Das könnte Ihnen auch gefallen
- 5 ASEMI Z 2013 The - Effect - of - DASH - Diet - On - PreDokument7 Seiten5 ASEMI Z 2013 The - Effect - of - DASH - Diet - On - Preiriartenela14Noch keine Bewertungen
- Zaharah KurniawatiDokument6 SeitenZaharah KurniawatiIhdina Hanifa Hasanal IbrahimNoch keine Bewertungen
- DIPSI GuidelinesDokument7 SeitenDIPSI GuidelinesvinaypharmNoch keine Bewertungen
- Assignment On Course During CCGDM.Dokument6 SeitenAssignment On Course During CCGDM.Biman MondalNoch keine Bewertungen
- Gestational Diabetes Mellitus Management Through ADokument15 SeitenGestational Diabetes Mellitus Management Through AdoctorshereNoch keine Bewertungen
- Single-Step DIPSI 75g Glucose Tolerance Test-For Diagnosis of Gestational Diabetes MellitusDokument7 SeitenSingle-Step DIPSI 75g Glucose Tolerance Test-For Diagnosis of Gestational Diabetes MellitusEditor ERWEJNoch keine Bewertungen
- Jurnal DMDokument8 SeitenJurnal DMNana MuktiNoch keine Bewertungen
- Diabetes in Pregnancy: Early Diagnosis and Comphrehensive ManagementDokument32 SeitenDiabetes in Pregnancy: Early Diagnosis and Comphrehensive ManagementayuNoch keine Bewertungen
- Diabetes Dalam KehamilanDokument26 SeitenDiabetes Dalam KehamilanamriNoch keine Bewertungen
- Pregnancy OutcomesDokument6 SeitenPregnancy Outcomesconstantius augustoNoch keine Bewertungen
- 47 Manuscript 226 5 10 20210811Dokument6 Seiten47 Manuscript 226 5 10 20210811Dikri NurfazrinNoch keine Bewertungen
- Gestational Diabetes 1Dokument12 SeitenGestational Diabetes 1Kyla Isobel DalonosNoch keine Bewertungen
- Oral Antidiabetic Drugs in Pregnancy: The Other AlternativeDokument5 SeitenOral Antidiabetic Drugs in Pregnancy: The Other AlternativeBelinda Indha KolelupunNoch keine Bewertungen
- Huiyan WangDokument8 SeitenHuiyan Wangconstantius augustoNoch keine Bewertungen
- 533 Afiska Prima Dewi G2C009078Dokument28 Seiten533 Afiska Prima Dewi G2C009078Dhanang Prawira NugrahaNoch keine Bewertungen
- Gestational Diabetes Mellitus - Glycemic Control and Maternal Prognosis - UpToDateDokument46 SeitenGestational Diabetes Mellitus - Glycemic Control and Maternal Prognosis - UpToDateBruno FernandesNoch keine Bewertungen
- Research Article Achievement of Target Glycemic Goal With Simple Basal Insulin Regimen in Women With Gestational Diabetes: A Prospective Cohort StudyDokument9 SeitenResearch Article Achievement of Target Glycemic Goal With Simple Basal Insulin Regimen in Women With Gestational Diabetes: A Prospective Cohort Studyzuliarni lubisNoch keine Bewertungen
- 17 ShaofangDokument4 Seiten17 Shaofangiriartenela14Noch keine Bewertungen
- Newer Insulin in Diabetic Pregnancy - PPT'Dokument56 SeitenNewer Insulin in Diabetic Pregnancy - PPT'Hemamalini100% (1)
- Nfs 774 Case StudyDokument37 SeitenNfs 774 Case Studyapi-533845626Noch keine Bewertungen
- Obstetric Research Journal DayandanteDokument4 SeitenObstetric Research Journal DayandanteKrizelle MesinaNoch keine Bewertungen
- Weight Management Clinical TrialsDokument7 SeitenWeight Management Clinical TrialschuariwapoohNoch keine Bewertungen
- Annotated BibliographyDokument20 SeitenAnnotated Bibliographyapi-347153077Noch keine Bewertungen
- Treatments For Women With Gestational DiabetesDokument3 SeitenTreatments For Women With Gestational DiabetesVincenzina SoósNoch keine Bewertungen
