Das könnte Ihnen auch gefallen
- CHADS2 Score: For Other Uses, SeeDokument5 SeitenCHADS2 Score: For Other Uses, SeeLiseth Victorio HuamanNoch keine Bewertungen
- Anticoagulation in Atrial FibrillationDokument22 SeitenAnticoagulation in Atrial FibrillationprobowurNoch keine Bewertungen
- Σκορ ΛιονηDokument38 SeitenΣκορ ΛιονηΑντώνιος ΧατζηγεωργίουNoch keine Bewertungen
- Not All Ccbs Are Equal Because Your 24 Hours Protection Very ImportantDokument21 SeitenNot All Ccbs Are Equal Because Your 24 Hours Protection Very ImportantSurya RajNoch keine Bewertungen
- Screenshot 2023-10-04 at 09.15.05Dokument1 SeiteScreenshot 2023-10-04 at 09.15.05Joe DrumNoch keine Bewertungen
- Atherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineDokument21 SeitenAtherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineHeryanti PusparisaNoch keine Bewertungen
- Ascvd PrimaryDokument21 SeitenAscvd Primaryprk prkNoch keine Bewertungen
- Atrial Fibrillation and Atrial Flutter Jimmy AsafDokument74 SeitenAtrial Fibrillation and Atrial Flutter Jimmy AsafFikriYTNoch keine Bewertungen
- Cha Ds - Vasc: Condition PointsDokument5 SeitenCha Ds - Vasc: Condition PointsΑντώνιος ΧατζηγεωργίουNoch keine Bewertungen
- Lower Is Better - FinalDokument91 SeitenLower Is Better - FinalJamsidul Hassan RajibNoch keine Bewertungen
- What's New in Lipid GuidelinesDokument31 SeitenWhat's New in Lipid GuidelinesYunita WidyaningsihNoch keine Bewertungen
- Af IndigoDokument60 SeitenAf IndigoLalrin ChhanaNoch keine Bewertungen
- AfibDokument91 SeitenAfibreyNoch keine Bewertungen
- Topic - ADokument4 SeitenTopic - Aapi-549451092Noch keine Bewertungen
- CG CHADS, SHMADS What's All This About AnticoagulationDokument16 SeitenCG CHADS, SHMADS What's All This About Anticoagulationพี่หนูอู๊ดแพ็ตตี้Noch keine Bewertungen
- Arrythmia Management in Primary CareDokument51 SeitenArrythmia Management in Primary CarecelinamannaNoch keine Bewertungen
- PSAP 2019 Dyslipidemia PDFDokument24 SeitenPSAP 2019 Dyslipidemia PDFdellykets_323822919Noch keine Bewertungen
- PSAP 2019 Dyslipidemia PDFDokument24 SeitenPSAP 2019 Dyslipidemia PDFdellykets_323822919Noch keine Bewertungen
- Management of Atrial Fibrillation CNA 2015Dokument14 SeitenManagement of Atrial Fibrillation CNA 2015isaNoch keine Bewertungen
- Prevention of Stroke in Patients With Atrial Fibrillation: A Guide For Primary Care January 2014Dokument13 SeitenPrevention of Stroke in Patients With Atrial Fibrillation: A Guide For Primary Care January 2014Ruth linayantiNoch keine Bewertungen
- Afib For JCU 2Dokument33 SeitenAfib For JCU 2Sofia KusumadewiNoch keine Bewertungen
- Q. Write Down The ECG Criteria of AF?: Atrial Fibrillation (D-470)Dokument5 SeitenQ. Write Down The ECG Criteria of AF?: Atrial Fibrillation (D-470)DR.SANJOY GHOSHNoch keine Bewertungen
- Clinical Risk Factors For Stroke, Transient Ischemic Attack, and Systemic EmboliDokument2 SeitenClinical Risk Factors For Stroke, Transient Ischemic Attack, and Systemic EmboliiglesiasowenNoch keine Bewertungen
- Understanding The Needs of The High Productive DyslipidemiaDokument47 SeitenUnderstanding The Needs of The High Productive DyslipidemiachchchchkNoch keine Bewertungen
- Cha2ds2 Vasc ScoreDokument12 SeitenCha2ds2 Vasc ScorehelviaseptariniNoch keine Bewertungen
- Lower Is Better - FinalDokument91 SeitenLower Is Better - FinalJamsidul Hassan RajibNoch keine Bewertungen
- Anticoagulacion en Fa Lo UltimoDokument6 SeitenAnticoagulacion en Fa Lo Ultimosanalejo0290Noch keine Bewertungen
- Cholesterol Guidelines Review 2020Dokument6 SeitenCholesterol Guidelines Review 2020oriannaocantoNoch keine Bewertungen
- Anticoag Peri Op ManagementDokument16 SeitenAnticoag Peri Op Managementlokeswara reddyNoch keine Bewertungen
