Das könnte Ihnen auch gefallen
- Public Corporations: An IntroductionDokument13 SeitenPublic Corporations: An IntroductionAnonymous ZkmVfVgvQ0Noch keine Bewertungen
- Public CorporationDokument14 SeitenPublic Corporationiamyni86% (14)
- Nachura Notes Local GovernmentsDokument34 SeitenNachura Notes Local GovernmentsNowhere Man100% (16)
- THELMA VDA. DE CANILANG, Petitioner, vs. Hon. Court of Appeals and Great Pacific Life Assurance Corporation, Respondents. FactsDokument24 SeitenTHELMA VDA. DE CANILANG, Petitioner, vs. Hon. Court of Appeals and Great Pacific Life Assurance Corporation, Respondents. FactsMarkB15Noch keine Bewertungen
- Answers to 2017 Bar Exam on Labor and Social Legislation Part OneDokument30 SeitenAnswers to 2017 Bar Exam on Labor and Social Legislation Part OneBryner Laurito Diaz86% (22)
- Municipal Corporations - Public CorporationsDokument273 SeitenMunicipal Corporations - Public CorporationsFerdinandopoe97% (32)
- I. General Principles: Nachura Notes - Local Government (Kiddy)Dokument34 SeitenI. General Principles: Nachura Notes - Local Government (Kiddy)MarkB15100% (1)
- Validity and Effect of LegacyDokument6 SeitenValidity and Effect of LegacyMarkB15Noch keine Bewertungen
- Labor Case 09242019Dokument11 SeitenLabor Case 09242019MarkB15Noch keine Bewertungen
- SuccessionDokument24 SeitenSuccessiondinvNoch keine Bewertungen
- Validity and Effect of LegacyDokument6 SeitenValidity and Effect of LegacyMarkB15Noch keine Bewertungen
- Comparative Table of Legitimes and Intestate SharesDokument6 SeitenComparative Table of Legitimes and Intestate SharesMarkB15Noch keine Bewertungen
- Table of Legitimes - Testate and Intestate SuccessionDokument1 SeiteTable of Legitimes - Testate and Intestate SuccessionLaurice PocaisNoch keine Bewertungen
- Table of Legitimes - Testate and Intestate SuccessionDokument1 SeiteTable of Legitimes - Testate and Intestate SuccessionLaurice PocaisNoch keine Bewertungen
- Table of Legitimes - Table 1Dokument1 SeiteTable of Legitimes - Table 1MarkB15Noch keine Bewertungen
- United Nations Special Committee On Decolonization Self-Determination Gilbert and Ellice Islands Referendum Was Held in December 1974Dokument1 SeiteUnited Nations Special Committee On Decolonization Self-Determination Gilbert and Ellice Islands Referendum Was Held in December 1974MarkB15Noch keine Bewertungen
- SPL CasesDokument13 SeitenSPL CasesMarkB15Noch keine Bewertungen
- Labor Case #10Dokument40 SeitenLabor Case #10MarkB15100% (1)
- Origins of the People of TuvaluDokument1 SeiteOrigins of the People of TuvaluMarkB15Noch keine Bewertungen
- Be It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledDokument6 SeitenBe It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledMarkB15Noch keine Bewertungen
- Constitution of Tuvalu: Human Rights in TuvaluDokument1 SeiteConstitution of Tuvalu: Human Rights in TuvaluMarkB15Noch keine Bewertungen
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Tuvalu 4Dokument1 SeiteTuvalu 4MarkB15Noch keine Bewertungen
- United Nations Special Committee On Decolonization Self-Determination Gilbert and Ellice Islands Referendum Was Held in December 1974Dokument1 SeiteUnited Nations Special Committee On Decolonization Self-Determination Gilbert and Ellice Islands Referendum Was Held in December 1974MarkB15Noch keine Bewertungen
- Tuvalu 6Dokument1 SeiteTuvalu 6MarkB15Noch keine Bewertungen
- Tuvalu 5Dokument2 SeitenTuvalu 5MarkB15Noch keine Bewertungen
- Early Contacts With Other CulturesDokument2 SeitenEarly Contacts With Other CulturesMarkB15Noch keine Bewertungen