- Gestational Diabetes Education and Diabetes Prevention StrategiesDokument5 SeitenGestational Diabetes Education and Diabetes Prevention StrategiesEsha KuttiNoch keine Bewertungen
- High Maternal Hba Is Associated With Overweight In Neonates: Dan Med Bul Ϧϫ/ϪDokument6 SeitenHigh Maternal Hba Is Associated With Overweight In Neonates: Dan Med Bul Ϧϫ/ϪHerry SasukeNoch keine Bewertungen
- Carol An 2013Dokument9 SeitenCarol An 2013Wismoyo Nugraha PutraNoch keine Bewertungen
- Jurnal 1Dokument14 SeitenJurnal 1Craig LewisNoch keine Bewertungen
- 11 ORATILE. P. ROBERTO OLMOSTrat. Con Dieta y EjercicoDokument8 Seiten11 ORATILE. P. ROBERTO OLMOSTrat. Con Dieta y Ejercicoiriartenela14Noch keine Bewertungen
- I J R P S: Metformin Compared To Insulin For The Management of Gestational DiabeticDokument5 SeitenI J R P S: Metformin Compared To Insulin For The Management of Gestational DiabeticAbed AlhaleemNoch keine Bewertungen
- Who PDFDokument23 SeitenWho PDFMayra PereiraNoch keine Bewertungen
- Efficacy of Value Added Foxtail Millet Therapeutic Food in The Management of Diabetes and Dyslipidamea in Type 2 Diabetic PatientsDokument3 SeitenEfficacy of Value Added Foxtail Millet Therapeutic Food in The Management of Diabetes and Dyslipidamea in Type 2 Diabetic PatientsFauziah AmrullahNoch keine Bewertungen
- sullivan1998 ເອກະສານອ້າງອີງ ຈາກ ວິທີວິທະຍາDokument10 Seitensullivan1998 ເອກະສານອ້າງອີງ ຈາກ ວິທີວິທະຍາKab Zuag HaamNoch keine Bewertungen
- DafneDokument6 SeitenDafnePatricia PalenqueNoch keine Bewertungen
- Clinical StudyDokument8 SeitenClinical StudyanitaNoch keine Bewertungen
- Guideline No. 393-Diabetes in Pregnancy: Sogc Clinical Practice GuidelineDokument13 SeitenGuideline No. 393-Diabetes in Pregnancy: Sogc Clinical Practice GuidelineAmel ZaoumaNoch keine Bewertungen
- Metformin Vs Insulin in Gestational DiabetesDokument17 SeitenMetformin Vs Insulin in Gestational Diabetesmiguel alejandro zapata olayaNoch keine Bewertungen
- GDM FOGSI Text Book FinalDokument29 SeitenGDM FOGSI Text Book FinalKruthika Devaraja GowdaNoch keine Bewertungen
- Journal GAJOMSDokument6 SeitenJournal GAJOMSmade dharmaNoch keine Bewertungen
- 2023 OGClinNA Medications For Managing Preexisting and Gestational Diabetes in PregnancyDokument16 Seiten2023 OGClinNA Medications For Managing Preexisting and Gestational Diabetes in PregnancynataliaNoch keine Bewertungen
- Literature Review of Gestational Diabetes MellitusDokument7 SeitenLiterature Review of Gestational Diabetes Mellitusc5rc7ppr100% (1)
- JCEM Diabetes in Pregnancy 2013Dokument23 SeitenJCEM Diabetes in Pregnancy 2013Ann DahngNoch keine Bewertungen
- Glycemic Variability and Hypoglycemia Before and ADokument7 SeitenGlycemic Variability and Hypoglycemia Before and ALeonorNoch keine Bewertungen
- Home-Based Exercise Training Improves Capillary Glucose Profile in Women With Gestational DiabetesDokument4 SeitenHome-Based Exercise Training Improves Capillary Glucose Profile in Women With Gestational DiabetesdiahadnyaNoch keine Bewertungen
- Emphasis of Yoga in The Management of Diabetes 2155 6156 1000613Dokument11 SeitenEmphasis of Yoga in The Management of Diabetes 2155 6156 1000613AnuradhatagoreNoch keine Bewertungen
