department visit, or hospi- Tdap and DTaP was greater than 0.67 available. For all analyses, nonoverlap-
talization—was recorded. Partici- (ie, =reciprocal of 1.5, a standard ap- ping 95% CIs were considered to be sta-
pants were contacted by telephone 6 proach required by FDA for demonstrat- tistically significant.
months after immunization to ensure ing noninferiority in vaccine trials). For
completeness of reporting. Serious ad- each antigen, booster response was a pri- RESULTS
verse events were recorded through- mary outcome measure, defined as a Between August 2001 and August
out the study and rated by investiga- 4-fold increase if the prevaccination ti- 2002, 4480 participants were random-
tors for relationship to study vaccine. ter was less than or equal to a pre- ized and underwent study procedures
3006 JAMA, June 22/29, 2005—Vol 293, No. 24 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
at 39 clinical centers across the United sera pairs were representative of all Safety and Reactogenicity
States. Of these participants, 2053 181 pairs tested in the original study, Safety and reactogenicity evaluation out-
were adolescents: 1213 received Tdap based on GMT ratios.4 comes were comparable between the
and 815 received Td. In the adult Tdap and Td groups for both the ado-
group, 2427 enrolled: 1804 received Immunogenicity lescent and adult populations. Sixteen
Tdap and 599 received Td (Figure 1). For tetanus and diphtheria, seropro- participants (11 adolescents and 5
Vaccination errors were reported for 5 tection rates of at least 0.1 IU/mL, adults) reported immediate reactions
participants (eg, randomized to Td but booster response rates, and 1-month within 30 minutes of vaccination. Pro-
vaccinated with Tdap); these partici- postimmunization GMTs were high and portions were similar among Tdap and
pants were reallocated to the group for similar between the Tdap and Td Td recipients: approximately 0.5% for
which they received vaccine. All data groups for both adolescents and adults. adolescents and 0.2% for adults. Most
from 1 site (130 participants total) Pertussis GMTs and proportions of par- immediate reactions were nervous sys-
were excluded from the primary safety ticipants with antibody levels consis- tem events, such as syncope, dizziness,
and immunogenicity analyses due to tent with boosting for each antigen or vasovagal reaction, or injection site
violations of Good Clinical Practices indicated robust responses to Tdap events, such as pain and erythema.
related to participants’ rights, vaccine (TABLE 2). The frequency and maximum inten-
administration and accountability, Pertussis antibody GMTs following sity of solicited local reactions of ery-
documentation, and study blinding 1 dose of Tdap were substantially higher thema and swelling were comparable
(Figure 1). The primary analysis of than those seen among infants follow- between the Tdap and Td groups for
data omits all data from this study site; ing 3 doses of DTaP for all pertussis an- both adolescents and adults (FIGURE 2).
for confirmatory purposes, an addi- tigens in both adults and adolescents In adolescents, pain occurred slightly
tional analysis was performed includ- (TABLE 3). In both age groups for diph- more frequently with Tdap vs Td. The
ing these data. Results were similar in theria and tetanus, the lower bounds of onset of solicited local adverse events
both analyses; accordingly, primary the CIs around the difference in rates was highest during days 0 through 3 in
analysis results are presented. Demo- between Tdap and Td were greater than both vaccine groups. Reported in-
graphic characteristics by age group –10%, and for pertussis the lower creases in limb circumference vs base-
are shown in TABLE 1. Data from 80 bounds of the CIs around the GMT ra- line were similar between the Tdap and
infants in a reference DTaP efficacy tios between Tdap and DTaP were Td groups, and most increases were 2
trial were included to evaluate pertus- above 0.67, meeting the noninferior- cm or less. Reported changes from base-
sis antibody responses; the 80 infant ity criteria. line included decreases in limb circum-
Table 2. Immunogenicity Findings in the Per-Protocol Population*
Adolescents 11-17 y Adults 18-64 y
Tdap Td Tdap Td
(n = 527) (n = 516) (n = 743) (n = 510)
Seroprotection ⱖ0.1 IU/mL, No./total (%)
Diphtheria 526/527 (99.8) 515/516 (99.8) 697/741 (94.1) 482/507 (95.1)
Tetanus 527/527 (100.0) 516/516 (100.0) 742/742 (100.0) 508/509 (99.8)
Booster response rates, No./total (%)†
Diphtheria 501/527 (95.1) 489/515 (95.0) 646/739 (87.4) 422/506 (83.4)
Tetanus 483/527 (91.7) 471/516 (91.3) 468/742 (63.1) 340/509 (66.8)
Pertussis toxin 482/524 (92.0) 624/739 (84.4)
Filamentous hemagglutinin 450/526 (85.6) 611/739 (82.7)
Pertactin 496/525 (94.5) 693/739 (93.8)
Fimbriae types 2 and 3 499/526 (94.9) 635/739 (85.9)
Geometric mean titers (95% CI)
Diphtheria, IU/mL 8.46 (7.56-9.48) 7.10 (6.43-7.83) 2.49 (2.17-2.85) 2.37 (2.05-2.73)
Tetanus, IU/mL 12.87 (12.28-13.48) 14.35 (13.64-15.09) 7.65 (7.28-8.04) 8.18 (7.64-8.75)
Pertussis toxin, EU/mL 309.26 (283.59-337.25) 15.61 (13.89-17.54) 178.84 (164.24-194.74) 13.16 (11.71-14.79)
Filamentous hemagglutinin, EU/mL 214.83 (200.34-230.37) 20.85 (18.63-23.34) 192.91 (180.72-205.93) 19.28 (17.26-21.54)
Pertactin, EU/mL 344.52 (313.28-378.87) 11.66 (10.33-13.16) 341.89 (306.19-381.75) 11.65 (10.28-13.21)
Fimbriae types 2 and 3, EU/mL 1792.40 (1603.74-2003.24) 28.84 (25.81-32.23) 852.72 (762.82-953.20) 31.68 (28.19-35.61)
Abbreviations: CI, confidence interval; ELISA, enzyme-linked immunosorbent assay; EU/mL, ELISA units per milliliter; Td, tetanus-diphtheria vaccine; Tdap, tetanus-diphtheria 5-com-
ponent acellular pertussis vaccine.
*For all comparisons, Tdap vaccine met predefined noninferiority criteria vs Td vaccine based on 95% CIs around the differences in seroprotection rates.
†Percentages based on participants for whom evaluable data were available. Up to 4 participants per group had missing data for an individual measurement.
