Das könnte Ihnen auch gefallen
- Clinical Skills ChecklistDokument4 SeitenClinical Skills Checklistapi-489851583Noch keine Bewertungen
- Practical Skills Evaluation SheetDokument98 SeitenPractical Skills Evaluation SheetLa Gracias TunaNoch keine Bewertungen
- Abonamente Beneficii Medicale MedicoverDokument22 SeitenAbonamente Beneficii Medicale MedicoverClaudia NijimNoch keine Bewertungen
- TCCC Skill Sets by Responder Level Master 190422 ApprovedDokument4 SeitenTCCC Skill Sets by Responder Level Master 190422 ApprovedIon MarinNoch keine Bewertungen
- TCCC Skill Set Level 2024Dokument4 SeitenTCCC Skill Set Level 2024Reza Devianto HambaliNoch keine Bewertungen
- NURS20171 - Assessment 2 - Artefact 2 CompletedDokument7 SeitenNURS20171 - Assessment 2 - Artefact 2 CompletedSarah HarwoodNoch keine Bewertungen
- TCCC Skill Sets by Provider Level 0904Dokument2 SeitenTCCC Skill Sets by Provider Level 0904beerensdNoch keine Bewertungen
- Resuscitation Trolley Checklist: RrcsuDokument7 SeitenResuscitation Trolley Checklist: RrcsuPatrick SimembaNoch keine Bewertungen
- VTOS Crew Competency MatrixDokument1 SeiteVTOS Crew Competency MatrixNMHaNoch keine Bewertungen
- List of Priority Medical Devices in The Context of COVID-19Dokument4 SeitenList of Priority Medical Devices in The Context of COVID-19Joresp EspinozaNoch keine Bewertungen
- phem-competency-frameworkDokument3 Seitenphem-competency-frameworkBelal HasanNoch keine Bewertungen
- Clinical Privilege Request - Dr. MD RoknuggamanDokument6 SeitenClinical Privilege Request - Dr. MD RoknuggamanMd RoknuggamanNoch keine Bewertungen
- A. Exhibit A - Appendix C - MCU Matrix - NewDokument1 SeiteA. Exhibit A - Appendix C - MCU Matrix - NewJoko SriyantoNoch keine Bewertungen
- Pediatrics Intensive Care Unit: Presented By: Ms. Sandeep KaurDokument52 SeitenPediatrics Intensive Care Unit: Presented By: Ms. Sandeep KaurArchanaNoch keine Bewertungen
- Table 1.5.A Minimum Requirements For Training Curricula (1.5.2)Dokument1 SeiteTable 1.5.A Minimum Requirements For Training Curricula (1.5.2)lyndon_baker_1Noch keine Bewertungen
- Autorizações Atendimentos PSDokument2 SeitenAutorizações Atendimentos PSthaysts2303Noch keine Bewertungen
- Ast Pamki Final 2015 - 230316 - 112711Dokument9 SeitenAst Pamki Final 2015 - 230316 - 112711Novia khasanahNoch keine Bewertungen
- Clinical Pathway Stroke IskemikDokument2 SeitenClinical Pathway Stroke IskemikRizki Pawestri100% (2)
- Ic Drive Copy Essential-Of-Healthcare Equipment SuppliesDokument4 SeitenIc Drive Copy Essential-Of-Healthcare Equipment Suppliesapi-688305379Noch keine Bewertungen
- Pocus en Shock SepticoDokument9 SeitenPocus en Shock SepticoJaime Guillén OrdóñezNoch keine Bewertungen
- Daftar Alat Kesehatan PMK Nomor 56 Tahun 2014Dokument35 SeitenDaftar Alat Kesehatan PMK Nomor 56 Tahun 2014RaniNoch keine Bewertungen
- Stretching AnatomyDokument3 SeitenStretching AnatomyMedShareNoch keine Bewertungen
