Das könnte Ihnen auch gefallen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- IsmsDokument1 SeiteIsmsJasonVasanthMSNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- နည္းပညာ စာအုပ္Dokument7 Seitenနည္းပညာ စာအုပ္Cur Io67% (3)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- Project Design Sign-Off FormDokument7 SeitenProject Design Sign-Off FormRicardo AngelNoch keine Bewertungen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Bus ID No.: M-2092: Passenger InformationDokument1 SeiteBus ID No.: M-2092: Passenger InformationJasonVasanthMSNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- MN AG v. SANOFI - 3:18-cv-14999 - Defendants' Joint Motion To Dismiss - 2019-08-12Dokument124 SeitenMN AG v. SANOFI - 3:18-cv-14999 - Defendants' Joint Motion To Dismiss - 2019-08-12The Type 1 Diabetes Defense FoundationNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Max 761 CsaDokument12 SeitenMax 761 CsabmhoangtmaNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Marketing ManagementDokument14 SeitenMarketing ManagementShaurya RathourNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- DSA NotesDokument87 SeitenDSA NotesAtefrachew SeyfuNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Asian Construction Dispute Denied ReviewDokument2 SeitenAsian Construction Dispute Denied ReviewJay jogs100% (2)
- Civil Aeronautics BoardDokument2 SeitenCivil Aeronautics BoardJayson AlvaNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Las Q1Dokument9 SeitenLas Q1Gaux SkjsjaNoch keine Bewertungen
- Ice Cream Cost Benefit AnalysisDokument12 SeitenIce Cream Cost Benefit AnalysischarlotteNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Geneva IntrotoBankDebt172Dokument66 SeitenGeneva IntrotoBankDebt172satishlad1288Noch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
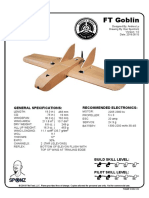
- FT Goblin Full SizeDokument7 SeitenFT Goblin Full SizeDeakon Frost100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Tata Group's Global Expansion and Business StrategiesDokument23 SeitenTata Group's Global Expansion and Business Strategiesvgl tamizhNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Discretionary Lending Power Updated Sep 2012Dokument28 SeitenDiscretionary Lending Power Updated Sep 2012akranjan888Noch keine Bewertungen
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- CFEExam Prep CourseDokument28 SeitenCFEExam Prep CourseM50% (4)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- Weka Tutorial 2Dokument50 SeitenWeka Tutorial 2Fikri FarisNoch keine Bewertungen
- Weibull Statistic and Growth Analysis in Failure PredictionsDokument9 SeitenWeibull Statistic and Growth Analysis in Failure PredictionsgmitsutaNoch keine Bewertungen
- Code Description DSMCDokument35 SeitenCode Description DSMCAnkit BansalNoch keine Bewertungen
- CCT AsqDokument12 SeitenCCT Asqlcando100% (1)
- 3) Stages of Group Development - To StudsDokument15 Seiten3) Stages of Group Development - To StudsDhannesh SweetAngelNoch keine Bewertungen
- Mapping Groundwater Recharge Potential Using GIS-Based Evidential Belief Function ModelDokument31 SeitenMapping Groundwater Recharge Potential Using GIS-Based Evidential Belief Function Modeljorge “the jordovo” davidNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Pyrometallurgical Refining of Copper in An Anode Furnace: January 2005Dokument13 SeitenPyrometallurgical Refining of Copper in An Anode Furnace: January 2005maxi roaNoch keine Bewertungen
- Single Wall Fuel Tank: FP 2.7 A-C Fire Pump SystemsDokument1 SeiteSingle Wall Fuel Tank: FP 2.7 A-C Fire Pump Systemsricardo cardosoNoch keine Bewertungen
- Improvements To Increase The Efficiency of The Alphazero Algorithm: A Case Study in The Game 'Connect 4'Dokument9 SeitenImprovements To Increase The Efficiency of The Alphazero Algorithm: A Case Study in The Game 'Connect 4'Lam Mai NgocNoch keine Bewertungen
- Bar Exam 2016 Suggested Answers in Political LawDokument15 SeitenBar Exam 2016 Suggested Answers in Political LawYlnne Cahlion KiwalanNoch keine Bewertungen
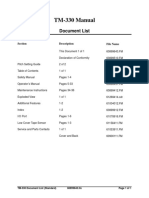
- PS300-TM-330 Owners Manual PDFDokument55 SeitenPS300-TM-330 Owners Manual PDFLester LouisNoch keine Bewertungen
- Lister LRM & SRM 1-2-3 Manual and Parts List - Lister - Canal WorldDokument4 SeitenLister LRM & SRM 1-2-3 Manual and Parts List - Lister - Canal Worldcountry boyNoch keine Bewertungen
- Craft's Folder StructureDokument2 SeitenCraft's Folder StructureWowNoch keine Bewertungen
- Unit 1 2marksDokument5 SeitenUnit 1 2marksLokesh SrmNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- 1990-1994 Electrical Wiring - DiagramsDokument13 Seiten1990-1994 Electrical Wiring - Diagramsal exNoch keine Bewertungen
- A320 Normal ProceduresDokument40 SeitenA320 Normal ProceduresRajesh KumarNoch keine Bewertungen
- Mini Ice Plant Design GuideDokument4 SeitenMini Ice Plant Design GuideDidy RobotIncorporatedNoch keine Bewertungen
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)