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, June 22/29, 2005—Vol 293, No. 24 3007
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
ference in some participants. No cases with fever were within predefined events were uncommon for all solic-
of whole-arm swelling were reported in comparability bounds. The majority of ited systemic adverse events, occur-
either vaccine group. these fevers were mild, with only 2 of ring in 1.3% or less of all Tdap and Td
For adolescents and adults, the fre- 1170 adolescents in the Tdap group participants. Severe headache was
quency and maximum intensity of and 1 of 783 adolescents and 1 of 551 reported by 23 of 1175 and 12 of 787
each of the solicited systemic reactions adults in the Td group reporting adolescents and 47 of 1698 and 12 of
were comparable between the Tdap severe fever (temperature ⱖ39.5°C). 560 adult Tdap and Td participants for
and Td groups, based on noninferior- Most solicited systemic reactions whom severity was reported, respec-
ity testing (TABLE 4). For adolescents reported were mild. With the excep- tively, during postvaccination days 0
and adults, proportions of participants tion of headache, severe adverse through 14. A trend for higher per-
Table 3. Antibody Responses to Pertussis Antigens*
GMT (95% CI) Tdap/DTaP GMT Ratio
(95% CI)
Tdap: Adolescents Tdap: Adults DTaP: Infants 2-6 mo
Antigens, EU/mL (n = 527) (n = 741) (n = 80) Adolescents Adults
Pertussis toxin
Prevaccination 14.46 (12.95-16.14) 12.54 (11.46-13.73) 5.24 (4.23-6.48) 2.76 (2.06-3.70) 2.39 (1.80-3.18)
Postvaccination 309.26 (283.59-337.25) 178.84 (164.24-194.74) 86.55 (71.31-105.04) 3.57 (2.83-4.52) 2.07 (1.58-2.70)
Filamentous hemagglutinin
Prevaccination 19.49 (17.51-21.69) 18.13 (16.69-19.68) 5.21 (4.18-6.49) 3.74 (2.81-4.99) 3.48 (2.68-4.52)
Postvaccination 214.83 (200.34-230.37) 192.91 (180.72-205.93) 39.95 (34.62-46.10) 5.38 (4.46-6.49) 4.83 (3.94-5.92)
Pertactin
Prevaccination 10.01 (8.93-11.24) 8.45 (7.65-9.34) 2.15 (1.85-2.49) 4.67 (3.46-6.30) 3.94 (2.89-5.36)
Postvaccination 344.52 (313.28-378.87) 341.89 (306.19-381.75) 108.12 (91.41-127.88) 3.19 (2.48-4.10) 3.16 (2.25-4.44)
Fimbriae types 2 and 3
Prevaccination 25.80 (23.49-28.33) 28.56 (26.12-31.23) 13.26 (11.23-15.67) 1.94 (1.52-2.50) 2.15 (1.63-2.84)
Postvaccination 1792.40 (1603.74-2003.24) 852.72 (762.82-953.20) 341.10 (270.23-430.56) 5.25 (3.90-7.09) 2.50 (1.77-3.54)
Abbreviations: CI, confidence interval; ELISA, enzyme-linked immunosorbent assay; EU/mL, ELISA units per milliliter; GMT, geometric mean titer; Td, tetanus-diphtheria vaccine; Tdap,
tetanus-diphtheria 5-component acellular pertussis vaccine.
*Based on number of participants with evaluable data for each antigen. For all comparisons, Tdap vaccine met predefined noninferiority criteria.
Figure 2. Solicited Reactions of Erythema, Swelling, Pain, and Fever and Change in Limb Circumference Between Tdap and Td for Adolescents
and Adults
Change in Limb Circumference
>2.99 cm 1 to 1.99 cm
Severe Moderate Mild 2 to 2.99 cm >0 to <1 cm
A B
Adolescents Adults Adolescents Adults
80
% of Those Reporting Severity
70
60
50
40
30
20
10
0
Tdap Td Tdap Td Tdap Td Tdap Td Tdap Td Tdap Td Tdap Td Tdap Td Tdap Td Tdap Td
Erythema Swelling Pain Fever Erythema Swelling Pain Fever
No.
Tdap 1175 1175 1175 1170 1698 1698 1698 1688 1184 1752
Td 787 787 787 783 551 551 551 551 792 573
A, Solicited reactions of erythema, swelling, pain, and fever for adolescents and adults who provided severity measurements of mild to severe. For the percentages of
participants reporting these reactions, the upper limit of the 95% confidence interval around the difference between Tdap and Td was less than 10% for all age groups
and reactions, except pain in adolescents (10.72%). B, Increases in circumference of the limb injected with Tdap or Td, measured at the midpoint of the upper arm. No
differences between the 2 vaccine groups were observed for adolescents or adults.
3008 JAMA, June 22/29, 2005—Vol 293, No. 24 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
centages of females vs males with local cipients. Pertussis GMTs to pertussis vaccine in an efficacy trial that demon-
reactions was observed in the Tdap toxoid, filamentous hemagglutinin, strated 85% protection against classic
and Td groups, with greater differ- pertactin, and fimbriae types 2 and 3 pertussis and 78% protection against
ences in adults than in adolescents. after 1 dose of Tdap exceeded those milder pertussis (defined as culture-
No significant between-group differ- measured in a subset of infants who had proven pertussis with ⱖ1 day of
ences were observed for unsolicited ad- received 3 doses of the analogous DTaP cough).4 In comparisons between Tdap
verse events (Table 4).