- Cardiothoracic Surgery v1.0Dokument19 SeitenCardiothoracic Surgery v1.0Ko YeKhaeNoch keine Bewertungen
- Daily Lab ProcessesDokument3 SeitenDaily Lab ProcessesKathrine Ann FavoritoNoch keine Bewertungen
- Pre-Op Lab Testing GuidelinesDokument36 SeitenPre-Op Lab Testing Guidelinesramzi MohamedNoch keine Bewertungen
- Course requirementsDokument2 SeitenCourse requirementsSurendra RamkissoonNoch keine Bewertungen
- EASA PPL Syllabus of Theoretical KnowledgeDokument3 SeitenEASA PPL Syllabus of Theoretical KnowledgeJohnNoch keine Bewertungen
- Emergency Laparotomy PDFDokument13 SeitenEmergency Laparotomy PDFbushra mughalNoch keine Bewertungen
- Connective Tissue Disease-Associated Interstitial Lung DiseaseDokument35 SeitenConnective Tissue Disease-Associated Interstitial Lung DiseaseSilp SatjawattanavimolNoch keine Bewertungen
- Poultry Histopathology Tissue Collection - General Guide : Sample Obvious Lesions!Dokument1 SeitePoultry Histopathology Tissue Collection - General Guide : Sample Obvious Lesions!Maamar AmamraNoch keine Bewertungen
- Alat Gawat DaruratDokument4 SeitenAlat Gawat Daruratjaja nugrahaNoch keine Bewertungen
- Friedman 1978Dokument7 SeitenFriedman 1978nicolas.sierra1Noch keine Bewertungen
- Surgical Instrumentation Program: Training Surgical Planning IQX-FT-003-BUCDokument17 SeitenSurgical Instrumentation Program: Training Surgical Planning IQX-FT-003-BUCapi-653899733Noch keine Bewertungen
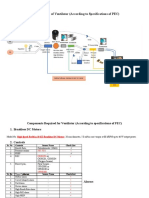
- Ventilator Block Diagram and Component SpecificationsDokument2 SeitenVentilator Block Diagram and Component SpecificationsMohammad Asmat Ullah KhanNoch keine Bewertungen
- For Nece DoresDokument8 SeitenFor Nece DoresvaldileiNoch keine Bewertungen
- Resuscitation Trolley Checking and Equipment (Adult & Neonatal)Dokument10 SeitenResuscitation Trolley Checking and Equipment (Adult & Neonatal)Michael Phratama NugrahaNoch keine Bewertungen
- Intraoperative Preparations A. Instruments, Supplies and Equipment NeededDokument16 SeitenIntraoperative Preparations A. Instruments, Supplies and Equipment NeededDhen MarcNoch keine Bewertungen
- Puskesmas Biaro schedules medical equipment maintenance in 2019Dokument32 SeitenPuskesmas Biaro schedules medical equipment maintenance in 2019Asma witaNoch keine Bewertungen
- Copy Intro Supply ListDokument2 SeitenCopy Intro Supply Listapi-688305379Noch keine Bewertungen
- 68 - ISO 18436 - 2 Annex - ADokument3 Seiten68 - ISO 18436 - 2 Annex - ACeliocp Pinheiro100% (1)
- Neonatal-Ventilation-brochure-V2.2.x Brochure en ELO20180806N.00Dokument8 SeitenNeonatal-Ventilation-brochure-V2.2.x Brochure en ELO20180806N.00Ashik AssimNoch keine Bewertungen
- GE Logiq e Probes (BT12)Dokument2 SeitenGE Logiq e Probes (BT12)rabbani.moNoch keine Bewertungen
- Edhemovic - Surgical Oncology 2014 09 20 PDFDokument21 SeitenEdhemovic - Surgical Oncology 2014 09 20 PDFRasheed ElayyanNoch keine Bewertungen
- Oct-2023-Durb-Agenda-Item3dDokument28 SeitenOct-2023-Durb-Agenda-Item3dI Made AryanaNoch keine Bewertungen
