Das könnte Ihnen auch gefallen
- JClinOphthalmolRes43123-8318319 021838Dokument4 SeitenJClinOphthalmolRes43123-8318319 021838Dex Bayu AcNoch keine Bewertungen
- GlaucomaDokument37 SeitenGlaucomaxuelun1Noch keine Bewertungen
- Migraine As A Risk Factor For Primary Open Angle Glaucoma A Systematic Review and Meta-AnalysisDokument8 SeitenMigraine As A Risk Factor For Primary Open Angle Glaucoma A Systematic Review and Meta-AnalysisEsteven Tanu GunawanNoch keine Bewertungen
- Trends in Corneal TopographyDokument7 SeitenTrends in Corneal TopographygustavoecardosoNoch keine Bewertungen
- Practical Gynecologic Pathology: Frequently Asked QuestionsVon EverandPractical Gynecologic Pathology: Frequently Asked QuestionsJian-Jun WeiNoch keine Bewertungen
- Janetos TM, Volpe NJ, and Simon SS. "Neuro-Ophthalmic Manifestations of Cancer - A Narrative Review." 2022 11 (3) - 25Dokument19 SeitenJanetos TM, Volpe NJ, and Simon SS. "Neuro-Ophthalmic Manifestations of Cancer - A Narrative Review." 2022 11 (3) - 25MarisyaNoch keine Bewertungen
- Alamanos 2016Dokument12 SeitenAlamanos 2016dana40018256Noch keine Bewertungen
- Artificial Intelligence in Early Diagnosis and Prevention of Oral CancerDokument6 SeitenArtificial Intelligence in Early Diagnosis and Prevention of Oral CancerAdam ArnandyNoch keine Bewertungen
- Outcome Prediction in CancerVon EverandOutcome Prediction in CancerAzzam F.G. TaktakNoch keine Bewertungen
- Diagnostics 12 01664 v2Dokument23 SeitenDiagnostics 12 01664 v2asim zamanNoch keine Bewertungen
- Artigo 2 - MestradoDokument6 SeitenArtigo 2 - MestradoThiago RodriguesNoch keine Bewertungen
- Choroidal NeovascularizationVon EverandChoroidal NeovascularizationJay ChhablaniNoch keine Bewertungen
- Jurnal Glaukoma2Dokument7 SeitenJurnal Glaukoma2faruq azmiNoch keine Bewertungen
- 5fu KeratocystDokument9 Seiten5fu Keratocystdanielnobre47570Noch keine Bewertungen
- Jackson2016 PDFDokument10 SeitenJackson2016 PDFResearch Assistant of Dr. Rizal HamidNoch keine Bewertungen
- Fenotipos Clínicos y de Neuroimagen de La Astrocitopatía de Proteína Ácida Fibrilar Glial Autoinmune Una Revisión Sistemática y Un MetanálisisDokument16 SeitenFenotipos Clínicos y de Neuroimagen de La Astrocitopatía de Proteína Ácida Fibrilar Glial Autoinmune Una Revisión Sistemática y Un MetanálisisOlga Manco GuzmánNoch keine Bewertungen
- PIIS0002939422003774Dokument10 SeitenPIIS0002939422003774Anca Florina GaceaNoch keine Bewertungen
- Progress in Retinal and Eye Research-Optic Neuropathy in High Myopia - Glaucoma or High Myopia or BothDokument60 SeitenProgress in Retinal and Eye Research-Optic Neuropathy in High Myopia - Glaucoma or High Myopia or Both钟华Noch keine Bewertungen
- Medi 96 E5864Dokument6 SeitenMedi 96 E5864mono1144Noch keine Bewertungen
- Independent Risk Factors of Acute Kidney Injury Among Patients Receiving Extracorporeal Membrane OxygenationDokument8 SeitenIndependent Risk Factors of Acute Kidney Injury Among Patients Receiving Extracorporeal Membrane OxygenationFreddy Shanner Chávez VásquezNoch keine Bewertungen
- Fragasso2018 AKI TRRDokument14 SeitenFragasso2018 AKI TRRLeydi johana Rodriguez alzateNoch keine Bewertungen
- Three-Year Incidence and Factors Associated With Posterior Capsule OpacificationDokument1 SeiteThree-Year Incidence and Factors Associated With Posterior Capsule OpacificationMuhammad HasbiNoch keine Bewertungen
- Prognostic Tools For ....Dokument15 SeitenPrognostic Tools For ....I'am AjhaNoch keine Bewertungen