Thirty women, 23 in the Tdap and Table 4. Reactions to Vaccination
7 in the Td group, became pregnant 1 No. (%)*
or more times during trial participa-
tion; each tested nongravid at study en- Adolescents Adults
try. Five miscarriages in the Tdap Tdap Td Tdap Td
group, 1 therapeutic abortion in the Td Reactions (n = 1175) (n = 787) (n = 1698) (n = 561)
group, and 4 early deliveries (2 in each Solicited Reactions
group) were reported. At birth, 23 new- Local reactions at days 0-3
postimmunization
borns, including the 4 early deliveries, Erythema 239 (20.34) 152 (19.31) 392 (23.09) 117 (20.86)
were reported to be normal. One Tdap Swelling 245 (20.85) 136 (17.28) 336 (19.79) 92 (16.40)
recipient experienced a miscarriage, re- Pain 912 (77.62) 555 (70.52) 1086 (63.96) 346 (61.68)
conceived, and subsequently deliv- Axillary node swelling 676 (5.70) 37 (4.70) 86 (5.06) 18 (3.21)
ered a healthy infant. Injection limb circumference 391 (33.27) 237 (30.11) 502 (29.56) 146 (26.02)
Sixty-three of 4301 (1.46%) partici- increase of ⱖ1 cm
pants reported 1 or more serious adverse Systemic reactions at days 0-3
postimmunization
events: 44 of 2936 (1.50%) in the Tdap Fever (temperature ⱖ38°C) 34 (2.91) 12 (1.53) 14 (0.83) 2 (0.36)
group and 19 of 1365 (1.39%) in the Td Vomiting 32 (2.72) 8 (1.02) 16 (0.94) 3 (0.54)
group. Only 2 serious adverse events, Headache 373 (31.74) 223 (28.34) 392 (23.09) 128 (22.86)
both in adult Tdap recipients, were con- Diarrhea 58 (4.94) 37 (4.70) 107 (6.31) 35 (6.25)
sidered possibly related to vaccine by the Nausea 91 (7.74) 47 (5.97) 89 (5.24) 22 (1.30)
investigator. A 23-year-old woman was Chills 125 (10.64) 65 (8.26) 93 (5.48) 18 (3.21)
hospitalized for a severe migraine with Rash 14 (1.19) 9 (1.14) 21 (1.24) 9 (1.61)
unilateral facial paralysis 1 day after vac- Generalized body ache/ 303 (25.79) 199 (25.29) 290 (17.09) 80 (14.29)
muscle weakness
cination, recovered without sequelae, and
Tiredness/decreased 287 (24.43) 180 (22.87) 316 (18.61) 86 (15.36)
was discharged 2 days later. A 49-year- energy level
old woman was hospitalized with a diag- Sore/swollen joints 113 (9.62) 73 (9.28) 118 (6.95) 32 (5.71)
nosis of nerve compression 12 days after
Unsolicited Adverse Events†
vaccination; the complaint resolved
Most common adverse events (n = 1184) (n = 792) (n = 1752) (n = 573)
within 1 day. Two cases of diabetes (1 (ⱖ1% in 1 or more groups)
in each vaccine group) and 2 cases of sei- at days 0-28 postimmunization
zures in adolescents with prior history Pharyngitis 40 (3.38) 27 (3.41) 34 (1.94) 7 (1.22)
of seizure disorder (1 in each vaccine Nasopharyngitis 36 (3.04) 34 (4.29) 33 (1.88) 11 (1.92)
group) were among the serious adverse Cough 25 (2.11) 20 (2.53) 17 (0.97) 6 (1.05)
events considered unrelated to study vac- Nasal congestion 24 (2.03) 7 (0.88) 6 (0.34) 2 (0.35)
cine by investigators. Upper respiratory tract 15 (1.27) 11 (1.39) 18 (1.03) 5 (0.87)
infection
Dizziness 14 (1.18) 7 (0.88) 5 (0.29) 1 (0.17)
COMMENT
Dysmenorrhea 14 (1.18) 9 (1.14) 19 (1.08) 6 (1.05)
In this study, the Tdap vaccine admin- Upper abdominal pain 12 (1.01) 2 (0.25) 0 (0.00) 0 (0.00)
istered was comparable with Td vac- Arthralgia 11 (0.93) 3 (0.38) 8 (0.46) 6 (1.05)
cine with respect to reactogenicity and Pain in limb 11 (0.93) 3 (0.38) 9 (0.51) 7 (1.22)
tetanus-diphtheria immunogenicity, Sinusitis 5 (0.42) 10 (1.26) 21 (1.20) 3 (0.52)
while providing robust pertussis anti- Limb injury 4 (0.34) 8 (1.01) 0 (0.00) 0 (0.00)
body responses in both adolescents and Abbreviations: Td, tetanus-diphtheria vaccine; Tdap, tetanus-diphtheria 5-component acellular pertussis vaccine.
adults. The percentages of partici- *Based on the number of participants for whom any diary card data was available; no data were imputed for missing
values. For formal comparisons, Tdap vaccine met predefined noninferiority criteria vs Td (the upper limit of the 95%
pants receiving Tdap and having sero- confidence interval [CI] around the between-group difference was less than 10%) for erythema, swelling, and fever.
For pain in adolescents, the upper limit was 10.72%. In the post-hoc rate ratio (RR) analysis of erythema, swelling,
protective antibody levels of at least 0.1 pain, and fever, statistical differences were noted only for pain (RR, 1.10; 95% CI, 1.04-1.16) and fever (RR, 1.85;
IU/mL to tetanus and diphtheria were 95% CI, 1.13-3.02) in adolescents.
†In the intent-to-treat population.
high and similar to those among Td re-
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, June 22/29, 2005—Vol 293, No. 24 3009
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
and Td for erythema, swelling, pain, and ferences in reactogenicity between fe- Study concept and design: Pichichero.
Acquisition of data: Pichichero, Rennels, Edwards,
fever, Tdap was comparable with Td, males and males were observed for both Blatter, Marshall, Bologa, Wang, Mills.
with the possible exception of pain in vaccines, consistent with observa- Analysis and interpretation of data: Pichichero, Rennels,
Edwards, Blatter, Bologa, Wang, Mills.
adolescents, for which the results were tions made with the use of other vac- Drafting of the manuscript: Pichichero, Blatter.
marginally outside of the predefined cines, such as influenza vaccine.20 Critical revision of the manuscript for important in-
tellectual content: Pichichero, Rennels, Edwards,
comparability bound. These results sup- Our study had certain limitations. Marshall, Bologa, Wang, Mills.
port the use of the Tdap vaccine in ado- There was insufficient power to detect Statistical analysis: Pichichero.
lescents and adults. uncommon adverse events. Also, the use Obtained funding: Pichichero.
Administrative, technical, or material support: Rennels,
The potential benefits of wide- of an infant comparison group to evalu- Edwards, Marshall, Bologa.
spread use of an adolescent and adult ate the immunogenicity of the pertussis Study supervision: Edwards, Blatter, Marshall, Bologa,
Wang, Mills.
pertussis booster vaccine include a re- component in adolescents and adults Financial Disclosures: Drs Pichichero and Edwards have
duction in pertussis disease. As the may raise some questions. However, no received grants from Aventis, GlaxoSmithKline, and
MedImmune. Dr Blatter is on the speakers’ bureau for
overall US case counts have grown, so definitive serological correlates of pro- Aventis. Dr Marshall has received research contracts,
too has the proportion of pertussis cases tection are available for pertussis, and the honoraria, and consultancies from Aventis.
in persons at least 10 years old, increas- efficacy of the infant formulation in pre- Funding/Support: Funding for the study was pro-
vided by Aventis Pasteur, now Sanofi Pasteur. Fund-
ing steadily from 15% in 1977-1979 to venting disease is well established. There- ing went to the academic institutions of the authors.
