Das könnte Ihnen auch gefallen
- Investor Account Opening Form For Individual: Day Month YearDokument4 SeitenInvestor Account Opening Form For Individual: Day Month YearEngr. Nadeem AhmadNoch keine Bewertungen
- Investor Account Opening Form For Individual: Day Month YearDokument9 SeitenInvestor Account Opening Form For Individual: Day Month YearTahir KhattakNoch keine Bewertungen
- Account Opening FormDokument22 SeitenAccount Opening FormTarun BhardwajNoch keine Bewertungen
- Auto Debit Instruction For Nach/Dd: Cc/Branchops/Mandate Form/002Dokument2 SeitenAuto Debit Instruction For Nach/Dd: Cc/Branchops/Mandate Form/002Dhruv SekhriNoch keine Bewertungen
- BOC Account Opening FormDokument2 SeitenBOC Account Opening FormCyberpoint Internet Cafe and Computer ShopNoch keine Bewertungen
- Form VendorDokument4 SeitenForm VendorEko HarnoNoch keine Bewertungen
- Unbranded Annuity Quote Request FormDokument2 SeitenUnbranded Annuity Quote Request FormKevin OttoNoch keine Bewertungen
- Term Deposit FormDokument2 SeitenTerm Deposit FormVishnu VNoch keine Bewertungen
- Bis - Co MakerDokument4 SeitenBis - Co MakerDee ReyesNoch keine Bewertungen
- Fixed Deposit FormDokument2 SeitenFixed Deposit FormNikita JainNoch keine Bewertungen
- JM Finance MF - Sip NachDokument1 SeiteJM Finance MF - Sip NacharunimaapkNoch keine Bewertungen
- Updated Non-Individual Application Form-Updated - FillableDokument2 SeitenUpdated Non-Individual Application Form-Updated - FillableHang VeasnaNoch keine Bewertungen
- 2 Compliance Questionnaire STANDARDDokument3 Seiten2 Compliance Questionnaire STANDARDchung elaineNoch keine Bewertungen
- Account Opening - CorporateDokument8 SeitenAccount Opening - CorporateSyed Mohsin SheraziNoch keine Bewertungen
- Banking Account Opening FormDokument12 SeitenBanking Account Opening FormCassiane OgliariNoch keine Bewertungen
- WEL TB PAY002 Account Activation Form PDFDokument1 SeiteWEL TB PAY002 Account Activation Form PDFAnonymous Z6ve7AqWKNoch keine Bewertungen
- Service-Request-Form DBS BankDokument3 SeitenService-Request-Form DBS BanketishreddyNoch keine Bewertungen
- CIMB Application FormDokument10 SeitenCIMB Application Formanie zuNoch keine Bewertungen
- VISA Corporate Card Application Form Clarien EDT Feb1120Dokument4 SeitenVISA Corporate Card Application Form Clarien EDT Feb1120Mihai ConstantinescuNoch keine Bewertungen
- युनाइटेड बक ऑफ इंडया United Bank of India: United Demat Account Opening FormDokument12 Seitenयुनाइटेड बक ऑफ इंडया United Bank of India: United Demat Account Opening Formjay meskaNoch keine Bewertungen
- Common Transaction Form Financial Transaction Kk3i5z51Dokument8 SeitenCommon Transaction Form Financial Transaction Kk3i5z51Balraj SinghNoch keine Bewertungen
- Standing Order Form For Saving PlanDokument1 SeiteStanding Order Form For Saving PlanSalman ArshadNoch keine Bewertungen
- Loan Application Form 1. Applicant'S Personal InformationDokument2 SeitenLoan Application Form 1. Applicant'S Personal InformationWingadianLeviOsa100% (5)
- Bosa Loan Application FormDokument2 SeitenBosa Loan Application Formal lakwena100% (1)
- SIP DebitMandateNACH-FormDokument2 SeitenSIP DebitMandateNACH-FormDevesh SinghNoch keine Bewertungen
- Fixed Deposit FormDokument2 SeitenFixed Deposit FormNikita JainNoch keine Bewertungen
- Automatic Investment Form: Asset ManagementDokument2 SeitenAutomatic Investment Form: Asset ManagementFreelancer SukanthoNoch keine Bewertungen
- Registration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachDokument2 SeitenRegistration Form Cum Mandate For Electronic Clearing Services (Ecs) /direct Debit/NachG.R.AzhaguvelSaranya Professor MechanicalNoch keine Bewertungen
- Personal - Ac - App - Form - V 2 - 29 - Nov2013Dokument3 SeitenPersonal - Ac - App - Form - V 2 - 29 - Nov2013nzekwesiliekenedilichukwuNoch keine Bewertungen
- 05 Circular - ForM 9 - Account Opening Form (Individual)Dokument4 Seiten05 Circular - ForM 9 - Account Opening Form (Individual)Sneha bagweNoch keine Bewertungen