- Case Study of Gestational Diabetes Mellitus Group 2Dokument19 SeitenCase Study of Gestational Diabetes Mellitus Group 2nicoleNoch keine Bewertungen
- The Relationship of Diabetes Mellitus Diet Knowledge With Blood Glucose Levels in Patients Diabetes Mellitus Type Ii in Hermana Hospital LembeanDokument5 SeitenThe Relationship of Diabetes Mellitus Diet Knowledge With Blood Glucose Levels in Patients Diabetes Mellitus Type Ii in Hermana Hospital LembeanIrene Hana HutagalungNoch keine Bewertungen
- Ramachandran 2006Dokument9 SeitenRamachandran 2006Dharsheena Seshadri ManogaranNoch keine Bewertungen
- Gestational Diabetes Mellitus (GDM)Dokument33 SeitenGestational Diabetes Mellitus (GDM)Sri WahyuniNoch keine Bewertungen
- DiabetesDokument34 SeitenDiabetesAdrián MartínezNoch keine Bewertungen
- To Study Effect of Medical Nutrition Therapy in Patients of Gestational Diabetes MellitusDokument4 SeitenTo Study Effect of Medical Nutrition Therapy in Patients of Gestational Diabetes MellitusIJAR JOURNALNoch keine Bewertungen
- Early Postpartum Metabolic Syndrome in Women With or Without 2017Dokument7 SeitenEarly Postpartum Metabolic Syndrome in Women With or Without 2017Lucas LorranNoch keine Bewertungen
- Gestational Diabetes Mellitus (GDM) .TriceDokument47 SeitenGestational Diabetes Mellitus (GDM) .TricejerrydanfordfxNoch keine Bewertungen
- Diabetes DietDokument8 SeitenDiabetes DietkitchaaNoch keine Bewertungen
- Clinical Nutrition: Original ArticleDokument6 SeitenClinical Nutrition: Original ArticleMed AjNoch keine Bewertungen
- Current Therapeutic ResearchDokument5 SeitenCurrent Therapeutic Researchmnn164Noch keine Bewertungen
- Obesitas Sentral Berhubungan Dengan Toleransi Glukosa Terganggu Pada Remaja PerempuanDokument6 SeitenObesitas Sentral Berhubungan Dengan Toleransi Glukosa Terganggu Pada Remaja PerempuanSelvira MarthingNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsVon EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNoch keine Bewertungen
- Complementary and Alternative Medical Lab Testing Part 18: PsychiatryVon EverandComplementary and Alternative Medical Lab Testing Part 18: PsychiatryBewertung: 5 von 5 Sternen5/5 (1)
- Quantities Survey MethodsDokument73 SeitenQuantities Survey MethodsparvezNoch keine Bewertungen
- Sample Papers ScienceDokument199 SeitenSample Papers SciencerkkanodiaNoch keine Bewertungen
- D4304-Syllabus-Neural Networks and Fuzzy SystemsDokument1 SeiteD4304-Syllabus-Neural Networks and Fuzzy Systemsshankar15050% (1)
- 1922 A Textbook of Balochi LanguageDokument228 Seiten1922 A Textbook of Balochi LanguageAnonymous 0ywnNS29EGNoch keine Bewertungen
- Partea I .60p I. Read The Text Below and Complete The Following Tasks. Write All Your Answers On The Answer SheetDokument4 SeitenPartea I .60p I. Read The Text Below and Complete The Following Tasks. Write All Your Answers On The Answer SheetaaddniaNoch keine Bewertungen
- An FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure CommunicationsDokument5 SeitenAn FPGA Implementation of A Feed-Back Chaotic Synchronization For Secure Communicationslaz_chikhi1574Noch keine Bewertungen
- Best Approach: Compound AngleDokument8 SeitenBest Approach: Compound AngleAbhiyanshu KumarNoch keine Bewertungen
