Das könnte Ihnen auch gefallen
- Chapter 2 The Z Plasty 2000 Fundamental Techniques of Plastic Surgery Tenth EditionDokument14 SeitenChapter 2 The Z Plasty 2000 Fundamental Techniques of Plastic Surgery Tenth Editionwerewolf3107Noch keine Bewertungen
- Miles Operation - Abdominoperineal Excision - Rectal CADokument5 SeitenMiles Operation - Abdominoperineal Excision - Rectal CASpencer DempseyNoch keine Bewertungen
- ComponentsDokument5 SeitenComponentsprakashmathewNoch keine Bewertungen
- Bone and Soft Tissue SarcomaDokument67 SeitenBone and Soft Tissue SarcomaSalmanArifNoch keine Bewertungen
- AnastomosisDokument7 SeitenAnastomosissuri84Noch keine Bewertungen
- Breast Cancer The LANCET Abril 2021Dokument20 SeitenBreast Cancer The LANCET Abril 2021Hernán Salazar RománNoch keine Bewertungen
- Nordtest Method NT Fire 049Dokument16 SeitenNordtest Method NT Fire 049mail2021Noch keine Bewertungen
- CHM Analysis and Comparisons of CRUS MULTHULLS2013Dokument60 SeitenCHM Analysis and Comparisons of CRUS MULTHULLS2013kkd108Noch keine Bewertungen
- 4TWX4036 Service FactsDokument4 Seiten4TWX4036 Service FactsAlejandro OrdoñezNoch keine Bewertungen
- Axillary Node DissectionDokument71 SeitenAxillary Node DissectionKartik Kaistha100% (1)
- Radial Forearm Free FlapDokument54 SeitenRadial Forearm Free FlapWakilAhmadNoch keine Bewertungen
- Skin - Grafts by Madhuri GoreDokument112 SeitenSkin - Grafts by Madhuri GoreAnonymous 8hVpaQdCtr100% (1)
- Soft Tissue SarcomaDokument45 SeitenSoft Tissue SarcomaWadhe TobingNoch keine Bewertungen
- FR Distal HumerusDokument55 SeitenFR Distal Humerusiisscribd100% (1)
- Degenerative Diseases of SpineDokument115 SeitenDegenerative Diseases of SpineCodillia CheongNoch keine Bewertungen
- FasciotomyDokument17 SeitenFasciotomyPrasojo JojoNoch keine Bewertungen
- Transient SynovitisDokument9 SeitenTransient SynovitisMuhammad Taufik AdhyatmaNoch keine Bewertungen
- Understanding Musculoskeletal TumoursDokument106 SeitenUnderstanding Musculoskeletal TumoursBharath NarasimhaNoch keine Bewertungen
- Bone Tumor: Daniel A. (Orthopedic Surgeon)Dokument225 SeitenBone Tumor: Daniel A. (Orthopedic Surgeon)mebrieNoch keine Bewertungen
- Shoulder Joint ReplacementDokument10 SeitenShoulder Joint ReplacementSiva ShanmugamNoch keine Bewertungen
- Tibia Shaft Fracture TreatmentDokument26 SeitenTibia Shaft Fracture Treatmentgalih widodoNoch keine Bewertungen
- Abdominal Incision1Dokument11 SeitenAbdominal Incision1njoNoch keine Bewertungen
- NeckdissectionsDokument130 SeitenNeckdissectionsAlvaro RivCalleNoch keine Bewertungen
- Fingertip Reconstruction Using Cross-Finger Flap TechniqueDokument36 SeitenFingertip Reconstruction Using Cross-Finger Flap TechniquevenuNoch keine Bewertungen
- Abdominal SurgeryDokument166 SeitenAbdominal SurgeryIndera VyasNoch keine Bewertungen
- Neoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerDokument57 SeitenNeoplastic Thyroid Disease - Thyroid Nodules Goiter and Thyroid CancerNavya SreeNoch keine Bewertungen
- Management of Thyroid CancerDokument57 SeitenManagement of Thyroid CancerAshis SahaNoch keine Bewertungen
- Anorectal Surgery PDFDokument33 SeitenAnorectal Surgery PDFLuminitaDumitriuNoch keine Bewertungen
- Open Hernia RepairDokument22 SeitenOpen Hernia RepairMuhammad AbdurrahmanNoch keine Bewertungen
- Tissue Repair: Kristine Krafts, M.D. - September 13, 2010Dokument59 SeitenTissue Repair: Kristine Krafts, M.D. - September 13, 2010Antonino CassottaNoch keine Bewertungen
- AmputationDokument40 SeitenAmputationAmruth KhNoch keine Bewertungen
- Tendon InjuriesDokument48 SeitenTendon InjuriesdiasNoch keine Bewertungen
- Gas Gangrene in Orthopaedic PatientsDokument18 SeitenGas Gangrene in Orthopaedic PatientsdennyefendiNoch keine Bewertungen
- Hand Infection Guide: Felons to Flexor TenosynovitisDokument68 SeitenHand Infection Guide: Felons to Flexor TenosynovitisSuren VishvanathNoch keine Bewertungen