- NT Opening NT Openingf: H.G Markets (PVT) Limited H.G Markets (PVT) Limited H.G Markets (PVT) LimitedDokument11 SeitenNT Opening NT Openingf: H.G Markets (PVT) Limited H.G Markets (PVT) Limited H.G Markets (PVT) LimitedMuhammad Azhar SaleemNoch keine Bewertungen
- Tata Eqty Jul14 PDFDokument4 SeitenTata Eqty Jul14 PDFsridharreddy14Noch keine Bewertungen
- Account Opening Form: Million MillionDokument1 SeiteAccount Opening Form: Million Millionsales 1Noch keine Bewertungen
- General Standing Instruction Order Payment PDFDokument3 SeitenGeneral Standing Instruction Order Payment PDFmiriam chewNoch keine Bewertungen
- App Nri 15-01-08Dokument4 SeitenApp Nri 15-01-08sarvathaqaryNoch keine Bewertungen
- Tradovate Individual Account ApplicationDokument6 SeitenTradovate Individual Account ApplicationAbdelazeem GawadNoch keine Bewertungen
- Corporate Account Opening FormDokument20 SeitenCorporate Account Opening FormEmmanuel Deeds-AshinzeNoch keine Bewertungen
- Zerodha Account OpeningDokument8 SeitenZerodha Account OpeningDeerajKumarNoch keine Bewertungen
- Common Application AxisDokument5 SeitenCommon Application AxisCubicle CoderNoch keine Bewertungen
- FSM ETF and Stock Transfer in Form20161007Dokument1 SeiteFSM ETF and Stock Transfer in Form20161007Isabel ImNoch keine Bewertungen
- Premature Withdrawal Form - 102Dokument8 SeitenPremature Withdrawal Form - 102sher singhNoch keine Bewertungen
- 3 - CamDokument3 Seiten3 - CamKavit Thakkar100% (1)
- Form 83Dokument5 SeitenForm 83Vivek Maheswari100% (1)
- WBG Form Account Opening BusinessDokument4 SeitenWBG Form Account Opening BusinessutlublyegNoch keine Bewertungen
- Hekima Plan Application Form-EDokument4 SeitenHekima Plan Application Form-ExeniaNoch keine Bewertungen
- Tamil Nadu Power Finance and Infrastructure Development Corporation LimitedDokument12 SeitenTamil Nadu Power Finance and Infrastructure Development Corporation Limitedtechnical100% (1)
- Empanelment Form New Mirae AssetDokument4 SeitenEmpanelment Form New Mirae AssetSachin KumarNoch keine Bewertungen
- Account Opening FormDokument23 SeitenAccount Opening Formabhishek shawNoch keine Bewertungen
- CIC Individual Application FormDokument4 SeitenCIC Individual Application FormmarcusNoch keine Bewertungen
- Retirement Notification FormDokument2 SeitenRetirement Notification FormAbongile PhinyanaNoch keine Bewertungen
- It Declaration Form 2010 11Dokument3 SeitenIt Declaration Form 2010 11maiudayNoch keine Bewertungen
- Fixed/Recurring Deposit: Type of AccountDokument4 SeitenFixed/Recurring Deposit: Type of AccountHarpreet0gjgkbkv KaurNoch keine Bewertungen
- Fixed Deposit Account Opening Form For Existing CustomersDokument4 SeitenFixed Deposit Account Opening Form For Existing Customershero romeoNoch keine Bewertungen
- Kina AccountDokument6 SeitenKina AccountNathan LakaNoch keine Bewertungen
- Vendor Master FormDokument2 SeitenVendor Master Formrekha0% (1)
- Kina Bank Personal Account Opening FormDokument7 SeitenKina Bank Personal Account Opening FormJohn Yala100% (3)
- The Handbook of Credit Risk Management: Originating, Assessing, and Managing Credit ExposuresVon EverandThe Handbook of Credit Risk Management: Originating, Assessing, and Managing Credit ExposuresNoch keine Bewertungen
- SECURITIES INDUSTRY ESSENTIALS EXAM STUDY GUIDE 2021 + TEST BANKVon EverandSECURITIES INDUSTRY ESSENTIALS EXAM STUDY GUIDE 2021 + TEST BANKBewertung: 5 von 5 Sternen5/5 (1)
- Exam Facts Series 52 Municipal Securities Representative Exam Study GuideVon EverandExam Facts Series 52 Municipal Securities Representative Exam Study GuideBewertung: 1.5 von 5 Sternen1.5/5 (2)
- Foreign Exchange Rate Sheet: 129 Sheet No Date 17-Jul-19Dokument1 SeiteForeign Exchange Rate Sheet: 129 Sheet No Date 17-Jul-19Salman ArshadNoch keine Bewertungen
- RemittanceMBL 17JUL PDFDokument1 SeiteRemittanceMBL 17JUL PDFSalman ArshadNoch keine Bewertungen
- FX MBL 30octDokument1 SeiteFX MBL 30octSalman ArshadNoch keine Bewertungen