- Comprehensive Guide to Body MRI Protocols and SequencesDokument136 SeitenComprehensive Guide to Body MRI Protocols and SequencesRadiologi Mika bintaroNoch keine Bewertungen
- Cleaning and Repair Boiler and Shoot Blower Scope of Works and SupplyDokument1 SeiteCleaning and Repair Boiler and Shoot Blower Scope of Works and SupplydharwinNoch keine Bewertungen
- JIG Standards Session G ODonnell N MasonDokument40 SeitenJIG Standards Session G ODonnell N Masonsamson anyumbaNoch keine Bewertungen
- Types of Rectal SurgeryDokument1 SeiteTypes of Rectal SurgeryPatrick PengosroNoch keine Bewertungen
- Paket LabDokument1 SeitePaket LabriaNoch keine Bewertungen
- First Aid Kit ContentsDokument6 SeitenFirst Aid Kit ContentsOleg ShubinNoch keine Bewertungen
- DOAC Webinar 2 Slide HandoutDokument58 SeitenDOAC Webinar 2 Slide HandoutStacie PenkovaNoch keine Bewertungen
- Journal Homepage: - : IntroductionDokument7 SeitenJournal Homepage: - : IntroductionIJAR JOURNALNoch keine Bewertungen
- US Liver Doppler OnlyDokument8 SeitenUS Liver Doppler OnlymicropocketfilmsNoch keine Bewertungen
- TABEL KLASIFIKASI TEKNOLOGI ALAT ELEKTROMEDIK by DarmaDokument4 SeitenTABEL KLASIFIKASI TEKNOLOGI ALAT ELEKTROMEDIK by DarmaGamerBro IDNoch keine Bewertungen
- Daftar Peralatan Kesehatan di Pelayanan Gawat Darurat dan Penyakit DalamDokument46 SeitenDaftar Peralatan Kesehatan di Pelayanan Gawat Darurat dan Penyakit DalamrusmilawatiNoch keine Bewertungen
- Bidirectional Cavopulmonary Shunt With Additional PBF - Gerelli2012Dokument7 SeitenBidirectional Cavopulmonary Shunt With Additional PBF - Gerelli2012Jose YoveraNoch keine Bewertungen
- Laparoscopic Hysterectomy and Decision When and WH PDFDokument5 SeitenLaparoscopic Hysterectomy and Decision When and WH PDFDian SiregarNoch keine Bewertungen
- Rih - Pedi Chest Siemens Definition As20 Protocol: Indications - Infection, Pulmonary Nodule, Mass, Effusion, EmpyemaDokument1 SeiteRih - Pedi Chest Siemens Definition As20 Protocol: Indications - Infection, Pulmonary Nodule, Mass, Effusion, Empyemaakhmad mustainNoch keine Bewertungen
- Operation Manual: Thumper Model 1007CCV Mechanical CPR SystemDokument46 SeitenOperation Manual: Thumper Model 1007CCV Mechanical CPR SystemKevin Isaac NamesNoch keine Bewertungen
- PMS Color Chart PDFDokument1 SeitePMS Color Chart PDFPradit SaraonNoch keine Bewertungen
- 2013 State of Oklahoma EMS ProtocolsDokument493 Seiten2013 State of Oklahoma EMS ProtocolsMarian Ioan-Lucian100% (1)
- Australian National Search and Rescue Council ManualDokument234 SeitenAustralian National Search and Rescue Council ManualShane Briggs100% (7)
- Infectious DiseaseDokument82 SeitenInfectious DiseaseMedical videos67% (3)
- New Cellular Aberration Lecture2010Dokument271 SeitenNew Cellular Aberration Lecture2010John Russell MoralesNoch keine Bewertungen
- BHP Masuk 2016Dokument39 SeitenBHP Masuk 2016agustinardiNoch keine Bewertungen
- OriginalDokument34 SeitenOriginalabdullah2020Noch keine Bewertungen