- Clinical Characteristics and Surgical Safety in Congenital Cataract Eyes With Three Pathological Types of Posterior Capsule AbnormalitiesDokument9 SeitenClinical Characteristics and Surgical Safety in Congenital Cataract Eyes With Three Pathological Types of Posterior Capsule Abnormalitiesaristo callenNoch keine Bewertungen
- Systematic Review and Meta-Analysis of The Efficacy and Safety of Immunosuppressive Pulse Therapy in The Treatment of Paraquat PoisoningDokument10 SeitenSystematic Review and Meta-Analysis of The Efficacy and Safety of Immunosuppressive Pulse Therapy in The Treatment of Paraquat PoisoningRICHARNoch keine Bewertungen
- Clinical Characteristics and Surgical Outcomes in Patients With Intermittent ExotropiaDokument6 SeitenClinical Characteristics and Surgical Outcomes in Patients With Intermittent ExotropiaIkmal ShahromNoch keine Bewertungen
- Termaat 2005Dokument11 SeitenTermaat 2005OkyôAmêliâNoch keine Bewertungen
- Xi, 2021 Tumor Associated Collagen SignaturesDokument15 SeitenXi, 2021 Tumor Associated Collagen Signaturesevahendrickx03Noch keine Bewertungen
- Comparison of Canaloplasty and Trabeculectomy For Open Angle Glaucoma: A Meta-AnalysisDokument6 SeitenComparison of Canaloplasty and Trabeculectomy For Open Angle Glaucoma: A Meta-AnalysisGesti Pratiwi HerlambangNoch keine Bewertungen
- Practical Lymph Node and Bone Marrow Pathology: Frequently Asked QuestionsVon EverandPractical Lymph Node and Bone Marrow Pathology: Frequently Asked QuestionsEndi WangNoch keine Bewertungen
- 1 ArticuloDokument14 Seiten1 ArticuloAlv JDNoch keine Bewertungen
- 1 s2.0 S1876034117301818 Main PDFDokument5 Seiten1 s2.0 S1876034117301818 Main PDFdiyanNoch keine Bewertungen
- Diagnostic Value of Cerebrospinal Fluid Lactate For Post-NeurosurgicalDokument9 SeitenDiagnostic Value of Cerebrospinal Fluid Lactate For Post-Neurosurgicalmariafernandasv98Noch keine Bewertungen
- FCVM 09 1022658Dokument20 SeitenFCVM 09 1022658francogarciaramirez1Noch keine Bewertungen
- Direct Oral Anticoagulants in Treatment of Cerebral Venous Thrombosis: A Systematic Review ProtocolDokument4 SeitenDirect Oral Anticoagulants in Treatment of Cerebral Venous Thrombosis: A Systematic Review Protocolrachman puteraNoch keine Bewertungen
- 2021 - Wu OphthalmologyRetina PreprintDokument17 Seiten2021 - Wu OphthalmologyRetina PreprintMARSELLA MICHELLE ERIKA SUMANGKUTNoch keine Bewertungen
- Epidemiology and Clinical Characteristics of Patients With Glaucoma: An Analysis of Hospital Data Between 2003 and 2012 Original ArticleDokument7 SeitenEpidemiology and Clinical Characteristics of Patients With Glaucoma: An Analysis of Hospital Data Between 2003 and 2012 Original Articlesyntacs skNoch keine Bewertungen
- Jurnal SuciDokument10 SeitenJurnal Sucinaufal12345Noch keine Bewertungen
- JAMDIG StudyDokument9 SeitenJAMDIG StudyTushar BatraNoch keine Bewertungen
- Journal Pone 0247330Dokument14 SeitenJournal Pone 0247330viju001Noch keine Bewertungen
- Platelet To Lymphocyte Ratio As A Potential.27Dokument8 SeitenPlatelet To Lymphocyte Ratio As A Potential.27Yohana Elisabeth GultomNoch keine Bewertungen
- Ischemic Cerebrovascular Accident and Its Secondary Renal ImpairmentDokument5 SeitenIschemic Cerebrovascular Accident and Its Secondary Renal ImpairmentAditya Angela AdamNoch keine Bewertungen
- Glioma Imaging: Physiologic, Metabolic, and Molecular ApproachesVon EverandGlioma Imaging: Physiologic, Metabolic, and Molecular ApproachesWhitney B. PopeNoch keine Bewertungen