49% in 1997-2000.2 In 2003, the latest fore, this approach has been endorsed by Role of the Sponsor: The authors who are employees
of Aventis Pasteur participated in the design, supervi-
year for which complete data are avail- the FDA’s Vaccines and Related Biologi- sion, and conduct of the study; performed interpreta-
able, that proportion increased to 64%.1 cal Products Advisory Committee21 for tion of the data; and provided critical review of the manu-
script. The sponsor played a principal role in the design
Waning immunity to pertussis has been the purpose of licensing adolescent and and conduct of the study. A contract research organi-
demonstrated in adolescents and adults, adult acellular pertussis vaccine formu- zation, PPD Development, made site visits to ensure ac-
indicating increased susceptibility to lations that are based on infant vaccines curacy and integrity of the data and managed the study.
Independent Statistical Analysis: Jason Roy, PhD, and
disease in these age groups. Increased of demonstrated efficacy. Additional ex- Shirley Eberly, MS, of the Department of Biostatistics
incidence of disease in older patients is perience will be needed to further de- at the University of Rochester Medical Center, Roch-
ester, NY, performed a confirmatory statistical analy-
of public health significance because fine the profile of this vaccine in larger sis. Shayami Thanabalasundrum and James Trammel
they serve as the reservoir for Borde- populations. of Red River Statistics Inc, Shreveport, La, as well as Alek-
sandra Kolenc-Saban, MSc, and James Sloan of Aventis
tella pertussis infections in infants who Booster vaccination with tetanus and Pasteur performed data analyses and management.
are too young to have completed the diphtheria toxoids every 10 years has be- Aventis Pasteur contracted with Red River Statistics for
independent statistical review of the data. Red River
primary series of immunization. Per- come a standard of care in the United Statistics was not employed by Aventis Pasteur, nor were
tussis may be severe and even life- States. Our data indicate that the Tdap there any other arrangements with Aventis Pasteur other
threatening in very young infants.11,13,17 vaccine studied could be used to pro- than the contracted arrangement. Analysis of the data
was performed by the independent statistics company
Antimicrobial therapy, although effec- vide protection for tetanus and diph- and guided by the Food and Drug Administration for
tive in eradicating the organism from theria, as recommended, while provid- data requested in association with the Biologics Li-
cense Application (BLA) (presentations for the BLA oc-
the respiratory tract,18 does not alter the ing additional protection against curred on March 15, 2005).
progression of disease unless given pertussis. Evidence to support the in- Study Investigators: The following physicians en-
rolled participants into the trial and performed study
early, during the catarrhal phase when troduction of an acellular pertussis evaluations: Brian Allen, Onalaska, Wis; Wilson P. An-
pertussis is rarely suspected. There- booster in the United States includes a drews, Jr, Marietta, Ga; Gerald Bader, Vancouver,
fore, control of the disease must be recent Canadian National Advisory Wash; Ladan Bakhtari, Plano, Tex; David Bernstein,
Cincinnati, Ohio; Mark M. Blatter, Pittsburgh, Pa; Ken-
based on vaccination. Committee on Immunization state- neth Bromberg, Brooklyn, NY; Daniel Brune, Peoria,
Tolerability is an important consid- ment recommending that all preadoles- Ill; Timothy Craig, Hershey, Pa; Robert Daum, Chi-
cago, Ill; Cornelia Dekker, Stanford, Calif; Arnold del
eration in the development of new vac- cents and adolescents be vaccinated with Pilar, Jr, South Bend, Ind; Kathryn M. Edwards, Nash-
cines. Reactogenicity to pediatric for- an appropriately formulated acellular ville, Tenn; Bryan D. Evans, Huntsville, Ala; Stephen
M. Fries, Boulder, Colo; David P. Greenberg, Pitts-
mulation DTaP vaccines is associated pertussis vaccine.22 The introduction of burgh, Pa; Susan A. Keathley, Little Rock, Ark; Don-
with the amount of pertussis or diph- adolescent and adult Tdap booster im- ald J. Kennedy, St Louis, Mo; Erik Lamberth, Sellers-
ville, Pa; Thomas Latiolais, Bossier City, La; Joseph
theria toxoid per dose. Formulations munization in the United States could Leader, Woburn, Mass; Gary Marshall, Louisville, Ky;
with lower diphtheria and pertussis tox- enhance immunity against pertussis, Emma E. McCarty, Shreveport, La; Douglas K. Mitchell,
oid concentrations elicit less reactoge- which would be anticipated to de- Norfolk, Va; Laurie Peterson, Chippewa Falls, Wis; Mi-
chael Pichichero, Rochester, NY; Sharon E. Prohaska,
nicity.19 Therefore, the Tdap studied crease the incidence of pertussis in the Kansas City, Mo; Alfredo Quinonez, San Diego, Calif;
was formulated to contain lower quan- population, reduce the reservoir of per- Margaret B. Rennels, Baltimore, Md; David Paul Rob-
inson, Columbia, Mo; Kevin G. Rouse, Jonesboro, Ark;
tities of diphtheria and pertussis tox- tussis, and lessen transmission from ado- Joseph Saponaro, Jupiter, Fla; Shelly David Senders,
oids than the analogous US-licensed pe- lescents and adults to infants. University Heights, Ohio; Charles Sheaffer, Chapel Hill,
NC; Marc R. Shepard, Washington, DC; Peter E. Si-
diatric DTaP vaccine. Results of this las, Layton, Utah; Alex Spyropoulos, Albuquerque, NM;
study show a favorable reactogenicity Author Contributions: Dr Pichichero had full access Bradley Sullivan, Marshfield, Wis; Leonard B. Weiner,
to all of the data in the study and takes responsibility Syracuse, NY.
profile in adolescents and adults, suit- for the integrity of the data and the accuracy of the Acknowledgment: We thank William Bartlett, PhD,
able for routine use. Furthermore, dif- data analysis. and Linda Young, who performed serology analy-
3010 JAMA, June 22/29, 2005—Vol 293, No. 24 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
COMBINED TETANUS, DIPHTHERIA, PERTUSSIS VACCINE
ses; Kathy Heard and Jennifer Kasztejna, who per- pertussis among infants in the United States, land: World Health Organization; 1993. The Immu-
formed and oversaw trial monitoring; Robert 1980-1999. JAMA. 2003;290:2968-2975. nological Basis for Immunization Series. WHO/EPI
Daum, MD, David Johnson, MD, and Michael D. 7. Vitek CR, Pascual FB, Baughman AL, et al. In- /GEN/93.13.
Decker, MD, who provided scientific advice; and crease in deaths from pertussis among young infants 16. Galazka A. Module 2: Diphtheria. Geneva, Swit-
Lisa DeTora, PhD, and David Johnson, MD, who in the United States in the 1990s. Pediatr Infect Dis zerland: World Health Organization; 1993. The Immu-
are both full-time employees of Sanofi Pasteur in J. 2003;22:628-634. nological Basis for Immunization Series. WHO/EPI
Swiftwater, Pa, and who assisted in the editing of 8. Guris D, Strebel PM, Bardenheier B, et al. Chang- /GEN/93.13.
the manuscript. ing epidemiology of pertussis in the United States: in- 17. Cherry JD, Baraff LJ, Hewlett E. The past, pre-
Published Online: June 2, 2005 (doi:10.1001/ creasing reported incidence among adolescents sent, and future of pertussis: the role of adults in epi-
jama.293.24.3003). and adults, 1990-1996. Clin Infect Dis. 1999; demiology and future control. West J Med. 1989;150:
28:1230-1237. 319-328.
