Das könnte Ihnen auch gefallen
- Potassium Level Changes - Arrhythmia Contributing Factor in Chronic Kidney Disease PatientsDokument4 SeitenPotassium Level Changes - Arrhythmia Contributing Factor in Chronic Kidney Disease PatientssigitNoch keine Bewertungen
- Hyponatremia in Stroke: Cerebral Salt Wasting Versus Syndrome of Inappropriate Anti-DiuresisDokument22 SeitenHyponatremia in Stroke: Cerebral Salt Wasting Versus Syndrome of Inappropriate Anti-DiuresisJames BarriosNoch keine Bewertungen
- Elevated Calcium After Acute Ischemic Stroke: Association With A Poor Short-Term Outcome and Long-Term MortalityDokument6 SeitenElevated Calcium After Acute Ischemic Stroke: Association With A Poor Short-Term Outcome and Long-Term MortalityMuhammad Ilham FarizNoch keine Bewertungen
- TrnsltcitooooDokument7 SeitenTrnsltcitooooAhmad SyaukatNoch keine Bewertungen
- Objective: Methods: Results: Conclusions:: What's Known On This SubjectDokument12 SeitenObjective: Methods: Results: Conclusions:: What's Known On This SubjectAnonymous AzkHFgubueNoch keine Bewertungen
- 2 PDFDokument6 Seiten2 PDFLisa HikmawanNoch keine Bewertungen
- Early Prediction of Severity StrokeDokument11 SeitenEarly Prediction of Severity StrokeainihanifiahNoch keine Bewertungen
- Therapeutic Approach in Patients With Dysnatraemias: Original ArticleDokument6 SeitenTherapeutic Approach in Patients With Dysnatraemias: Original ArticleJuan Manuel MonteroNoch keine Bewertungen
- Full Text 01Dokument8 SeitenFull Text 01febyNoch keine Bewertungen
- Hipernatremia en UCIDokument7 SeitenHipernatremia en UCIcolo_med1077Noch keine Bewertungen
- Park2019 Article RecoveryFromAcuteKidneyInjuryADokument11 SeitenPark2019 Article RecoveryFromAcuteKidneyInjuryALeandro NogueiraNoch keine Bewertungen
- Preoperative Serum Bicarbonate Levels Predict Acute Kidney Injury After Cardiac SurgeryDokument11 SeitenPreoperative Serum Bicarbonate Levels Predict Acute Kidney Injury After Cardiac SurgeryRoni ArmandaNoch keine Bewertungen
- Acidosis Metabolica en UciDokument5 SeitenAcidosis Metabolica en UciPedro Fernando GiraldoNoch keine Bewertungen
- Admission Serum Potassium in Patients With Acute Myocardial InfarctionDokument10 SeitenAdmission Serum Potassium in Patients With Acute Myocardial InfarctionSurya UlhaqNoch keine Bewertungen
- Hyper Na CorrectionDokument11 SeitenHyper Na CorrectionalizanNoch keine Bewertungen
- Trial of Early, Goal-Directed Resuscitation For Septic ShockDokument11 SeitenTrial of Early, Goal-Directed Resuscitation For Septic Shockapi-308365861Noch keine Bewertungen
- 09 Is Routine Supplementation Therapy Calcium and Vitamin D Useful After Total ThyroidectomyDokument5 Seiten09 Is Routine Supplementation Therapy Calcium and Vitamin D Useful After Total ThyroidectomyBridia BogarNoch keine Bewertungen
- Ojsadmin, 176Dokument4 SeitenOjsadmin, 176Signor 2019Noch keine Bewertungen
- Hypernatremia in Hospitalized Children 7380Dokument4 SeitenHypernatremia in Hospitalized Children 7380menesesgilbertmd333Noch keine Bewertungen
- HYPERKALEMIADokument9 SeitenHYPERKALEMIAKhánh UyênNoch keine Bewertungen
- Cerebral Salt Wasting Syndrome ReviewDokument6 SeitenCerebral Salt Wasting Syndrome ReviewSoewira Sastra100% (1)
- Laboratory Risk Factors For Hospital Mortality in AcutelyDokument7 SeitenLaboratory Risk Factors For Hospital Mortality in AcutelypmunizNoch keine Bewertungen