- Currency Buying: Treasury DepartmentDokument1 SeiteCurrency Buying: Treasury DepartmentSalman ArshadNoch keine Bewertungen
- FX MBL 29octDokument1 SeiteFX MBL 29octSalman ArshadNoch keine Bewertungen
- FXNOV13Dokument1 SeiteFXNOV13Salman ArshadNoch keine Bewertungen
- RemittanceMBL 11DECDokument1 SeiteRemittanceMBL 11DECSalman ArshadNoch keine Bewertungen
- RemittanceMBL 29OCTDokument1 SeiteRemittanceMBL 29OCTSalman ArshadNoch keine Bewertungen
- RemittanceMBL 30OCTDokument1 SeiteRemittanceMBL 30OCTSalman ArshadNoch keine Bewertungen
- RMBL13NOVDokument1 SeiteRMBL13NOVSalman ArshadNoch keine Bewertungen
- CTA Case EB For ReferenceDokument29 SeitenCTA Case EB For Referencepatricia_arpilledaNoch keine Bewertungen
- Module 07.5 - Foreign Currency Accounting PSDokument5 SeitenModule 07.5 - Foreign Currency Accounting PSFiona Morales100% (2)
- SEAT Ibiza Range BrochureDokument25 SeitenSEAT Ibiza Range BrochureJason SmithNoch keine Bewertungen
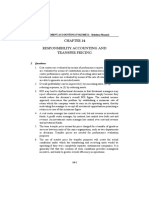
- Chapter 14Dokument18 SeitenChapter 14RenNoch keine Bewertungen
- AppendicesDokument8 SeitenAppendicescrackheads philippinesNoch keine Bewertungen
- Bsda FormDokument1 SeiteBsda FormGayathriSureshNoch keine Bewertungen
- CFA Preparation COURSE 2021: Organized by Cfa Society PolandDokument4 SeitenCFA Preparation COURSE 2021: Organized by Cfa Society PolandJua perezNoch keine Bewertungen
- FOMB - Letter - Senate of Puerto Rico - Response Letter Section 204 (A) (6) SB 1304 - February 7, 2024Dokument3 SeitenFOMB - Letter - Senate of Puerto Rico - Response Letter Section 204 (A) (6) SB 1304 - February 7, 2024Metro Puerto RicoNoch keine Bewertungen
- HDFC Top 100 Fund - Patience Pays!Dokument4 SeitenHDFC Top 100 Fund - Patience Pays!Manju Bhashini M RNoch keine Bewertungen
- Greek CrisisDokument3 SeitenGreek CrisisΕυα ΕυαNoch keine Bewertungen
- Quiz 3Dokument4 SeitenQuiz 3ErionNoch keine Bewertungen
- Capital Budgeting 2Dokument4 SeitenCapital Budgeting 2Nicole Daphne FigueroaNoch keine Bewertungen
- DU M.Com Information Brochure 2015Dokument14 SeitenDU M.Com Information Brochure 2015Neepur GargNoch keine Bewertungen
- Muthoot Finance LTD 110912Dokument3 SeitenMuthoot Finance LTD 110912Kannan SundaresanNoch keine Bewertungen
- TLMDokument32 SeitenTLMsampada_shekharNoch keine Bewertungen
- University of Kota - Kota: Day Date Time Subject PaperDokument3 SeitenUniversity of Kota - Kota: Day Date Time Subject PaperDinesh LalwaniNoch keine Bewertungen
- DP Classes CA Final IDT May 2021 Module 3Dokument235 SeitenDP Classes CA Final IDT May 2021 Module 3Sathwika DevarapalliNoch keine Bewertungen
- Sachin Tyagi Insurance PDFDokument4 SeitenSachin Tyagi Insurance PDFsachin tyagiNoch keine Bewertungen
- FIN448-Final-Exam-Fall2020-Review - MCDokument85 SeitenFIN448-Final-Exam-Fall2020-Review - MCMay ChenNoch keine Bewertungen
- On Consumer Perspective Towards Various Investment Sectors in The Leading SolutionDokument26 SeitenOn Consumer Perspective Towards Various Investment Sectors in The Leading SolutionAbhishek Choudhary89% (9)
- FinalDokument31 SeitenFinalAniruddha RantuNoch keine Bewertungen
- ASE20091 Bank Recon - 2017-04 - P53212A0120Dokument2 SeitenASE20091 Bank Recon - 2017-04 - P53212A0120Thooi Joo Wong0% (1)
- Marketing Strategies For Mortgage Lenders and BrokersDokument2 SeitenMarketing Strategies For Mortgage Lenders and BrokersTodd Lake100% (7)
- Internship Report On Financial PerformanDokument70 SeitenInternship Report On Financial PerformanPik PokNoch keine Bewertungen
- PWT 90Dokument1.315 SeitenPWT 90burcakkaplanNoch keine Bewertungen
- AnDokument5 SeitenAnPritesh ChaudhariNoch keine Bewertungen
- 6 MNTH STMNTDokument22 Seiten6 MNTH STMNTVikrant VermaNoch keine Bewertungen
- Mariel Princess TabilangonDokument2 SeitenMariel Princess TabilangonMariel PrincessNoch keine Bewertungen
- FIN2012 Ovigele 10effectivetips ExcerptDokument19 SeitenFIN2012 Ovigele 10effectivetips ExcerptOng OngNoch keine Bewertungen
- Warren Buffett 1985Dokument7 SeitenWarren Buffett 1985anil1820Noch keine Bewertungen