- [19330715 - Journal of Neurosurgery_ Pediatrics] Comparative effectiveness of flexible versus rigid neuroendoscopy for endoscopic third ventriculostomy and choroid plexus cauterization_ a propensity score–matchedDokument7 Seiten[19330715 - Journal of Neurosurgery_ Pediatrics] Comparative effectiveness of flexible versus rigid neuroendoscopy for endoscopic third ventriculostomy and choroid plexus cauterization_ a propensity score–matchedBruno MañonNoch keine Bewertungen
- 2021 Efficacy, Safety and Complications of Autologous Fat Grafting To The Eyelids and Periorbital Area A Systematic Review and Meta-AnalysisDokument18 Seiten2021 Efficacy, Safety and Complications of Autologous Fat Grafting To The Eyelids and Periorbital Area A Systematic Review and Meta-AnalysisDimitris RodriguezNoch keine Bewertungen
- Practical Oncologic Molecular Pathology: Frequently Asked QuestionsVon EverandPractical Oncologic Molecular Pathology: Frequently Asked QuestionsNoch keine Bewertungen
- Pressure Fluctuations in GlaucomaDokument6 SeitenPressure Fluctuations in GlaucomaTushar BatraNoch keine Bewertungen
- Impact of Stem Cells-Based TherapyDokument7 SeitenImpact of Stem Cells-Based TherapyIvaylo RangelovNoch keine Bewertungen
- Acta Ophthalmologica - 2015 - Wong - Central Serous Chorioretinopathy What We Have Learnt So FarDokument5 SeitenActa Ophthalmologica - 2015 - Wong - Central Serous Chorioretinopathy What We Have Learnt So FarSalsa BillaNoch keine Bewertungen
- The Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-AnalysisDokument7 SeitenThe Impact of Sealer Extrusion On Endodontic Outcome: A Systematic Review With Meta-Analysisitsme543210Noch keine Bewertungen
- NIH Public Access: Author ManuscriptDokument23 SeitenNIH Public Access: Author ManuscriptIntan Kartika NursyahbaniNoch keine Bewertungen
- Translational Research in Breast CancerVon EverandTranslational Research in Breast CancerDong-Young NohNoch keine Bewertungen
- Brolucizumab EstudioDokument13 SeitenBrolucizumab EstudioJuan Carlos Mejía SernaNoch keine Bewertungen
- Critical Pathway For Primary Open Angle Glaucoma DiagnosisDokument5 SeitenCritical Pathway For Primary Open Angle Glaucoma DiagnosisSadhira GitaNoch keine Bewertungen
- Validation of An Objective Keratoconus Detection System Implemented in A Scheimpflug Tomographer and Comparison With Other MethodsDokument7 SeitenValidation of An Objective Keratoconus Detection System Implemented in A Scheimpflug Tomographer and Comparison With Other Methodstai daisyNoch keine Bewertungen
- Fisiopatología de La Cirrosis HepáticaDokument12 SeitenFisiopatología de La Cirrosis HepáticaysauraNoch keine Bewertungen
- Complications Secondary To Nonsurgical Rhinoplasty A Systematic Review and Meta-Analysis - de Victor, 2021Dokument6 SeitenComplications Secondary To Nonsurgical Rhinoplasty A Systematic Review and Meta-Analysis - de Victor, 2021Rafael Autran Cavalcante AraújoNoch keine Bewertungen
- 1 s2.0 S0039625720300709 MainDokument23 Seiten1 s2.0 S0039625720300709 Mainneha midhaNoch keine Bewertungen
- Assignment 3 - 2 Microcontrollers With DatasheetsDokument2 SeitenAssignment 3 - 2 Microcontrollers With Datasheetsapi-42328551276% (45)
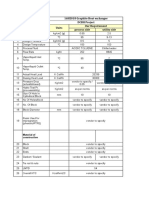
- 16HE018 Graphite Heat Exchanger DCBH Project Sr. No. Particulars Units Our Requirement Process Side Utility SideDokument2 Seiten16HE018 Graphite Heat Exchanger DCBH Project Sr. No. Particulars Units Our Requirement Process Side Utility SideBhaumik BhuvaNoch keine Bewertungen
- Technology Architecture For NginX, postgreSQL, postgRESTDokument5 SeitenTechnology Architecture For NginX, postgreSQL, postgRESTkarelvdwalt9366Noch keine Bewertungen