- Credibility of Three Column Fixation in Schatzker Types V and VI Tibial Plateau FracturesDokument6 SeitenCredibility of Three Column Fixation in Schatzker Types V and VI Tibial Plateau FracturesInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Excision of Branchial Cleft CystsDokument10 SeitenExcision of Branchial Cleft Cystssjs315Noch keine Bewertungen
- Nur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin PalembangDokument38 SeitenNur Rachmat Lubis: Divisi Orthopaedi Dept Bedah FK UNSRI/ RS Dr. M. Hoesin Palembangsoleha09la solehaNoch keine Bewertungen
- Definition of Damage Control OrthopaedicsDokument2 SeitenDefinition of Damage Control OrthopaedicsHerryanto Agustriadi100% (1)
- Flexor Tendon Surgery - 25 Years of Progress - Strickland - JHS 2000Dokument22 SeitenFlexor Tendon Surgery - 25 Years of Progress - Strickland - JHS 2000Professeur Christian DumontierNoch keine Bewertungen
- Transhiatal EsophagectomyDokument12 SeitenTranshiatal EsophagectomyprofarmahNoch keine Bewertungen
- Cysts of Pancreas RADIOLOGYDokument20 SeitenCysts of Pancreas RADIOLOGYmhany12345Noch keine Bewertungen
- Distal Amputations For The Diabetic Foot PDFDokument4 SeitenDistal Amputations For The Diabetic Foot PDFGiuliana ReyesNoch keine Bewertungen
- External Fixation of FemurDokument27 SeitenExternal Fixation of FemurMemoona AmeerNoch keine Bewertungen
- Hand Surgery Trauma OrthoDokument59 SeitenHand Surgery Trauma OrthoFiki A RisentaNoch keine Bewertungen
- Recent Advances in The Treatment of FracturesDokument29 SeitenRecent Advances in The Treatment of Fracturesmanjunatha100% (1)
- Surgical Anatomy-Anal Canal: Dr. Belal MansoorDokument79 SeitenSurgical Anatomy-Anal Canal: Dr. Belal MansoorYogi drNoch keine Bewertungen
- Damage Control OrthopaedicsDokument16 SeitenDamage Control OrthopaedicsPatrick LukitoNoch keine Bewertungen
- Management of Fractures - DR Matthew SherlockDokument142 SeitenManagement of Fractures - DR Matthew Sherlockreeves_cool100% (1)
- Epidural HematomaDokument16 SeitenEpidural HematomaDavid ZamrilNoch keine Bewertungen
- PreOp Planning For THRDokument60 SeitenPreOp Planning For THRronnyNoch keine Bewertungen
- Neligan Mandible FractureDokument17 SeitenNeligan Mandible FractureRibka TheodoraNoch keine Bewertungen
- Tugas Vascular AnomaliesDokument26 SeitenTugas Vascular AnomaliesElno TatipikalawanNoch keine Bewertungen
- Anatomy of the Pelvis and PerineumDokument101 SeitenAnatomy of the Pelvis and PerineumCiprianTeodorulNoch keine Bewertungen
- New Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauDokument8 SeitenNew Trends and Techniques in Open Reduction and Internal Fixation of Fractures of The Tibial PlateauCosmina BribanNoch keine Bewertungen
- Flexor Tendon Injuries of the Hand: Treatment and RehabilitationDokument94 SeitenFlexor Tendon Injuries of the Hand: Treatment and RehabilitationGobinath KannanNoch keine Bewertungen
- Simple MastectomyDokument3 SeitenSimple MastectomyCindy DayocNoch keine Bewertungen
- Management of Intraarticular Hand FracturesDokument86 SeitenManagement of Intraarticular Hand FracturesthrylibanNoch keine Bewertungen
- Anatomy of The AxillarDokument43 SeitenAnatomy of The AxillarJustine NyangaresiNoch keine Bewertungen
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDokument28 SeitenOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNoch keine Bewertungen
- AO Trauma Vol.2Dokument100 SeitenAO Trauma Vol.2Cujba GheorgheNoch keine Bewertungen
- Distribusi Patah Tulang Panjang TerbukaDokument73 SeitenDistribusi Patah Tulang Panjang TerbukaCininta Anisa SavitriNoch keine Bewertungen
- Current Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderVon EverandCurrent Challenges with their Evolving Solutions in Surgical Practice in West Africa: A ReaderNoch keine Bewertungen
- Glandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.Dokument2 SeitenGlandula Salivales. Tto de Enfermedad Locorregional. UpToDate 2022.juanrangoneNoch keine Bewertungen
- 9 Biopsy of The Sentinel Lymph NodeDokument32 Seiten9 Biopsy of The Sentinel Lymph NodejuanrangoneNoch keine Bewertungen