- KDIGO Acute Hyperkalemia Conf Report FINALDokument9 SeitenKDIGO Acute Hyperkalemia Conf Report FINALJuan Carlos Kuan HigueraNoch keine Bewertungen
- Terapi Suplementasi Oksigen Pada STEMI 3Dokument31 SeitenTerapi Suplementasi Oksigen Pada STEMI 3Yeny ElfiyantiNoch keine Bewertungen
- Epilepsia - 2011 - Halawa - Hyponatremia and Risk of Seizures A Retrospective Cross Sectional StudyDokument4 SeitenEpilepsia - 2011 - Halawa - Hyponatremia and Risk of Seizures A Retrospective Cross Sectional StudyMecuc YecucNoch keine Bewertungen
- Age +estimated+glomerular+filtration+rate+and+ejection+fraction+score+predicts+contrast-Induced+acute+kidney+injury+in+patients+with+diabetes+and+chronic+kidney+disease +insight+from+the+TRACK-D+studyDokument5 SeitenAge +estimated+glomerular+filtration+rate+and+ejection+fraction+score+predicts+contrast-Induced+acute+kidney+injury+in+patients+with+diabetes+and+chronic+kidney+disease +insight+from+the+TRACK-D+studyangga_darmawan26Noch keine Bewertungen
- Serum Uric Acid As An Independent Predictor of Recurrence in Ischemic Stroke PatientsDokument4 SeitenSerum Uric Acid As An Independent Predictor of Recurrence in Ischemic Stroke PatientssourceofnotesNoch keine Bewertungen
- Efficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryDokument9 SeitenEfficacy of Hyperventilation, Blood Pressure Elevation, and Metabolic Suppression Therapy in Controlling Intracranial Pressure After Head InjuryAik NoeraNoch keine Bewertungen
- Predicting Spontaneous Conversion To Sinus Rhythm in - 2020 - European Journal oDokument9 SeitenPredicting Spontaneous Conversion To Sinus Rhythm in - 2020 - European Journal oStefan LaurentiuNoch keine Bewertungen
- Babandi Et Al., (2017) BJMLS, 2 (1) :: Level Among Hypertensive Patients in Kano-Nigeria BJMLS. 2Dokument8 SeitenBabandi Et Al., (2017) BJMLS, 2 (1) :: Level Among Hypertensive Patients in Kano-Nigeria BJMLS. 2idiNoch keine Bewertungen
- SLED Vs CRRT PDFDokument9 SeitenSLED Vs CRRT PDFquilino2012Noch keine Bewertungen
- Timing RRT AkiDokument9 SeitenTiming RRT AkidharmaNoch keine Bewertungen
- American Journal of Emergency MedicineDokument3 SeitenAmerican Journal of Emergency MedicineRina ErlinaNoch keine Bewertungen
- Urologi Jurnal InternasionalDokument9 SeitenUrologi Jurnal InternasionalMyisha UfairaNoch keine Bewertungen
- 10.1007@s11739 019 02196 ZDokument10 Seiten10.1007@s11739 019 02196 ZMaharani Sari NastitiNoch keine Bewertungen
- Restrictive Fluids in Septic Shock. NEJM 2022Dokument12 SeitenRestrictive Fluids in Septic Shock. NEJM 2022neeraj SinghNoch keine Bewertungen
- Meta-Analysis: The Safety and Ef Ficacy of Vaptans (Tolvaptan, Satavaptan and Lixivaptan) in Cirrhosis With Ascites or HyponatraemiaDokument8 SeitenMeta-Analysis: The Safety and Ef Ficacy of Vaptans (Tolvaptan, Satavaptan and Lixivaptan) in Cirrhosis With Ascites or HyponatraemiaHadi KuriryNoch keine Bewertungen
- 35th Vicenza Course On Aki & CRRT: Selected Abstracts From TheDokument27 Seiten35th Vicenza Course On Aki & CRRT: Selected Abstracts From TheMARIA LEIVANoch keine Bewertungen
- HipercalcemiaDokument4 SeitenHipercalcemiadrichard123Noch keine Bewertungen
- Hidronefrosis 3Dokument11 SeitenHidronefrosis 3Zwinglie SandagNoch keine Bewertungen
- Print 2 PDFDokument6 SeitenPrint 2 PDFfk unswagatiNoch keine Bewertungen
- Ekg Dan SyncopeDokument6 SeitenEkg Dan SyncopeDIdit FAjar NUgrohoNoch keine Bewertungen