- Colostomy CareDokument13 SeitenColostomy CareLord Pozak MillerNoch keine Bewertungen
- NCM 417 - Final Exam 2015Dokument12 SeitenNCM 417 - Final Exam 2015Mae DacerNoch keine Bewertungen
- 2020 ISMP - Smart Infusion Pumps-FINALDokument38 Seiten2020 ISMP - Smart Infusion Pumps-FINALmochkurniawanNoch keine Bewertungen
- Sentinel Pump Manual - 2Dokument13 SeitenSentinel Pump Manual - 2Michael LevitNoch keine Bewertungen
- CVC - B Braun - CertofixDokument14 SeitenCVC - B Braun - CertofixMargaretta LimawanNoch keine Bewertungen
- IV CalculationsDokument31 SeitenIV CalculationschanaNoch keine Bewertungen
- NEW CBT 2021 Summary Q 1Dokument34 SeitenNEW CBT 2021 Summary Q 1himali ranasingheNoch keine Bewertungen
- Purpose: Billroth I, More Formally Billroth's Operation I, Is AnDokument8 SeitenPurpose: Billroth I, More Formally Billroth's Operation I, Is AnttriggerNoch keine Bewertungen
- HISTORICAL EVOLUTION OF IV STANDARDSDokument45 SeitenHISTORICAL EVOLUTION OF IV STANDARDSjodipotpot77% (13)
- Nursing Practice ConceptDokument19 SeitenNursing Practice ConceptpauchanmnlNoch keine Bewertungen
- En - 2025-123-1837662383-Nursing KPI 2013 - FINALDokument9 SeitenEn - 2025-123-1837662383-Nursing KPI 2013 - FINALIamnurse NylejNoch keine Bewertungen
- Arcomed Syramed USP-6000 - Maintenance ManualDokument43 SeitenArcomed Syramed USP-6000 - Maintenance ManualDino Abreu50% (2)
- Funda Past Board 2 Brilliant ChoiceDokument5 SeitenFunda Past Board 2 Brilliant Choicecoffee bean100% (1)
- NCM 112 Lesson3Dokument6 SeitenNCM 112 Lesson3Trisha LopezNoch keine Bewertungen
- November 2008 NLE Practice IVDokument19 SeitenNovember 2008 NLE Practice IVEJ Cubero, R☤NNoch keine Bewertungen
- Lactated Ringer's Injection GuideDokument10 SeitenLactated Ringer's Injection GuideJeannette Richelle DacilloNoch keine Bewertungen
- BMJ g7620 FullDokument10 SeitenBMJ g7620 FullRui PenedaNoch keine Bewertungen
- Medical Dosage Calculations Cheat SheetDokument14 SeitenMedical Dosage Calculations Cheat SheetJennifer Jaworsky100% (3)
- Central Venous CatheterDokument2 SeitenCentral Venous CatheterErick ToHuNoch keine Bewertungen
- Fundamentals of NursingDokument14 SeitenFundamentals of NursingFreeNursingNotes95% (63)
- Case Study,,,,,,pneumoniaDokument52 SeitenCase Study,,,,,,pneumoniaJaillah Reigne Cura0% (1)
- NW Newborn Drug Protocol - Calcium Gluconate AdministrationDokument2 SeitenNW Newborn Drug Protocol - Calcium Gluconate AdministrationElla Masliana Dewi100% (1)
- IV Insertion ProcedureDokument11 SeitenIV Insertion ProcedureEdelweiss Marie Cayetano100% (1)
- Short Keys and Formulas of ExcelDokument40 SeitenShort Keys and Formulas of ExcelSattar CANoch keine Bewertungen
- Braun Infusomat SpaceDokument70 SeitenBraun Infusomat Spacelmver04Noch keine Bewertungen
- Intravenous Maintenance Fluid Therapy in The Pedia PDFDokument18 SeitenIntravenous Maintenance Fluid Therapy in The Pedia PDFAdrianRuizNoch keine Bewertungen