Das könnte Ihnen auch gefallen
- Penyakit Inf Saluran Pencernaan PDFDokument9 SeitenPenyakit Inf Saluran Pencernaan PDFAde PermanaNoch keine Bewertungen
- Daftar PustakaDokument3 SeitenDaftar PustakaJohn'sSujonoNoch keine Bewertungen
- Journal 3Dokument7 SeitenJournal 3AgustyaNoch keine Bewertungen
- Catatan Bedah 1Dokument18 SeitenCatatan Bedah 1John'sSujonoNoch keine Bewertungen
- Jurding Anestesi RSKHDokument16 SeitenJurding Anestesi RSKHJohn'sSujonoNoch keine Bewertungen
- Lehninger Intraksi Prot-LiganDokument34 SeitenLehninger Intraksi Prot-LiganJohn'sSujonoNoch keine Bewertungen
- Pic.1. Arteries and Veins of Pelvis MaleDokument3 SeitenPic.1. Arteries and Veins of Pelvis MaleJohn'sSujonoNoch keine Bewertungen
- Lateral Lingual Swellings and One Medial Swelling, The Tuberculum ImparDokument1 SeiteLateral Lingual Swellings and One Medial Swelling, The Tuberculum ImparIntan HaddadNoch keine Bewertungen
- Regulasi Ekspresi GenDokument41 SeitenRegulasi Ekspresi GenJohn'sSujonoNoch keine Bewertungen
- Recognising The Signs of A StrokeDokument4 SeitenRecognising The Signs of A StrokeJohn'sSujonoNoch keine Bewertungen
- Interaksi Protein LigandDokument7 SeitenInteraksi Protein LigandJohn'sSujonoNoch keine Bewertungen
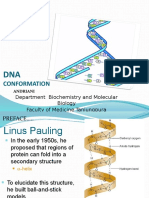
- Conformation: Department Biochemistry and Molecular Biology Faculty of Medicine Tanjungpura UniversityDokument31 SeitenConformation: Department Biochemistry and Molecular Biology Faculty of Medicine Tanjungpura UniversityJohn'sSujonoNoch keine Bewertungen
- Molecular Components of Cells: Nucleic AcidsDokument24 SeitenMolecular Components of Cells: Nucleic AcidsJohn'sSujonoNoch keine Bewertungen
- WHO Global Programme To Eliminate Lymphatic FilariasisDokument107 SeitenWHO Global Programme To Eliminate Lymphatic FilariasisVergaaBellanyNoch keine Bewertungen
- Lampiran: Gambar 1. Izin Ketua RWDokument3 SeitenLampiran: Gambar 1. Izin Ketua RWJohn'sSujonoNoch keine Bewertungen
- Antibiotics: Choices For Common InfectionsDokument30 SeitenAntibiotics: Choices For Common InfectionsAlfeus GradyNoch keine Bewertungen
- Pemicu 1 Hematologi Dan OnkologiDokument6 SeitenPemicu 1 Hematologi Dan OnkologiJohn'sSujonoNoch keine Bewertungen
- Sop Kel Immulite Bahasa InggDokument3 SeitenSop Kel Immulite Bahasa InggJohn'sSujonoNoch keine Bewertungen
- New New Proposal Mk. IIDokument10 SeitenNew New Proposal Mk. IIJohn'sSujonoNoch keine Bewertungen
- Pic.1. Arteries and Veins of Pelvis MaleDokument3 SeitenPic.1. Arteries and Veins of Pelvis MaleJohn'sSujonoNoch keine Bewertungen
- Pic.1. Arteries and Veins of Pelvis MaleDokument3 SeitenPic.1. Arteries and Veins of Pelvis MaleJohn'sSujonoNoch keine Bewertungen
- DR - Ita - Antihipertensi-Kv2014Dokument31 SeitenDR - Ita - Antihipertensi-Kv2014John'sSujonoNoch keine Bewertungen
- DR - Ita - Antihipertensi-Kv2014Dokument31 SeitenDR - Ita - Antihipertensi-Kv2014John'sSujonoNoch keine Bewertungen
- PhysioEx Ex 6 Activty 1-4Dokument6 SeitenPhysioEx Ex 6 Activty 1-4juwitavalenNoch keine Bewertungen
- SKEMA Poltekkes Games Asli FixDokument16 SeitenSKEMA Poltekkes Games Asli FixJohn'sSujonoNoch keine Bewertungen
- PhysioEx Ex 6 Activty 1-4Dokument6 SeitenPhysioEx Ex 6 Activty 1-4juwitavalenNoch keine Bewertungen
- Retinopati DiabetikDokument5 SeitenRetinopati DiabetikMuhammad Afriadi HamdanNoch keine Bewertungen
- Learnmares18 Hormther HCG Apr09Dokument2 SeitenLearnmares18 Hormther HCG Apr09John'sSujonoNoch keine Bewertungen