- Causes of Syncope in Patients With AlzheDokument8 SeitenCauses of Syncope in Patients With AlzheMichael VavosaNoch keine Bewertungen
- Resuscitation Fluid Composition in Acute Kidney Injury in Critical IllnessDokument2 SeitenResuscitation Fluid Composition in Acute Kidney Injury in Critical IllnessDe Frede EditoreNoch keine Bewertungen
- Effects of Magnesium On Central Arterial Compliance in PreeclampsiaDokument8 SeitenEffects of Magnesium On Central Arterial Compliance in PreeclampsiaJuana Maria Montoya RamirezNoch keine Bewertungen
- Liu2017 Article HypokalemiaIsABiochemicalSignaDokument7 SeitenLiu2017 Article HypokalemiaIsABiochemicalSignaAngélica Téllez ANoch keine Bewertungen
- Fifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDokument6 SeitenFifteen-Year Experience: Open Heart Surgery in Patients With End-Stage Renal FailureDavid RamirezNoch keine Bewertungen
- ScribdDokument8 SeitenScribdMaria JuliaNoch keine Bewertungen
- Advances in Medical SciencesDokument6 SeitenAdvances in Medical SciencesMihaela-Alexandra PopNoch keine Bewertungen
- Burden of Sodium Abnormalities in Patients Hospitalized For Heart FailureDokument7 SeitenBurden of Sodium Abnormalities in Patients Hospitalized For Heart FailureVincent ReyesNoch keine Bewertungen
- Use of Conivaptan To Allow Aggressive Hydration To Prevent Tumor Lysis Syndrome in A Pediatric Patient With Large-Cell Lymphoma and SIADHDokument5 SeitenUse of Conivaptan To Allow Aggressive Hydration To Prevent Tumor Lysis Syndrome in A Pediatric Patient With Large-Cell Lymphoma and SIADHmaryNoch keine Bewertungen
- Circulation 2011 1250 9Dokument33 SeitenCirculation 2011 1250 9Carminia RivasNoch keine Bewertungen
- Clinical Validation For The Aldosterone To Renin.19Dokument12 SeitenClinical Validation For The Aldosterone To Renin.19dasdNoch keine Bewertungen
- Nimodipine in Aneurysmal Subarachnoid Hemorrhage: A Randomized Study of Intravenous or Peroral AdministrationDokument5 SeitenNimodipine in Aneurysmal Subarachnoid Hemorrhage: A Randomized Study of Intravenous or Peroral AdministrationMiftakhul BaitiNoch keine Bewertungen
- Konishi 2008Dokument6 SeitenKonishi 2008PROF. ERWIN M. GLOBIO, MSITNoch keine Bewertungen
- 67 Ej20-0159Dokument9 Seiten67 Ej20-0159desconocido 123 ambticonNoch keine Bewertungen
- Jurnal Kedokteran Dan Kesehatan IndonesiaDokument11 SeitenJurnal Kedokteran Dan Kesehatan IndonesiaTeuku Ilham AkbarNoch keine Bewertungen
- Eur J Echocardiogr 2007 Scardovi 30 6Dokument7 SeitenEur J Echocardiogr 2007 Scardovi 30 6Eman SadikNoch keine Bewertungen
- Pi Is 2590059522000863Dokument4 SeitenPi Is 2590059522000863nina2911Noch keine Bewertungen
- KDIGO Optimal Anemia Management - Scope For Public ReviewDokument13 SeitenKDIGO Optimal Anemia Management - Scope For Public ReviewDesi HutapeaNoch keine Bewertungen
- Musa 2015Dokument15 SeitenMusa 2015Jose Luis Morales BautistaNoch keine Bewertungen
- Patof Spell PDFDokument3 SeitenPatof Spell PDFAnggi CalapiNoch keine Bewertungen
- Spond Ylo ArthritisDokument5 SeitenSpond Ylo ArthritisSuwandi AlghozyNoch keine Bewertungen
- Peritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDokument9 SeitenPeritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDesi HutapeaNoch keine Bewertungen
- 702 FullDokument10 Seiten702 FullDesi HutapeaNoch keine Bewertungen
- Peritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDokument6 SeitenPeritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDesi HutapeaNoch keine Bewertungen
- Peritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDokument6 SeitenPeritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDesi HutapeaNoch keine Bewertungen
- Renal PhysiologyDokument7 SeitenRenal PhysiologyLucas TheotonioNoch keine Bewertungen
- Current Management of Acquired Solitary KidneyDokument4 SeitenCurrent Management of Acquired Solitary KidneyDesi HutapeaNoch keine Bewertungen
- Peritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDokument9 SeitenPeritoneal Dialysis-Related Peritonitis Caused by Pseudomonas Species: Insight From A Post-Millennial Case SeriesDesi HutapeaNoch keine Bewertungen
- ANCA Glomerulonephritis and VasculitisDokument12 SeitenANCA Glomerulonephritis and VasculitisSofía Elizabeth BlancoNoch keine Bewertungen
- Peritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDokument6 SeitenPeritoneal Dialysis-Associated Peritonitis: Cheuk-Chun Szeto and Philip Kam-Tao LiDesi HutapeaNoch keine Bewertungen
- 796 FullDokument3 Seiten796 FullDesi HutapeaNoch keine Bewertungen
- Use of Vitamin D Drops Leading To Kidney Failure in A 54-Year-Old ManDokument5 SeitenUse of Vitamin D Drops Leading To Kidney Failure in A 54-Year-Old ManDesi HutapeaNoch keine Bewertungen
- ANCA Glomerulonephritis and VasculitisDokument12 SeitenANCA Glomerulonephritis and VasculitisSofía Elizabeth BlancoNoch keine Bewertungen
- Onco Neph PDFDokument9 SeitenOnco Neph PDFNarinder SharmaNoch keine Bewertungen
- s41581 018 0077 4 PDFDokument15 Seitens41581 018 0077 4 PDFDesi HutapeaNoch keine Bewertungen
- Relationship of Kidney Injury Biomarkers With Long-Term Cardiovascular Outcomes After Cardiac SurgeryDokument9 SeitenRelationship of Kidney Injury Biomarkers With Long-Term Cardiovascular Outcomes After Cardiac SurgeryDesi HutapeaNoch keine Bewertungen
- 796 FullDokument3 Seiten796 FullDesi HutapeaNoch keine Bewertungen
- s41581 018 0077 4 PDFDokument15 Seitens41581 018 0077 4 PDFDesi HutapeaNoch keine Bewertungen
- CJN 10640918 FullDokument8 SeitenCJN 10640918 FullDesi HutapeaNoch keine Bewertungen
- 641 FullDokument12 Seiten641 FullDesi HutapeaNoch keine Bewertungen
- Nrneph 2017 2Dokument17 SeitenNrneph 2017 2Desi HutapeaNoch keine Bewertungen
- FastDokument10 SeitenFastAnonymous Lxho3INoch keine Bewertungen
- NephrologyDokument10 SeitenNephrologyDesi HutapeaNoch keine Bewertungen
- CJN 09630818 FullDokument10 SeitenCJN 09630818 FullDesi HutapeaNoch keine Bewertungen
- KDIGO Dialysis Initiation Conf Report in PressDokument11 SeitenKDIGO Dialysis Initiation Conf Report in PressDesi HutapeaNoch keine Bewertungen
- CJN 09630818 FullDokument10 SeitenCJN 09630818 FullDesi HutapeaNoch keine Bewertungen
- 28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDokument5 Seiten28-Year-Old Man With Crohn Disease and Hematuria: Residents ' ClinicDesi HutapeaNoch keine Bewertungen
- Healthcare ProfessionalismDokument28 SeitenHealthcare ProfessionalismAnjo CincoNoch keine Bewertungen
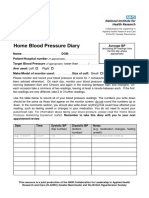
- Home Blood Pressure DiaryDokument2 SeitenHome Blood Pressure DiaryCherieNoch keine Bewertungen
- Nicu ReflectionDokument2 SeitenNicu Reflectionapi-422763411100% (1)
- Comparison of The Lma-Proseal and Lma-Classic in ChildrenDokument4 SeitenComparison of The Lma-Proseal and Lma-Classic in ChildrenBobby AksandaNoch keine Bewertungen