- Coding Assignment 18-WPS OfficeDokument9 SeitenCoding Assignment 18-WPS Officetamj tamjNoch keine Bewertungen
- JSF + JPA + JasperReports (Ireport) Part 2 - Ramki Java BlogDokument7 SeitenJSF + JPA + JasperReports (Ireport) Part 2 - Ramki Java BlogMartin MurciegoNoch keine Bewertungen
- Excel Formulas and Functions 2021-The Intermediate Level Step byDokument122 SeitenExcel Formulas and Functions 2021-The Intermediate Level Step bymaolegu100% (3)
- Oracle Goldengate: Oracle Installation and Setup Guide 11 Release 2 (11.2.1.0.0)Dokument188 SeitenOracle Goldengate: Oracle Installation and Setup Guide 11 Release 2 (11.2.1.0.0)kashifmeoNoch keine Bewertungen
- GB-T 5137.1-2002 Test Methods of Safety Glazing Materials Used On Road Vehicles Part1 Mechanical Properties TestsDokument14 SeitenGB-T 5137.1-2002 Test Methods of Safety Glazing Materials Used On Road Vehicles Part1 Mechanical Properties TestsRandyzhuNoch keine Bewertungen
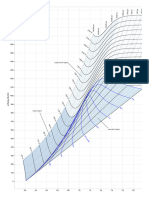
- Mollier Enthalpy Entropy Chart For Steam - US UnitsDokument1 SeiteMollier Enthalpy Entropy Chart For Steam - US Unitslin tongNoch keine Bewertungen
- Origin and Structure of The EarthDokument8 SeitenOrigin and Structure of The EarthRobin Suarez ViladoNoch keine Bewertungen
- Astm A394 2008 PDFDokument6 SeitenAstm A394 2008 PDFJavier Ricardo Romero BohorquezNoch keine Bewertungen
- Programming For Problem SolvingDokument5 SeitenProgramming For Problem SolvingAPOLLO Sem 4 I.T.Noch keine Bewertungen
- Microgrid Modeling and Grid Interconnection StudiesDokument71 SeitenMicrogrid Modeling and Grid Interconnection StudiesVeeravasantharao BattulaNoch keine Bewertungen
- LTE Rach ProcedureDokument4 SeitenLTE Rach ProcedureDeepak JammyNoch keine Bewertungen
- Applications of Modern RF PhotonicsDokument213 SeitenApplications of Modern RF PhotonicsrmcmillanNoch keine Bewertungen
- Bruh I Hate File Handling - CPPDokument3 SeitenBruh I Hate File Handling - CPPJayson AmodiaNoch keine Bewertungen
- Asme Ix Test 1Dokument8 SeitenAsme Ix Test 1RedzuanNoch keine Bewertungen
- Sample Paper III (Science) - Question PaperDokument21 SeitenSample Paper III (Science) - Question Paperfathima MiranNoch keine Bewertungen
- AWK - WikipediaDokument1 SeiteAWK - WikipediachassisdNoch keine Bewertungen
- CISCO Router Software - Configuration PDFDokument408 SeitenCISCO Router Software - Configuration PDFasalihovicNoch keine Bewertungen
- Lecture 2: Stacks and Queues: CSE 373: Data Structures and AlgorithmsDokument31 SeitenLecture 2: Stacks and Queues: CSE 373: Data Structures and AlgorithmsTawsifNoch keine Bewertungen
- Ball Charge ManagementDokument14 SeitenBall Charge ManagementSalud Y SucesosNoch keine Bewertungen
- Reaktor 5 Core Manual EnglishDokument210 SeitenReaktor 5 Core Manual EnglishmonistoNoch keine Bewertungen
- Hazardous Area ClassificationDokument36 SeitenHazardous Area Classificationvenkeeku100% (1)
- EC SyllDokument4 SeitenEC SyllDDIYNoch keine Bewertungen
- Chapter 1: Coding Decoding: Important Note: It Is Good To Avoid Pre-Defined Coding Rule To Write A Coded MessageDokument7 SeitenChapter 1: Coding Decoding: Important Note: It Is Good To Avoid Pre-Defined Coding Rule To Write A Coded MessageUmamNoch keine Bewertungen