- 6th Central Pay Commission Salary CalculatorDokument15 Seiten6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Tuvalu: From Wikipedia, The Free Encyclopedia This Article Is About The Country. For Other Uses, See .Dokument3 SeitenTuvalu: From Wikipedia, The Free Encyclopedia This Article Is About The Country. For Other Uses, See .MarkB15Noch keine Bewertungen
- Martinique Economy OverviewDokument1 SeiteMartinique Economy OverviewMarkB15Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Therminol 55Dokument5 SeitenTherminol 55Dinesh KumarNoch keine Bewertungen
- The Role of Play Therapists in Children's Transitions: From Residential Care To Foster CareDokument11 SeitenThe Role of Play Therapists in Children's Transitions: From Residential Care To Foster Caresherry_hoang_1Noch keine Bewertungen
- Dar Breathing Filter Hme SellsheetDokument2 SeitenDar Breathing Filter Hme SellsheetmangkunegaraNoch keine Bewertungen
- Ups Installation Method StatementDokument197 SeitenUps Installation Method StatementehteshamNoch keine Bewertungen
- Training and Supervision of Health Care WorkersDokument12 SeitenTraining and Supervision of Health Care WorkerspriyankaNoch keine Bewertungen
- Khatr Khola ISP District RatesDokument56 SeitenKhatr Khola ISP District RatesCivil EngineeringNoch keine Bewertungen
- AnxietyDokument5 SeitenAnxietydrmadankumarbnysNoch keine Bewertungen
- Movie Ethics ReviewDokument4 SeitenMovie Ethics ReviewpearlydawnNoch keine Bewertungen
- Radiol 2020201473Dokument37 SeitenRadiol 2020201473M Victoria SalazarNoch keine Bewertungen
- WHO COVID-19 Situation Report - July 11Dokument16 SeitenWHO COVID-19 Situation Report - July 11CityNewsTorontoNoch keine Bewertungen
- Indian Boyhood PDFDokument316 SeitenIndian Boyhood PDFHasanNoch keine Bewertungen
- ASTM IndexDokument34 SeitenASTM IndexJimmy Chan67% (3)
- Capital Cost Mining PDFDokument263 SeitenCapital Cost Mining PDFsue1001Noch keine Bewertungen
- Otology Fellowships 2019Dokument5 SeitenOtology Fellowships 2019Sandra SandrinaNoch keine Bewertungen
- Earthing of GIS Type ELK - GTIDokument20 SeitenEarthing of GIS Type ELK - GTIJairo MoralesNoch keine Bewertungen
- Final TLE9 Nail Care9 Q1 Module 3Dokument20 SeitenFinal TLE9 Nail Care9 Q1 Module 3Ma. Andrea LagmanNoch keine Bewertungen
- 4 6051111060339957657Dokument361 Seiten4 6051111060339957657Oviedo OviedoNoch keine Bewertungen
- Seguridad Boltec Cable PDFDokument36 SeitenSeguridad Boltec Cable PDFCesar QuintanillaNoch keine Bewertungen
- Rundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967Dokument15 SeitenRundingan Perdagangan Antara Malaysia Dan Indonesia Di Wisma Putra, Kuala Lumpur 1967nixyingboNoch keine Bewertungen
- HBV Real Time PCR Primer Probe Sequncence PDFDokument9 SeitenHBV Real Time PCR Primer Probe Sequncence PDFnbiolab6659Noch keine Bewertungen
- Individualized Education PlanDokument7 SeitenIndividualized Education PlanElaine Aninang Hupeda100% (2)
- Honda PCX150Dokument137 SeitenHonda PCX150Akchu KadNoch keine Bewertungen
- 01 01Dokument232 Seiten01 01Muhammad Al-MshariNoch keine Bewertungen
- Evolution Chart 3Dokument1 SeiteEvolution Chart 3sasupraNoch keine Bewertungen
- MAPEH 2 SBC 2nd Quarterly AssesmentDokument5 SeitenMAPEH 2 SBC 2nd Quarterly AssesmentReshiele FalconNoch keine Bewertungen
- Refresher 2 (Pipe)Dokument12 SeitenRefresher 2 (Pipe)Kira YagamiNoch keine Bewertungen
- Bibie Evana OsmanDokument6 SeitenBibie Evana OsmanStabat Jaya TrademarkNoch keine Bewertungen
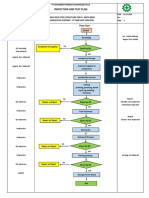
- Inspection and Test Plan: Flow Chart Start IncomingDokument1 SeiteInspection and Test Plan: Flow Chart Start IncomingSinden AyuNoch keine Bewertungen
- Regional Ecology Test ScoringDokument14 SeitenRegional Ecology Test Scoringaisyah Wardah201Noch keine Bewertungen
- The Truth About EtawahDokument4 SeitenThe Truth About EtawahPoojaDasgupta100% (1)