Das könnte Ihnen auch gefallen
- Pathophysiology and Management of Urinary Retention in Men: Review ArticleDokument7 SeitenPathophysiology and Management of Urinary Retention in Men: Review ArticleRara Aulia IINoch keine Bewertungen
- Daneshmand, 2017Dokument188 SeitenDaneshmand, 2017Rara Aulia IINoch keine Bewertungen
- A Guide For The Assessment and Management of Post-Obstructive DiuresisDokument3 SeitenA Guide For The Assessment and Management of Post-Obstructive DiuresisRara Aulia IINoch keine Bewertungen
- Post-Obstructive Diuresis: A Complication of Urinary RetentionDokument3 SeitenPost-Obstructive Diuresis: A Complication of Urinary RetentionRara Aulia IINoch keine Bewertungen
- Full Text 01Dokument71 SeitenFull Text 01Rara Aulia IINoch keine Bewertungen
- Lobo 2017Dokument10 SeitenLobo 2017Rara Aulia IINoch keine Bewertungen
- Bladder Decompression For Chronic Urinary Retention May Lead To Upper Tract BleedingDokument3 SeitenBladder Decompression For Chronic Urinary Retention May Lead To Upper Tract BleedingRara Aulia IINoch keine Bewertungen
- Postobstructive Diuresis: Clinical ReviewDokument6 SeitenPostobstructive Diuresis: Clinical ReviewRara Aulia IINoch keine Bewertungen
- UC Irvine: Clinical Practice and Cases in Emergency MedicineDokument4 SeitenUC Irvine: Clinical Practice and Cases in Emergency MedicineRara Aulia IINoch keine Bewertungen
- Gynecologic Oncology: Omari K. Johnson, Andrew Berchuck, Angeles A. Secord, Andrew C. PetersonDokument8 SeitenGynecologic Oncology: Omari K. Johnson, Andrew Berchuck, Angeles A. Secord, Andrew C. PetersonRara Aulia IINoch keine Bewertungen
- Urinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesDokument10 SeitenUrinary Diversion After Pelvic Exenteration For Gynecologic MalignanciesRara Aulia IINoch keine Bewertungen
- New and Evolving Immunotherapy in Inflammatory Bowel DiseaseDokument11 SeitenNew and Evolving Immunotherapy in Inflammatory Bowel DiseaseRara Aulia IINoch keine Bewertungen
- E020500 FullDokument11 SeitenE020500 FullRara Aulia IINoch keine Bewertungen
- Urinary Diversion Highlights: Editorial - 50th AnniversaryDokument12 SeitenUrinary Diversion Highlights: Editorial - 50th AnniversaryRara Aulia IINoch keine Bewertungen
- Ileal Neobladder and Its Variants: Georgios Gakis, Arnulf StenzlDokument9 SeitenIleal Neobladder and Its Variants: Georgios Gakis, Arnulf StenzlRara Aulia IINoch keine Bewertungen
- Robotic Urinary Diversion: The Range of Options: ReviewDokument7 SeitenRobotic Urinary Diversion: The Range of Options: ReviewRara Aulia IINoch keine Bewertungen
- Major Protein Sorting Pathways in Eukaryotic CellsDokument19 SeitenMajor Protein Sorting Pathways in Eukaryotic CellsRara Aulia IINoch keine Bewertungen
- Which Knife Was Used Using A Porcine Model To.2Dokument4 SeitenWhich Knife Was Used Using A Porcine Model To.2Rara Aulia IINoch keine Bewertungen
- UpdatesDokument24 SeitenUpdatesRara Aulia IINoch keine Bewertungen
- Vitamin D AdministrationDokument1 SeiteVitamin D AdministrationRara Aulia IINoch keine Bewertungen
- Dong 2015Dokument4 SeitenDong 2015Rara Aulia IINoch keine Bewertungen
- Global Nutrition Report 2016Dokument180 SeitenGlobal Nutrition Report 2016IFPRINoch keine Bewertungen
- What Are The Advantages If We Culture Cell As Our Research Model and What Are The LimitationsDokument1 SeiteWhat Are The Advantages If We Culture Cell As Our Research Model and What Are The LimitationsRara Aulia IINoch keine Bewertungen
- Ijmcmed v3n4p216 enDokument9 SeitenIjmcmed v3n4p216 enRara Aulia IINoch keine Bewertungen
- Bibi 2017Dokument8 SeitenBibi 2017Rara Aulia IINoch keine Bewertungen
- Rna ExtractionDokument21 SeitenRna ExtractionBaoz PingNoch keine Bewertungen
- Materi Sertifikasi TI UBDokument138 SeitenMateri Sertifikasi TI UBMaika100% (2)
- Pediatric Clinics Type 1 Diabetes 2005Dokument26 SeitenPediatric Clinics Type 1 Diabetes 2005Rara Aulia IINoch keine Bewertungen
- HperlipidemiaDokument52 SeitenHperlipidemiaRara Aulia IINoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- PCR Tests and Vaccines DiscussedDokument74 SeitenPCR Tests and Vaccines DiscussedConstantin RaduNoch keine Bewertungen