9. De Serres G, Shadmani R, Duval B, et al. Morbid- 18. Skowronski DM, De Serres G, MacDonald D, et al.
REFERENCES
ity of pertussis in adolescents and adults. J Infect Dis. The changing age and seasonal profile of pertussis in
1. Centers for Disease Control and Prevention. Sum- 2000;182:174-179. Canada. J Infect Dis. 2002;185:1448-1453.
mary of notifiable diseases, United States, 2003. 10. Yih K, Lett S, des Vignes F, et al. The increasing 19. Wharton M, Vitek C. Diphtheria toxoid. In: Plot-
MMWR Morb Mortal Wkly Rep. 2003;52:1-85. incidence of pertussis in Massachusetts adolescents kin S, Orenstein W, eds. Vaccines. 4th ed. Philadel-
2. Centers for Disease Control and Prevention. Per- and adults, 1989-1998. J Infect Dis. 2000;182:1409- phia, Pa: WB Saunders Co; 2004:211-228.
tussis-United States, 1997-2000. MMWR Morb Mor- 1416. 20. Beyer WE, Palache AM, Kerstens R, et al. Gender
tal Wkly Rep. 2002;51:73-76. 11. Deen JL, Mink CA, Cherry JD, et al. Household differences in local and systemic reactions to inacti-
3. Centers for Disease Control and Prevention. Notifi- contact study of Bordetella pertussis infections. Clin vated influenza vaccine, established by a meta-
able diseases/deaths in selected cities weekly information. Infect Dis. 1995;21:1211-1219. analysis of fourteen independent studies. Eur J Clin
MMWR Morb Mortal Wkly Rep. 2004;53:1213-1221. 12. von Konig CH, Halperin S, Riffelmann M, et al. Microbiol Infect Dis. 1996;15:65-70.
4. Gustafsson L, Hallander HO, Olin P, et al. A con- Pertussis of adults and infants. Lancet Infect Dis. 2002; 21. US Food and Drug Administration/Center for Bio-
trolled trial of a two-component acellular, a five- 2:744-750. logics Evaluation and Research. Vaccines and Related
component acellular, and a whole-cell pertussis vaccine. 13. Bisgard KM, Pascual FB, Ehresmann KR, et al. In- Biological Products Advisory Committee Meeting, June
N Engl J Med. 1996;334:349-355. fant pertussis: who was the source? Pediatr Infect Dis 5, 1997, Session 2. Available at: http://www.fda.gov
5. Greco D, Salmaso S, Mastrantonio P, et al; Pro- J. 2004;23:985-989. /ohrms/dockets/ac/97/transcpt/3300t1.pdf. Acces-
getto Pertosse Working Group. A controlled trial of 14. Gentili J, et al. The determination of potency of sibility verified May 31, 2005.
two acellular vaccines and one whole-cell vaccine human tetanus immunoglobulin. Biological 22. National Advisory Committee on Immunization
against pertussis. N Engl J Med. 1996;334:341-348. Standardization. 1984;12:167-173. (NACI). Pertussis vaccine. In: Canada Immunization
6. Tanaka M, Vitek CR, Pascual FB, et al. Trends in 15. Galazka A. Module 3: Tetanus. Geneva, Switzer- Guide. Ottawa, Ontario: NACI; 2002:169-176.
Author in the Room
Join the author of this article on Wednesday, July 20, 2005, from
2 to 3 PM Eastern time for “Author in the Room,” an interactive
conference call aimed at closing the gap between knowledge—
what is published in this article—and action—how much of this
knowledge can be put into your actual practice. This call, facili-
tated by clinical experts, should help readers answer their ques-
tions and consider the implications of the study results for their
practice. We will be studying the degree to which readers who
participate report implementing this change within their prac-
tice, and participants will be asked to complete 3 short surveys
(at registration, immediately after the call, and 3 months after the
call), which will assess clinical application.
Author in the Room is brought to you by JAMA and the Insti-
tute for Healthcare Improvement, with generous support from The
Robert Wood Johnson Foundation.
Please register early for this innovative initiative as there is no
fee for the first 200 callers. For more information or to register for
“Author in the Room,” please visit http://www.ihi.org/IHI/Programs
/ConferencesAndTraining/Author⫹in⫹the⫹Room.htm.
©2005 American Medical Association. All rights reserved. (Reprinted) JAMA, June 22/29, 2005—Vol 293, No. 24 3011
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
LETTERS
That approach leaves several critical issues unresolved.
First, federal policy actively discourages high-quality re-
CORRECTIONS
search by making access to marijuana by researchers ex- Author Contribution Omissions: In the Original Contribution entitled “High-
ceedingly difficult. Even when access to marijuana is fi- Dose Atorvastatin vs Usual-Dose Simvastatin for Secondary Prevention After Myo-
cardial Infarction: The IDEAL Study: A Randomized Controlled Trial” published in
nally granted, there is substantial variability in the purity the November 16, 2005, issue of JAMA (2005;294:2437-2445), several contri-
and content of the product. Second, researchers need to test butions were omitted for the author Anders G. Olsson, MD, PhD. In addition to
his contributions listed in the article, Dr Olsson contributed to the study concept
the assumption noted by Das that THC is the active ingre- and design, acquisition of data, drafting of the manuscript, and statistical analysis
dient responsible for the perceived beneficial effects. Al- for the IDEAL trial.
though that assumption is reasonable, there remains the pos- Duplicated Text: In the Original Contribution entitled “Neurologic Adverse Events
sibility that marijuana, not THC in isolation, achieves the Associated With Smallpox Vaccination in the United States, 2002-2004” pub-
desirable effects. Third, researchers should test the most ef- lished in the December 7, 2005, issue of JAMA (2005;294:2744-2750), a section
of text was duplicated. The first 4½ lines on the top of page 2747 should be de-
ficient delivery system. There may be some added value in leted. Thus, the last sentence on the bottom of page 2746 and continuing onto
smoking that needs to be evaluated. 2747 should read: “Of the remaining 3 cases, one man had probable encephalitis
defined by altered mental status, pleocytosis, and multifocal demyelinating le-
If research concludes that THC is the beneficial ingredi- sions on brain MRI 10 days after primary vaccination.”