- Casting Fabrication of Carbon Steel Pitman For Crusher Suppliers and Manufacturers China - Professional Factory - Zhengda HDokument1 SeiteCasting Fabrication of Carbon Steel Pitman For Crusher Suppliers and Manufacturers China - Professional Factory - Zhengda HCarlos Ediver Arias RestrepoNoch keine Bewertungen
- Session 2A JonkerDokument15 SeitenSession 2A JonkerD_D_ANoch keine Bewertungen
- TIBCO Hawk Rulebase Standard GuidelinesDokument9 SeitenTIBCO Hawk Rulebase Standard GuidelinesAshish ShrivastavaNoch keine Bewertungen
- Surface Finish StandardDokument3 SeitenSurface Finish StandardvinodmysoreNoch keine Bewertungen
- MagnetostictiveDokument17 SeitenMagnetostictivekanikasharma22Noch keine Bewertungen
- Manual Udian AL 7021Dokument6 SeitenManual Udian AL 7021Vasudha SharmaNoch keine Bewertungen
- 4 Ataxle PDFDokument22 Seiten4 Ataxle PDFAnonymous XTkln6H100% (1)
- Sabor CaseDokument3 SeitenSabor CaseTushar LaroiyaNoch keine Bewertungen
- Invoice Cod Invoice Cod: Agen Pos Agen PosDokument4 SeitenInvoice Cod Invoice Cod: Agen Pos Agen Poswahids0204Noch keine Bewertungen
- Section: Engine MechanicalDokument76 SeitenSection: Engine MechanicalcesarNoch keine Bewertungen
- Ic 1403 2 MarksDokument14 SeitenIc 1403 2 MarksJeya Prakash100% (2)
- SMB4004 Topic 3Dokument34 SeitenSMB4004 Topic 3Norainah Abdul GaniNoch keine Bewertungen
- SB658Dokument3 SeitenSB658ricardo novoa saraviaNoch keine Bewertungen
- Wireless NetworkingDokument200 SeitenWireless NetworkingVamsikrishna PanugantiNoch keine Bewertungen
- Esna CatalogDokument12 SeitenEsna Catalogbalaji_jayadeva9546Noch keine Bewertungen
- HTTP StreamsDokument8 SeitenHTTP StreamsMarcelo Castro MartinoNoch keine Bewertungen
- Introduction To Boltzmann LearningDokument2 SeitenIntroduction To Boltzmann LearningnvbondNoch keine Bewertungen
- A-Class Mark II: Print Engines For ApplicatorsDokument25 SeitenA-Class Mark II: Print Engines For ApplicatorsJeffery ReynoldsNoch keine Bewertungen
- Government Polytechnic Muzaffarpur: Name of The Lab: Power Electronics & DrivesDokument18 SeitenGovernment Polytechnic Muzaffarpur: Name of The Lab: Power Electronics & DrivesVK DNoch keine Bewertungen
- LS-VINA EHV Cable's CatalogueDokument36 SeitenLS-VINA EHV Cable's CatalogueDjar Ndoeth0% (1)
- Factors Affecting Beam StrengthDokument2 SeitenFactors Affecting Beam StrengthkalpanaadhiNoch keine Bewertungen
- Plasma TV SMPS TroubleshoutingDokument5 SeitenPlasma TV SMPS TroubleshoutingmindjokerNoch keine Bewertungen
- Mac Puarsa MRL SCHEMATICDokument28 SeitenMac Puarsa MRL SCHEMATICthanggimme.phanNoch keine Bewertungen
- B. Tech. Electrical and Electronics EngineeringDokument105 SeitenB. Tech. Electrical and Electronics EngineeringKarthik NagarajanNoch keine Bewertungen
- Performance Analysis of Cooperative Communication For Wireless NetworksDokument164 SeitenPerformance Analysis of Cooperative Communication For Wireless NetworksIhtesham JadoonNoch keine Bewertungen
- QCDD-Duyar-QR SprinklersDokument2 SeitenQCDD-Duyar-QR SprinklersBaraa' KahlawiNoch keine Bewertungen
- Links Deep WebDokument2 SeitenLinks Deep WebArnoldTorresNoch keine Bewertungen













































![[19330715 - Journal of Neurosurgery_ Pediatrics] Comparative effectiveness of flexible versus rigid neuroendoscopy for endoscopic third ventriculostomy and choroid plexus cauterization_ a propensity score–matched](https://imgv2-1-f.scribdassets.com/img/document/722525723/149x198/0c84be9862/1712965550?v=1)