- Learnmares18 Hormther HCG Apr09Dokument2 SeitenLearnmares18 Hormther HCG Apr09John'sSujonoNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Amino Acidss & AminoacidopathiesDokument55 SeitenAmino Acidss & AminoacidopathiesMustafa KhandgawiNoch keine Bewertungen
- Bachelor of Surgery (MBBS)Dokument8 SeitenBachelor of Surgery (MBBS)Dinesh KumarNoch keine Bewertungen
- CA CardiovascularDokument10 SeitenCA CardiovascularNina OaipNoch keine Bewertungen
- (Revisi Plus Oke) Describe YourselfDokument3 Seiten(Revisi Plus Oke) Describe Yourselfchenth3r3Noch keine Bewertungen
- Inguinal HerniaDokument27 SeitenInguinal HerniaNeneng WulandariNoch keine Bewertungen
- Anorectal ClinicalDokument17 SeitenAnorectal ClinicalEster Sibarani100% (1)
- Anatomy of FistDokument4 SeitenAnatomy of FistCreative Flow Media100% (1)
- Pediatrics 2013 Kapadia E1488 96Dokument11 SeitenPediatrics 2013 Kapadia E1488 96M Aprial DarmawanNoch keine Bewertungen
- Annual CME Program ITBPDokument7 SeitenAnnual CME Program ITBPAnkit PrajapatiNoch keine Bewertungen
- MELANOMA: Risk Factors, Diagnosis, Staging and TreatmentDokument25 SeitenMELANOMA: Risk Factors, Diagnosis, Staging and TreatmentFazaKhilwanAmnaNoch keine Bewertungen
- Instructions for Ministry of Health Officials on Statement of Need LettersDokument1 SeiteInstructions for Ministry of Health Officials on Statement of Need LetterssurenvishvaNoch keine Bewertungen
- CSF Dynamics in Dandy-Walker Syndrome ExplainedDokument5 SeitenCSF Dynamics in Dandy-Walker Syndrome ExplainedSergio SaraivaNoch keine Bewertungen
- Emergency Department Anemia EvaluationDokument16 SeitenEmergency Department Anemia EvaluationJeffrey Stefan Pal RiveraNoch keine Bewertungen
- Dr. Sajid Sattar Butt - Consultant General Medicine FCPSDokument2 SeitenDr. Sajid Sattar Butt - Consultant General Medicine FCPScdeekyNoch keine Bewertungen
- Pharmacist's Letter: Prescriber's LetterDokument6 SeitenPharmacist's Letter: Prescriber's LetterJaved AkhtarNoch keine Bewertungen
- Dermatology For The Small Animal PractitionerDokument9 SeitenDermatology For The Small Animal PractitionerDenisa VescanNoch keine Bewertungen
- Mouth Breathing A Menace To Developing DentitionDokument7 SeitenMouth Breathing A Menace To Developing DentitionLia CucoranuNoch keine Bewertungen
- Infant Flow SiPAP - Operator's Manual EN (Rev.p) PDFDokument80 SeitenInfant Flow SiPAP - Operator's Manual EN (Rev.p) PDFPaul GennsonNoch keine Bewertungen
- Icrp 135Dokument144 SeitenIcrp 135Roshi_11Noch keine Bewertungen
- IlizarovDokument2 SeitenIlizarovsunshinehospitalNoch keine Bewertungen
- HH-II-163 ExercisesDokument3 SeitenHH-II-163 ExercisesGeorge AlbuNoch keine Bewertungen
- Jurnal ColonosDokument10 SeitenJurnal ColonosFuri Ainun KhikmahNoch keine Bewertungen
- Myresume 1Dokument3 SeitenMyresume 1MusadunDunNoch keine Bewertungen
- Peptic Duodenal Ulcer History, Causes, Symptoms and TreatmentDokument106 SeitenPeptic Duodenal Ulcer History, Causes, Symptoms and TreatmentCanan YilmazNoch keine Bewertungen
- Chintamani PHCDokument2 SeitenChintamani PHCSandeep GhosthNoch keine Bewertungen
- Motivation Letter Guideline Roy Bagus KurniawanDokument1 SeiteMotivation Letter Guideline Roy Bagus KurniawanRoy KurniawanNoch keine Bewertungen
- Minimum Standard Requirements For 100 AdmissionsDokument88 SeitenMinimum Standard Requirements For 100 AdmissionsKirthinath BallalNoch keine Bewertungen
- Nelson Roy MCT PDFDokument42 SeitenNelson Roy MCT PDFMonica Djaja SaputeraNoch keine Bewertungen
- Pediatric Clinical ExaminationDokument3 SeitenPediatric Clinical ExaminationAlexander EnnesNoch keine Bewertungen
- Bhabha ReprtDokument126 SeitenBhabha ReprtRinky MansukhaniNoch keine Bewertungen