ent and that delivery by tablet is safest and most effective,
Incorrect Wording and Data: In the Original Contribution entitled “Combined Teta-
then there is justification for approval of that method only. nus, Diphtheria, and 5-Component Pertussis Vaccine for Use in Adolescents and
A synthetic THC oral medication (dronabinol) is already Adults” published in the June 22/29, 2005, issue of JAMA (2005;293:3003-
3011), incorrect wording appeared at the end of the Results section. On page 3009,
available for prescription with US Food and Drug Admin- lines 15-16 of the fourth paragraph, “ . . . the complaint resolved within 1 day”
istration-approved indications for anorexia associated with should read “the patient was hospitalized for 1 day and the complaint subse-
weight loss in patients with AIDS and for nausea and vom- quently resolved without sequelae.” In addition, in Table 4, for the entry “Axillary
node swelling,” in column 2 (Tdap Adolescents) 676 should be 67.
iting associated with cancer chemotherapy in patients who
have failed to respond adequately to conventional anti- Incorrect Data: In the Original Contribution entitled “Adverse Events Reported Fol-
lowing Live, Cold-Adapted, Intranasal Influenza Vaccine,” published in the De-
emetic treatments. cember 7, 2005, issue of JAMA (2005;294:2720-2725), there were incorrect data
Regulation of the use of marijuana for medical purposes in the first full paragraph on page 2724. The corrected paragraph is reprinted
below:
is feasible and socially desirable, but it will require a differ-
ent way of thinking about the problem. It requires viewing Among 11 reports concerning individuals with a prior history of chronic cardio-
vascular disease, 1 serious case involved a 42-year-old man with a history of un-
marijuana as a potential medication subject to carefully con- controlled hyperlipidemia who was hospitalized with a myocardial infarction 2 days
trolled research, rather than as a drug of strict prohibition. after vaccination. He underwent cardiac catheterization. Among 10 reports from
individuals with preexisting metabolic conditions (including 8 with thyroid dis-
Lawrence O. Gostin, JD, LLD (Hon) ease), 1 (a 30-year-old man hospitalized with pneumonia 7 days after vaccina-
gostin@law.georgetown.edu tion) was serious. There were no other hospitalizations. Among the remaining 15
Georgetown Law Center individuals, 13 had chronic conditions (3 with chronic neurological conditions, 4
with chronic respiratory diseases, 2 with pernicious anemia, 2 with sarcoidosis, 1
Washington, DC with fibromyalgia, and 1 with lupus) and 2 were pregnant; none resulted in hos-
pitalization. One report, in a 48-year-old woman who had a prior history of Bell
Financial Disclosures: None reported. palsy, was classified as serious.
3092 JAMA, December 28, 2005—Vol 294, No. 24 (Reprinted) ©2005 American Medical Association. All rights reserved.
Downloaded From: http://jama.jamanetwork.com/ on 09/09/2013
Das könnte Ihnen auch gefallen
- Management of Infections in the Immunocompromised HostVon EverandManagement of Infections in the Immunocompromised HostBrahm H. SegalNoch keine Bewertungen
- Joc 50057Dokument10 SeitenJoc 50057Sudarman Abdul RahmanNoch keine Bewertungen
- Summaries of Evidence in Support of Proposed Recommendations FinalDokument25 SeitenSummaries of Evidence in Support of Proposed Recommendations FinalodyNoch keine Bewertungen
- Tdap Vaccine Effectiveness in Adolescents (Acosta 2017)Dokument11 SeitenTdap Vaccine Effectiveness in Adolescents (Acosta 2017)gd_hbarNoch keine Bewertungen
- Peds 2012-3836 FullDokument9 SeitenPeds 2012-3836 FullAnonymous hK8RDoNoch keine Bewertungen
- Nej Mo A 0807381Dokument12 SeitenNej Mo A 0807381Mildred MontNoch keine Bewertungen
- A Vaccine For MalariaDokument2 SeitenA Vaccine For MalariaArcciPradessatamaNoch keine Bewertungen
- 1 s2.0 S1875957210000185 Main PDFDokument4 Seiten1 s2.0 S1875957210000185 Main PDFirs2407Noch keine Bewertungen
- New England Journal Medicine: The ofDokument10 SeitenNew England Journal Medicine: The ofAlmuizzu NurjannahNoch keine Bewertungen
- Fneur 04 00142Dokument7 SeitenFneur 04 00142nyuwwchocolavaNoch keine Bewertungen
- Pediatrics 2014 Vogt 721 8Dokument10 SeitenPediatrics 2014 Vogt 721 8NurulSoraiyaNoch keine Bewertungen
- Mechanisms and Regulation of The Gene-Expression Response To SepsisDokument11 SeitenMechanisms and Regulation of The Gene-Expression Response To SepsisNagy MonikaNoch keine Bewertungen
- Seguridad Vacunal: Precauciones y Contraindicaciones de Las Vacunas. Reacciones Adversas. FarmacovigilanciaDokument25 SeitenSeguridad Vacunal: Precauciones y Contraindicaciones de Las Vacunas. Reacciones Adversas. FarmacovigilanciaMaribel Catalan HabasNoch keine Bewertungen
- Infancy Interchangeability of 2 Diphtheria-Tetanus-Acellular Pertussis Vaccines inDokument9 SeitenInfancy Interchangeability of 2 Diphtheria-Tetanus-Acellular Pertussis Vaccines inMargaretha MonikaNoch keine Bewertungen
- Safety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesDokument9 SeitenSafety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesHansley Templeton CookNoch keine Bewertungen
- Safety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesDokument11 SeitenSafety Surveillance of Diphtheria and Tetanus Toxoids and Acellular Pertussis (Dtap) VaccinesElva PatabangNoch keine Bewertungen
- Journal Gerontik 1Dokument11 SeitenJournal Gerontik 1AgUnk MancuNianNoch keine Bewertungen
- Clinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiaDokument6 SeitenClinico-Epidemiological Profile and Predictors of Outcome in Children With Diphtheria: A Study From Northern IndiamariaprincesitaNoch keine Bewertungen
