Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Midwives' Role in Empowering Women to Support SDGsDokument6 SeitenMidwives' Role in Empowering Women to Support SDGsMita RiskaNoch keine Bewertungen
- Sexually Transmitted Disesase.: Ralph Gabriel QuinalDokument16 SeitenSexually Transmitted Disesase.: Ralph Gabriel QuinalJohn Michael MonteflacoNoch keine Bewertungen
- Hiv & Aids Awareness ProgramDokument8 SeitenHiv & Aids Awareness ProgramKenzie WalshNoch keine Bewertungen
- Maternal and Child NCLEX QuestionsDokument3 SeitenMaternal and Child NCLEX QuestionsShengxy Ferrer100% (1)
- MisoprostolDokument6 SeitenMisoprostolMitchel Córdova LoaizaNoch keine Bewertungen
- PIDDokument11 SeitenPIDManjuNoch keine Bewertungen
- Print - Ectopic Pregnancy - 10min TalkDokument2 SeitenPrint - Ectopic Pregnancy - 10min TalknicdeepNoch keine Bewertungen
- Ovulation CalanderDokument2 SeitenOvulation CalanderBN NGNoch keine Bewertungen
- Sexual Behavior Buffalo BullsDokument2 SeitenSexual Behavior Buffalo BullsGovind Narayan PurohitNoch keine Bewertungen
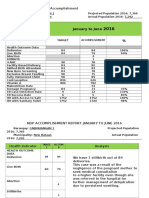
- CABINUANGAN 1 Health Indicators Report Shows Success in Maternal and Child OutcomesDokument4 SeitenCABINUANGAN 1 Health Indicators Report Shows Success in Maternal and Child OutcomesRonald A. SagangNoch keine Bewertungen
- Fiqh 20 - The Chapter of Major Bath (Ghusl)Dokument7 SeitenFiqh 20 - The Chapter of Major Bath (Ghusl)Noor-uz-Zamaan AcademyNoch keine Bewertungen
- Banned WordsDokument10 SeitenBanned Wordsnelu49Noch keine Bewertungen
- Post Abortion Care (Pac)Dokument9 SeitenPost Abortion Care (Pac)Ekiran BabajideNoch keine Bewertungen
- Young Talk, February 2009Dokument4 SeitenYoung Talk, February 2009Straight Talk FoundationNoch keine Bewertungen
- Biology Study Material Final2012 13Dokument157 SeitenBiology Study Material Final2012 13Tapas BanerjeeNoch keine Bewertungen
- Permanent Family PlanningDokument24 SeitenPermanent Family Planningsurajchavan231116Noch keine Bewertungen
- Unitive and Procreative Health Procreation, Creation and EvolutionDokument9 SeitenUnitive and Procreative Health Procreation, Creation and EvolutionJustJ ThingsNoch keine Bewertungen
- Position Paper Presentation PDFDokument10 SeitenPosition Paper Presentation PDFGladys NamocoNoch keine Bewertungen
- IVM (In Vitro Maturation) WWWWWWWWWDokument17 SeitenIVM (In Vitro Maturation) WWWWWWWWWMirza HassanNoch keine Bewertungen
- Birth Control GuideDokument4 SeitenBirth Control GuideNessaNoch keine Bewertungen
- The Use of Dienogest Before IVFDokument2 SeitenThe Use of Dienogest Before IVFAmeer AbdallahNoch keine Bewertungen
- Oklahoma HIV guide outlines testing, treatment and preventionDokument26 SeitenOklahoma HIV guide outlines testing, treatment and preventionaazmiardiNoch keine Bewertungen
- Premature EjaculationDokument1 SeitePremature EjaculationssmaddiNoch keine Bewertungen
- IUD InsertionDokument4 SeitenIUD InsertionToP Clutches PUBGMNoch keine Bewertungen
- Product Review EllaOne - Ulipristal AcetateDokument7 SeitenProduct Review EllaOne - Ulipristal AcetateAnonymous SDUIPeqXNoch keine Bewertungen
- Multi OrgasmusDokument29 SeitenMulti Orgasmus4gen_30% (1)
- Placenta PreviaDokument9 SeitenPlacenta PreviaVishal GuptaNoch keine Bewertungen
- UGANDA SCOUTS ASSOCIATION SVoice01Dokument1 SeiteUGANDA SCOUTS ASSOCIATION SVoice01Conrad NatseNoch keine Bewertungen
- Antepartum 2Dokument3 SeitenAntepartum 2Emily Davis100% (2)
- Post Abortion Care (Pac)Dokument9 SeitenPost Abortion Care (Pac)api-3705046100% (14)