- 2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskDokument9 Seiten2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskGandri Ali Ma'suNoch keine Bewertungen
- CCB in HypertensionDokument33 SeitenCCB in HypertensionSuardy CiayadiNoch keine Bewertungen
- New Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesDokument6 SeitenNew Recommendations and Revised Concepts in Recent Guidelines On The Management of Dyslipidemias To Prevent Cardiovascular Disease-The 2018 ACC-AHA and 2019 ESC-EAS GuidelinesJustinaNoch keine Bewertungen
- Curriculum Vitae: Nama: Dr. I B Kusuma P, SP.S TGL Lahir: 27 Maret 1964 Riwayat PendidikanDokument31 SeitenCurriculum Vitae: Nama: Dr. I B Kusuma P, SP.S TGL Lahir: 27 Maret 1964 Riwayat PendidikanJuliana sieNoch keine Bewertungen
- Drogas en Dislipidemia para Prevemncion CVDokument19 SeitenDrogas en Dislipidemia para Prevemncion CVeleanhy95Noch keine Bewertungen
- Aha Guidelinedriven Management of Hypertension An Evidencebased UpdateDokument56 SeitenAha Guidelinedriven Management of Hypertension An Evidencebased UpdateNanda Gopal Reddy AnamNoch keine Bewertungen
- Guidelines For The Management of Atrial Fibrillation Part-IVDokument56 SeitenGuidelines For The Management of Atrial Fibrillation Part-IVJamil Muqtadir BhattiNoch keine Bewertungen
- Atrial Fibrillation FinalDokument67 SeitenAtrial Fibrillation FinalHafiz Wajid SadiqNoch keine Bewertungen
- HypertensionDokument54 SeitenHypertensionAli Murtaza AbbasNoch keine Bewertungen
- Treatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlideDokument31 SeitenTreatment of Hypertension-Zanidip 5 Aug 2017 DR Antonia Rev For SlidejoshuaNoch keine Bewertungen
- Bridging AnticoagulantDokument29 SeitenBridging AnticoagulantTessa OktaramdaniNoch keine Bewertungen
- Initiating Therapy of Hypertension. When and HowDokument53 SeitenInitiating Therapy of Hypertension. When and HowDesy LestariNoch keine Bewertungen
- Chads2 ScoreDokument1 SeiteChads2 ScoreJonas OltmanNoch keine Bewertungen
- Guidelines DyslipidDokument49 SeitenGuidelines Dyslipidnoveldycb89Noch keine Bewertungen
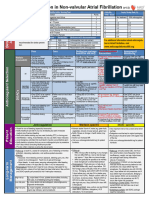
- Anticoagulation in Non-Valvular Atrial FibrillationDokument2 SeitenAnticoagulation in Non-Valvular Atrial Fibrillationadolfozg20041Noch keine Bewertungen
- A Pragmatic View of The New Cholesterol Treatment GuidelinesDokument4 SeitenA Pragmatic View of The New Cholesterol Treatment GuidelinesMaria Fernanda CoralNoch keine Bewertungen
- Afp 20170501 P 580Dokument2 SeitenAfp 20170501 P 580Heryanti PusparisaNoch keine Bewertungen
- Lower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsDokument59 SeitenLower Is Better - No Evidence For Treating To Spepecific Lipid Targets & Use of StatinsJamsidul Hassan RajibNoch keine Bewertungen
- AntitrobotikDokument6 SeitenAntitrobotikollyvia mariance kembuanNoch keine Bewertungen
- L2 Hypertension in Special GroupsDokument44 SeitenL2 Hypertension in Special GroupsMustaquim YusopNoch keine Bewertungen
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDokument8 SeitenRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNoch keine Bewertungen
- Management of Blood Cholesterol 2019Dokument2 SeitenManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNoch keine Bewertungen
- Warfarin Management - Adult - Ambulatory Clinical Practice GuidelineDokument18 SeitenWarfarin Management - Adult - Ambulatory Clinical Practice GuidelineAlexious Marie CalluengNoch keine Bewertungen
- Slide Speaker Candesartan For Hypertension in CKD PatientsDokument43 SeitenSlide Speaker Candesartan For Hypertension in CKD Patientsesdras pramuditaNoch keine Bewertungen
- Warfarin Management - Adult - Inpatient Clinical Practice GuidelineDokument14 SeitenWarfarin Management - Adult - Inpatient Clinical Practice GuidelineRyeskaFajarNoch keine Bewertungen