- Robust Humoral and Cellular Immune Responses To PeDokument11 SeitenRobust Humoral and Cellular Immune Responses To PeHtp BkkNoch keine Bewertungen
- Antigen-Specific Proliferation and Interferon-γ and Interleukin-5 Production Are Down-Regulated during Schistosoma haematobium Infection PDFDokument5 SeitenAntigen-Specific Proliferation and Interferon-γ and Interleukin-5 Production Are Down-Regulated during Schistosoma haematobium Infection PDFGabriel CoutoNoch keine Bewertungen
- A Two-Phased Population Epidemiological Study of The Safety of Thimerosal-Containing Vaccines: A Follow-Up AnalysisDokument11 SeitenA Two-Phased Population Epidemiological Study of The Safety of Thimerosal-Containing Vaccines: A Follow-Up AnalysisRodrigo YepsenNoch keine Bewertungen
- CefepimeDokument5 SeitenCefepimeMich KingsNoch keine Bewertungen
- Immune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsDokument10 SeitenImmune Responses To Measles and Mumps Vaccination of Infants at 6, 9, and 12 MonthsManiru Aliyu GiganeNoch keine Bewertungen
- Poi 130021Dokument5 SeitenPoi 130021Olivia DwimaswastiNoch keine Bewertungen
- Vol. 69, No. 02, February 2019Dokument4 SeitenVol. 69, No. 02, February 2019Rahma ArsytaNoch keine Bewertungen
- Impact of Tetanus ToxoidDokument6 SeitenImpact of Tetanus Toxoidanes noerNoch keine Bewertungen
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDokument11 SeitenAcellular Pertussis Vaccine Effectiveness Over Time: Objectives[JC]Noch keine Bewertungen
- Ipt 1Dokument7 SeitenIpt 1PPDS ANAK FK USUNoch keine Bewertungen
- PertussisDokument8 SeitenPertussisomjoshNoch keine Bewertungen
- Acellular Pertussis Vaccine Effectiveness Over Time: ObjectivesDokument11 SeitenAcellular Pertussis Vaccine Effectiveness Over Time: ObjectivesLee제노Noch keine Bewertungen
- Asmainf AmamDokument10 SeitenAsmainf AmamgabibarbozaNoch keine Bewertungen
- Genetics and The Evaluation of The Febrile Child: EditorialDokument2 SeitenGenetics and The Evaluation of The Febrile Child: EditorialYRRVNoch keine Bewertungen
- THT - 12 Acute Otitis Media and Other Complication of Viral Respiratory InfectionDokument12 SeitenTHT - 12 Acute Otitis Media and Other Complication of Viral Respiratory InfectionWelly SuryaNoch keine Bewertungen
- Ham Mitt 2019Dokument11 SeitenHam Mitt 2019heryanggunNoch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument17 SeitenNIH Public Access: Author ManuscriptJoyBoyXNoch keine Bewertungen
- Judicious Use of Antibiotics: A Guide For Oregon CliniciansDokument32 SeitenJudicious Use of Antibiotics: A Guide For Oregon CliniciansRiyan SaputraNoch keine Bewertungen
- Typhoid BangladeshDokument11 SeitenTyphoid BangladeshMarindaRamadhanyNoch keine Bewertungen
- Nejm VaricellaDokument9 SeitenNejm VaricellaadityailhamNoch keine Bewertungen
- Review ArticleDokument8 SeitenReview ArticleIdmNoch keine Bewertungen
- Investigation of Tetanus Antibody Levels in Adults: Erişkinlerde Tetanoz Antikor Düzeylerinin AraştırılmasıDokument7 SeitenInvestigation of Tetanus Antibody Levels in Adults: Erişkinlerde Tetanoz Antikor Düzeylerinin Araştırılmasısyafiq ishakNoch keine Bewertungen
- MMR VaccineDokument3 SeitenMMR VaccineDaniel Ninety-Nine Percent BrumbaughNoch keine Bewertungen
- High Virological Failure Rates in HIV1 Perinatally Infected Children in South Africa A Retrospective Cohort StudySouth African Medical JournalDokument5 SeitenHigh Virological Failure Rates in HIV1 Perinatally Infected Children in South Africa A Retrospective Cohort StudySouth African Medical JournalFarrell AnggoroNoch keine Bewertungen
- An Observational Study of Febrile Seizures: The Importance of Viral Infection and ImmunizationDokument6 SeitenAn Observational Study of Febrile Seizures: The Importance of Viral Infection and Immunizationnavali rahmaNoch keine Bewertungen
- JURNAL READINGnejmoa1007174Dokument11 SeitenJURNAL READINGnejmoa1007174Sukma WinahyuNoch keine Bewertungen
- Immunogenicity of Fractional-Dose Vaccine During A Yellow Fever Outbreak - Preliminary ReportDokument9 SeitenImmunogenicity of Fractional-Dose Vaccine During A Yellow Fever Outbreak - Preliminary Reportrizki agusmaiNoch keine Bewertungen
- Comment: Pallidum-The Syphilis AgentDokument2 SeitenComment: Pallidum-The Syphilis AgentM AlbertNoch keine Bewertungen
- Sitasi Jurnal 4Dokument8 SeitenSitasi Jurnal 4ninikNoch keine Bewertungen
- Literature Review On Dengue VirusDokument7 SeitenLiterature Review On Dengue Virusaflskeqjr100% (1)
- With Pneumonia Narrow Vs Broad-Spectrum Antimicrobial Therapy For Children HospitalizedDokument10 SeitenWith Pneumonia Narrow Vs Broad-Spectrum Antimicrobial Therapy For Children HospitalizedanettepardedeNoch keine Bewertungen
- PIIS0091674900700467Dokument6 SeitenPIIS0091674900700467Ayu DewiNoch keine Bewertungen
- Malaria ResearchDokument10 SeitenMalaria ResearchYosfikriansyahYosfiqarNoch keine Bewertungen
- Research Paper On Childhood VaccinationsDokument8 SeitenResearch Paper On Childhood Vaccinationsefjr9yx3100% (1)
- Articles: BackgroundDokument11 SeitenArticles: BackgroundRicho WijayaNoch keine Bewertungen
- Capstone 2Dokument11 SeitenCapstone 2mauriciosagredoNoch keine Bewertungen
- Impact of Glutathione S-Transferase M1 and T1 On Anti-Tuberculosis Drug-Induced Hepatotoxicity in Chinese Pediatric PatientsDokument11 SeitenImpact of Glutathione S-Transferase M1 and T1 On Anti-Tuberculosis Drug-Induced Hepatotoxicity in Chinese Pediatric PatientsLuis JaramilloNoch keine Bewertungen
- Response To Measles-Mumps-Rubella Vaccine in Children With Autism Spectrum DisordersDokument6 SeitenResponse To Measles-Mumps-Rubella Vaccine in Children With Autism Spectrum DisorderspriciliaNoch keine Bewertungen