- PHARMA Revised + Extra QsDokument51 SeitenPHARMA Revised + Extra Qsdoaa naieemNoch keine Bewertungen
- Unit 1 Cell Biology Practice 1: (72 Marks)Dokument17 SeitenUnit 1 Cell Biology Practice 1: (72 Marks)Rita LimNoch keine Bewertungen
- (MT 57) PARA - Pathogenic ProtozoaDokument5 Seiten(MT 57) PARA - Pathogenic ProtozoaLiana JeonNoch keine Bewertungen
- WJG 20 Anniversary Special Issues (3) : Inflammatory Bowel DiseaseDokument10 SeitenWJG 20 Anniversary Special Issues (3) : Inflammatory Bowel DiseaseDeril RidwanNoch keine Bewertungen
- Pharmacology of Antithrombotic AgentsDokument7 SeitenPharmacology of Antithrombotic AgentsadityaNoch keine Bewertungen
- Seminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsDokument14 SeitenSeminar: Annelies Wilder-Smith, Eng-Eong Ooi, Olaf Horstick, Bridget WillsAlexander ArguelloNoch keine Bewertungen
- Enfermedades de Transmision Sexual: Dr. Hernán Alonso Aponte Varón Profesor TitularDokument34 SeitenEnfermedades de Transmision Sexual: Dr. Hernán Alonso Aponte Varón Profesor Titulardiego jNoch keine Bewertungen
- Protozoa-RevisionDokument6 SeitenProtozoa-RevisionIssam HadiNoch keine Bewertungen
- Clinico-Basic Microbiology: Comprehensive Review for Undergraduates & PostgraduatesDokument254 SeitenClinico-Basic Microbiology: Comprehensive Review for Undergraduates & PostgraduatesAimal Khan67% (3)
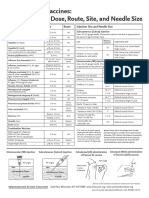
- Administering Vaccines: Dose, Route, Site and Needle Size GuideDokument1 SeiteAdministering Vaccines: Dose, Route, Site and Needle Size GuideKate Lucernas MayugaNoch keine Bewertungen
- Genetics Notes:: A Pair of Factors (Alleles) Is SeparatedDokument6 SeitenGenetics Notes:: A Pair of Factors (Alleles) Is SeparatedNethra Sasikumar100% (1)
- The Eukaryotic Replication Machine: D. Zhang, M. O'DonnellDokument39 SeitenThe Eukaryotic Replication Machine: D. Zhang, M. O'DonnellÁgnes TóthNoch keine Bewertungen
- Viruses (BOT-501) by Dr. Kirtika PadaliaDokument75 SeitenViruses (BOT-501) by Dr. Kirtika PadaliaDinesh MahantNoch keine Bewertungen
- Annual Report 2019 2020Dokument248 SeitenAnnual Report 2019 2020Prince PanwarNoch keine Bewertungen
- Labcomp FDokument23 SeitenLabcomp Fking peaceNoch keine Bewertungen
- Postherpetic NeuralgiaDokument20 SeitenPostherpetic NeuralgiaDimitra VasileiouNoch keine Bewertungen
- IT 9 - Hematology Malignancy - NDDokument93 SeitenIT 9 - Hematology Malignancy - NDDesi MawarniNoch keine Bewertungen
- The World of Science and Innovation 14 16.01.2021Dokument1.289 SeitenThe World of Science and Innovation 14 16.01.2021Костя ДолинськийNoch keine Bewertungen
- Acid Fast StainDokument3 SeitenAcid Fast StainGUIDO ERNESTO VILLOTA CALVACHINoch keine Bewertungen
- Sample Questions: American Board of Medical MicrobiologyDokument8 SeitenSample Questions: American Board of Medical Microbiologyelattar.laila1891Noch keine Bewertungen
- Dictionary of Biomedical Research 4080 Words 155pDokument155 SeitenDictionary of Biomedical Research 4080 Words 155pMSKCNoch keine Bewertungen
- Pituitary Disorders - Adrenal Disorders - Thyroid DiseasesDokument207 SeitenPituitary Disorders - Adrenal Disorders - Thyroid Diseasesnurliah armandNoch keine Bewertungen
- Brochure AurizonDokument5 SeitenBrochure AurizonRachelNoch keine Bewertungen
- Taller 1, Genética MendelianaDokument3 SeitenTaller 1, Genética MendelianaalesssssNoch keine Bewertungen
- Chapter 14 Mendel and The Gene IdeaDokument9 SeitenChapter 14 Mendel and The Gene IdeaJUNG LEENoch keine Bewertungen
- (VCE Biology) 2017 YVG Unit 1 Exam v2Dokument10 Seiten(VCE Biology) 2017 YVG Unit 1 Exam v2Justine LyNoch keine Bewertungen
- The Richest Licorice Medicinal Composition On The Public Health GuardDokument9 SeitenThe Richest Licorice Medicinal Composition On The Public Health GuardInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Gram Negative RodsDokument23 SeitenGram Negative RodsYasir KareemNoch keine Bewertungen
- Halo Internis Edisi 27 - Agustus 2017Dokument49 SeitenHalo Internis Edisi 27 - Agustus 2017HenryOei100% (1)