- Pre Employment Occupational Health FormDokument7 SeitenPre Employment Occupational Health Formlinks2309Noch keine Bewertungen
- Oral RevalidaDokument3 SeitenOral RevalidaJaye DangoNoch keine Bewertungen
- TEST 1 Nursing FundamentalsDokument11 SeitenTEST 1 Nursing FundamentalsLisa Keefer100% (1)
- GRK Extrospection Excerpt PDFDokument7 SeitenGRK Extrospection Excerpt PDFChrysoula GkaniNoch keine Bewertungen
- 2.segaert FINALDokument42 Seiten2.segaert FINALBagoes LoekmanNoch keine Bewertungen
- Tooth Discoloration Hypomineralization and HypoplasiaDokument5 SeitenTooth Discoloration Hypomineralization and HypoplasiamirfanulhaqNoch keine Bewertungen
- Nursing Process DiagnosisDokument20 SeitenNursing Process DiagnosisGabz Gabby100% (1)
- Cure For A Stiff Neck-Chi KungDokument2 SeitenCure For A Stiff Neck-Chi Kungheroig100% (2)
- Not GlaucomaDokument5 SeitenNot GlaucomaFabio LuccheseNoch keine Bewertungen
- AplDokument37 SeitenApladitiya tegarNoch keine Bewertungen
- Surgical SafetyDokument23 SeitenSurgical SafetyNimi BatuboNoch keine Bewertungen
- Course List For The Bachelor of Pharmacy (Honours) - My - UQ - The University of Queensland, AustraliaDokument2 SeitenCourse List For The Bachelor of Pharmacy (Honours) - My - UQ - The University of Queensland, AustraliaLy Huyen TranNoch keine Bewertungen
- Lmccii GuideDokument56 SeitenLmccii Guideaaycee100% (1)
- Team PerceptionDokument3 SeitenTeam PerceptionSupriadi HardiantoNoch keine Bewertungen
- Laser Retinopexy PDFDokument4 SeitenLaser Retinopexy PDFveerroxxNoch keine Bewertungen
- Oral Hygiene InstructionsDokument2 SeitenOral Hygiene Instructionstepokpantat100% (1)
- Guidelines For APE 2021 With Drug Testing ROYCE HOTELDokument3 SeitenGuidelines For APE 2021 With Drug Testing ROYCE HOTELJm CayabyabNoch keine Bewertungen
- ACLS DrugDokument7 SeitenACLS DrugPhongsatorn Thunin100% (1)
- Uti in PregnancyDokument42 SeitenUti in Pregnancydeepak122Noch keine Bewertungen
- As Far As Possible - en ISO 14971Dokument19 SeitenAs Far As Possible - en ISO 14971Kanwal Jit Singh100% (1)
- Benign Prostat HiperplasiaDokument17 SeitenBenign Prostat HiperplasiahawhawnurNoch keine Bewertungen
- TPNDokument57 SeitenTPNPeace Andong PerochoNoch keine Bewertungen
- Case Study HFMD :)Dokument15 SeitenCase Study HFMD :)Princess CavestaniNoch keine Bewertungen
- Bible of Bee Venom TherapyDokument0 SeitenBible of Bee Venom TherapypaulxeNoch keine Bewertungen
- Drug Study - DiazepamDokument2 SeitenDrug Study - DiazepamCerie Anne Olay40% (5)
- Coronary Artery Disease Congestive Heart Failure HypertensionDokument28 SeitenCoronary Artery Disease Congestive Heart Failure HypertensionNocReyesNoch keine Bewertungen
- Summary of Mary Claire Haver's The Galveston DietVon EverandSummary of Mary Claire Haver's The Galveston DietBewertung: 5 von 5 Sternen5/5 (1)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyVon EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyBewertung: 4.5 von 5 Sternen4.5/5 (2)
- Eat & Run: My Unlikely Journey to Ultramarathon GreatnessVon EverandEat & Run: My Unlikely Journey to Ultramarathon GreatnessNoch keine Bewertungen
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookVon EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookBewertung: 3.5 von 5 Sternen3.5/5 (2)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Von EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Bewertung: 4 von 5 Sternen4/5 (378)