- DermatomiositisDokument7 SeitenDermatomiositisCarlos CalvoNoch keine Bewertungen
- Risk Factors For and Outcomes of Multidrug-Resistant Escherichia Coli Infections in ChildrenDokument17 SeitenRisk Factors For and Outcomes of Multidrug-Resistant Escherichia Coli Infections in ChildrenLihaniUltifaNoch keine Bewertungen
- Jurnal 1Dokument6 SeitenJurnal 1Rey M FakhruryNoch keine Bewertungen
- Comparison of A Whole-Blood Interferon Assay With Tuberculin Skin Testing For Detecting LatentDokument8 SeitenComparison of A Whole-Blood Interferon Assay With Tuberculin Skin Testing For Detecting Latentfduran2015Noch keine Bewertungen
- Total and Acute Uterine Inversion After Delivery A Case Report PDFDokument4 SeitenTotal and Acute Uterine Inversion After Delivery A Case Report PDFatika sgrtNoch keine Bewertungen
- Metabolic Precursors of SurfactantDokument8 SeitenMetabolic Precursors of Surfactantatika sgrtNoch keine Bewertungen
- Cervical Insufficiency A New Issue For Guidelines On Prevention of Perinatal Group B Streptococcal DiseaseDokument6 SeitenCervical Insufficiency A New Issue For Guidelines On Prevention of Perinatal Group B Streptococcal Diseaseatika sgrtNoch keine Bewertungen
- PLACENTAL LESIONS ASSOCIATED WITH MATERNAL Underperfusion Are More Frequent in Early Onset Pre EclampsiaDokument22 SeitenPLACENTAL LESIONS ASSOCIATED WITH MATERNAL Underperfusion Are More Frequent in Early Onset Pre Eclampsiaatika sgrtNoch keine Bewertungen
- Preeclampsia and The Risk of Bronchopulmonary Dysplasia in VLBW Infants A Population Based StudyDokument7 SeitenPreeclampsia and The Risk of Bronchopulmonary Dysplasia in VLBW Infants A Population Based Studyatika sgrtNoch keine Bewertungen
- Clinical Risk Index For Babies (CRIB II)Dokument4 SeitenClinical Risk Index For Babies (CRIB II)atika sgrtNoch keine Bewertungen
- MPV Congress Schedule - Time SpeakersDokument4 SeitenMPV Congress Schedule - Time SpeakersMary AntNoch keine Bewertungen
- Past Quiz QuestionsDokument4 SeitenPast Quiz QuestionsAbubakar AbdhooNoch keine Bewertungen
- SMU Prospectus 2024 2025Dokument76 SeitenSMU Prospectus 2024 2025g8fh9dkcmgNoch keine Bewertungen
- Your Health Is Mostly ImportantDokument2 SeitenYour Health Is Mostly ImportantNolie De Lara CastilloNoch keine Bewertungen
- Fifth Edition Answers To End-Of-Chapter Questions: GCSE Biology For YouDokument2 SeitenFifth Edition Answers To End-Of-Chapter Questions: GCSE Biology For YouRafia ArmanNoch keine Bewertungen
- Table I IAP Immunization Schedule 2016 FinalDokument7 SeitenTable I IAP Immunization Schedule 2016 FinalVaishnavi AgrawalNoch keine Bewertungen
- Health Effects in Vaccinated Versus Unvaccinated ChildrenDokument11 SeitenHealth Effects in Vaccinated Versus Unvaccinated ChildrenMahesh JayaramanNoch keine Bewertungen
- 2009 Hy-Line Brown GuiaDokument41 Seiten2009 Hy-Line Brown GuiaJorge AymeNoch keine Bewertungen
- DR Vernon Coleman Covid 19 Vaccine - Possible Vaccine Side EffectsDokument2 SeitenDR Vernon Coleman Covid 19 Vaccine - Possible Vaccine Side EffectsGeorge KourisNoch keine Bewertungen
- Ilovepdf Merged 2 PDFDokument307 SeitenIlovepdf Merged 2 PDFAhmed ZidanNoch keine Bewertungen
- NP2 1 1Dokument12 SeitenNP2 1 1Lyca Berin100% (1)
- Soal TPS Bahasa InggrisDokument3 SeitenSoal TPS Bahasa InggrisMaya Putri EkasariNoch keine Bewertungen
- Vaccination: A Mythical HistoryDokument9 SeitenVaccination: A Mythical HistoryDisicienciaNoch keine Bewertungen
- The Role of Nanotechnology in The Treatment of Viral InfectionsDokument27 SeitenThe Role of Nanotechnology in The Treatment of Viral InfectionsDr. Shrikant BarkadeNoch keine Bewertungen
- ErysipelothrixDokument4 SeitenErysipelothrixFanny CanoNoch keine Bewertungen
- Vacuna Neumócoco 15 ValenteDokument8 SeitenVacuna Neumócoco 15 ValenteRoberto MorenoNoch keine Bewertungen
- Reviews: Viral Hepatitis and PregnancyDokument15 SeitenReviews: Viral Hepatitis and PregnancyRANINoch keine Bewertungen
- Toronto Notes 2012-Paeds PDFDokument99 SeitenToronto Notes 2012-Paeds PDFvrsiewNoch keine Bewertungen
- Edgcse TTPP cb5 SB AnswersDokument5 SeitenEdgcse TTPP cb5 SB AnswersRaijin Kaze0% (1)
- Dental Infection Control GuidelinesDokument77 SeitenDental Infection Control GuidelinesMohamed KhaledNoch keine Bewertungen
- NSTP 111 Maintaining Health Care at Home & in The CommunityDokument3 SeitenNSTP 111 Maintaining Health Care at Home & in The CommunityAthena Irish LastimosaNoch keine Bewertungen
- VDCA Guideline SrilankaDokument31 SeitenVDCA Guideline SrilankaVinay PathakNoch keine Bewertungen
- Male Qbank PDFDokument126 SeitenMale Qbank PDFgabby_54everNoch keine Bewertungen
- Hostel Prospectus BookletDokument12 SeitenHostel Prospectus BookletsansharmajsNoch keine Bewertungen
- DNA Vaccines Prim Time Is NowDokument7 SeitenDNA Vaccines Prim Time Is NowalferezhassanNoch keine Bewertungen
- Swarnaprashana PDFDokument9 SeitenSwarnaprashana PDFAnuroop MondruNoch keine Bewertungen
- CBSE NCERT Solutions For Class 9 Science Chapter 13: Back of Chapter QuestionsDokument6 SeitenCBSE NCERT Solutions For Class 9 Science Chapter 13: Back of Chapter QuestionsNarayanamurthy AmirapuNoch keine Bewertungen
- Brand Name: Berirab Contents: Indication / Action:: RabiesDokument4 SeitenBrand Name: Berirab Contents: Indication / Action:: RabiesAbdelmar SusulanNoch keine Bewertungen
- 2021-08-05 St. Mary's County TimesDokument32 Seiten2021-08-05 St. Mary's County TimesSouthern Maryland OnlineNoch keine Bewertungen
- 2009-09-17Dokument40 Seiten2009-09-17Southern Maryland OnlineNoch keine Bewertungen