- Guidelines Made Simple Tool 2018 CholesterolDokument22 SeitenGuidelines Made Simple Tool 2018 CholesterolSafira HalimatussadiahNoch keine Bewertungen
- Special 1030415Dokument9 SeitenSpecial 1030415Maria CostandachiNoch keine Bewertungen
- Well Score: ResultsDokument4 SeitenWell Score: ResultsMalueth AnguiNoch keine Bewertungen
- ToolkitfullDokument75 SeitenToolkitfullapi-278913876100% (1)
- Student Project Herpes Simplex Type 2 InfectionDokument15 SeitenStudent Project Herpes Simplex Type 2 Infectiontiramisu cocoNoch keine Bewertungen
- Vesicovaginal Fistula: Urology DepartmentDokument24 SeitenVesicovaginal Fistula: Urology DepartmentHardiTariqHamma100% (1)
- Drug Study (Schizo)Dokument5 SeitenDrug Study (Schizo)aliannaNoch keine Bewertungen
- Book Eczema PsoriazisDokument457 SeitenBook Eczema Psoriazisdaniel bNoch keine Bewertungen
- ReportDokument4 SeitenReportRancho AmithNoch keine Bewertungen
- Coronary Artery DiseaseDokument3 SeitenCoronary Artery DiseaseMarta Luquez RNoch keine Bewertungen
- ASTHMA & COPD (Emphysema, CB) (CHAP 20)Dokument10 SeitenASTHMA & COPD (Emphysema, CB) (CHAP 20)Abegail QuintoNoch keine Bewertungen
- Electrocardiogram: Dr. PacnaDokument13 SeitenElectrocardiogram: Dr. PacnaEcel AggasidNoch keine Bewertungen
- Health Lesson 2Dokument13 SeitenHealth Lesson 2rosemarie guimbaolibotNoch keine Bewertungen
- Communicable Disease NRSGDokument63 SeitenCommunicable Disease NRSGValeryn QuimanNoch keine Bewertungen
- Case Study of SVIDokument27 SeitenCase Study of SVICristina100% (1)
- Outline On Dengue Fever - EDITEDDokument2 SeitenOutline On Dengue Fever - EDITEDDavid Skeat0% (1)
- Cancer of The CervixDokument68 SeitenCancer of The CervixSandra mugunzvaNoch keine Bewertungen
- DVT Case StudyDokument2 SeitenDVT Case StudyCrystal B Costa78Noch keine Bewertungen
- Alterations With Infectious Inflammatory and Immunologic Responses 1Dokument42 SeitenAlterations With Infectious Inflammatory and Immunologic Responses 1PATRIZJA YSABEL REYESNoch keine Bewertungen
- Uterine Fibroids ReportDokument3 SeitenUterine Fibroids ReportVince John SevillaNoch keine Bewertungen
- Fall From Heights Emergency Procedure - ACE CivilDokument1 SeiteFall From Heights Emergency Procedure - ACE CivilNicole AnthonyNoch keine Bewertungen
- Lumbar SpondylosisDokument26 SeitenLumbar SpondylosisBanni Aprilita PratiwiNoch keine Bewertungen
- 2 Months Well Child CheckDokument3 Seiten2 Months Well Child CheckJanelleNoch keine Bewertungen
- Nursing Care Plan Funds 2Dokument8 SeitenNursing Care Plan Funds 2Yash RamawatNoch keine Bewertungen
- AnxietyDokument48 SeitenAnxietyGira HirparaNoch keine Bewertungen
- Pref - 7 - Vocabulary 3.7 - Revisión Del Intento PDFDokument4 SeitenPref - 7 - Vocabulary 3.7 - Revisión Del Intento PDFnaslyNoch keine Bewertungen
- Presentation On Care of Critically Ill PatientDokument9 SeitenPresentation On Care of Critically Ill Patientanamika sharmaNoch keine Bewertungen
- Microbiology Module 7 - BacilliDokument87 SeitenMicrobiology Module 7 - BacilliArt Arts100% (1)
- Adhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Dokument56 SeitenAdhesive Small Bowel Obstruction: Leslie Kobayashi Trauma Conference 2013Ananda RizkiNoch keine Bewertungen
- Medicine - BhanuDokument469 SeitenMedicine - BhanuHIMAVARADHAN UNoch keine Bewertungen
- Assessment Diagnosis Planning Intervention Rationale EvaluationDokument2 SeitenAssessment Diagnosis Planning Intervention Rationale EvaluationKim SungaNoch keine Bewertungen
- Ncp. Oral MucosaDokument1 SeiteNcp. Oral MucosaZmiaNoch keine Bewertungen
- Shashikant PDFDokument4 SeitenShashikant PDFAacharya Shashikant VashishthNoch keine Bewertungen
- Uwise ReviewDokument14 SeitenUwise ReviewAnonymous T1G9BQQNoch keine Bewertungen