- Forever Strong: A New, Science-Based Strategy for Aging WellVon EverandForever Strong: A New, Science-Based Strategy for Aging WellNoch keine Bewertungen
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonVon EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonBewertung: 3.5 von 5 Sternen3.5/5 (33)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingVon EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingBewertung: 4 von 5 Sternen4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeVon EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNoch keine Bewertungen
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthVon EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthBewertung: 4 von 5 Sternen4/5 (6)
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeVon EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeBewertung: 4 von 5 Sternen4/5 (3)
- Glucose Revolution: The Life-Changing Power of Balancing Your Blood SugarVon EverandGlucose Revolution: The Life-Changing Power of Balancing Your Blood SugarBewertung: 5 von 5 Sternen5/5 (351)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouVon EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNoch keine Bewertungen
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyVon EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNoch keine Bewertungen
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainVon EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainBewertung: 3.5 von 5 Sternen3.5/5 (38)
- Molecules of Emotion: Why You Feel the Way You FeelVon EverandMolecules of Emotion: Why You Feel the Way You FeelBewertung: 4 von 5 Sternen4/5 (128)
- Keto Friendly Recipes: Easy Keto For Busy PeopleVon EverandKeto Friendly Recipes: Easy Keto For Busy PeopleBewertung: 3.5 von 5 Sternen3.5/5 (2)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsVon EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsBewertung: 4 von 5 Sternen4/5 (49)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseVon EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseBewertung: 4.5 von 5 Sternen4.5/5 (84)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeVon EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeBewertung: 4 von 5 Sternen4/5 (3)
- The End of Craving: Recovering the Lost Wisdom of Eating WellVon EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellBewertung: 4.5 von 5 Sternen4.5/5 (81)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomVon EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomBewertung: 4 von 5 Sternen4/5 (1)
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthVon EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNoch keine Bewertungen
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondVon EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondBewertung: 4.5 von 5 Sternen4.5/5 (28)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeVon EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeBewertung: 5 von 5 Sternen5/5 (1)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodVon EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNoch keine Bewertungen
- Ultrametabolism: The Simple Plan for Automatic Weight LossVon EverandUltrametabolism: The Simple Plan for Automatic Weight LossBewertung: 4.5 von 5 Sternen4.5/5 (28)