- Parotidectomia - UpToDate 2022Dokument2 SeitenParotidectomia - UpToDate 2022juanrangoneNoch keine Bewertungen
- Parathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022Dokument42 SeitenParathyroid Exploration For Primary Hyperparathyroidism - Uptodate 2022juanrangoneNoch keine Bewertungen
- Lymph Node Dissection Techniques and Indications for Melanoma PatientsDokument19 SeitenLymph Node Dissection Techniques and Indications for Melanoma PatientsjuanrangoneNoch keine Bewertungen
- Parathyroid Surgery For Inherited Syndromes - Uptodate 2022Dokument25 SeitenParathyroid Surgery For Inherited Syndromes - Uptodate 2022juanrangoneNoch keine Bewertungen
- Intraoperative PTH assays predict post-op calciumDokument18 SeitenIntraoperative PTH assays predict post-op calciumjuanrangoneNoch keine Bewertungen
- Localization for parathyroid surgeryDokument22 SeitenLocalization for parathyroid surgeryjuanrangoneNoch keine Bewertungen
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Dokument8 SeitenSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNoch keine Bewertungen
- Localization for parathyroid surgeryDokument22 SeitenLocalization for parathyroid surgeryjuanrangoneNoch keine Bewertungen
- Parathyroidectomy in End-Stage Kidney Disease - Uptodate 2022Dokument27 SeitenParathyroidectomy in End-Stage Kidney Disease - Uptodate 2022juanrangoneNoch keine Bewertungen
- Vandeventer 2010Dokument8 SeitenVandeventer 2010juanrangoneNoch keine Bewertungen
- Surgical Anatomy of The Parathyroid Glands - Uptodate 2022Dokument8 SeitenSurgical Anatomy of The Parathyroid Glands - Uptodate 2022juanrangoneNoch keine Bewertungen
- 1 A History Fo Melanoma - From Hunter To Morton Sober2019Dokument19 Seiten1 A History Fo Melanoma - From Hunter To Morton Sober2019juanrangoneNoch keine Bewertungen
- 5 Axillary and Epitrochlear Lymph Node Dissection For MelanomaDokument11 Seiten5 Axillary and Epitrochlear Lymph Node Dissection For MelanomajuanrangoneNoch keine Bewertungen
- The Attachments of The Breast To The Chest Wall: A Dissection StudyDokument12 SeitenThe Attachments of The Breast To The Chest Wall: A Dissection StudyjuanrangoneNoch keine Bewertungen
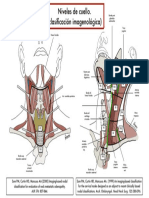
- Niveles cuello clasificacion imagenologicaDokument1 SeiteNiveles cuello clasificacion imagenologicajuanrangoneNoch keine Bewertungen
- Anatomy of The Superficial Fascia System of The Breast: A Comprehensive Theory of Breast Fascial AnatomyDokument10 SeitenAnatomy of The Superficial Fascia System of The Breast: A Comprehensive Theory of Breast Fascial AnatomyLuiggi FayadNoch keine Bewertungen
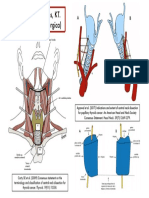
- Niveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesDokument1 SeiteNiveles de Robbins, KT. (Clasificación Quirúrgica) : Hueso HioidesjuanrangoneNoch keine Bewertungen
- AnsaCervicalis Chhetri1997Dokument7 SeitenAnsaCervicalis Chhetri1997ita mustainahNoch keine Bewertungen
- Vandeventer 2016Dokument10 SeitenVandeventer 2016juanrangoneNoch keine Bewertungen
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Dokument5 SeitenSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Surgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.Dokument6 SeitenSurgical Anatomy and Operative Technique of The Axillary Lymph Node Dissection.juanrangone100% (2)
- Alternator NotesDokument24 SeitenAlternator Notesarunima arunimaNoch keine Bewertungen
- Hufenus 2006 Geotextiles GeomembranesDokument18 SeitenHufenus 2006 Geotextiles Geomembranesbkollarou9632Noch keine Bewertungen
- Vietnam & Angkor Wat (PDFDrive) PDFDokument306 SeitenVietnam & Angkor Wat (PDFDrive) PDFChristine TranNoch keine Bewertungen
- Educ 211 Ancient EgyptDokument27 SeitenEduc 211 Ancient Egyptapi-207262700Noch keine Bewertungen
- CodigosDokument73 SeitenCodigosEnzo Miguel Sarabia MontesNoch keine Bewertungen
- Tenofovir Disoproxil Fumarate: Riefing - Nfrared BsorptionDokument4 SeitenTenofovir Disoproxil Fumarate: Riefing - Nfrared BsorptionMostofa RubalNoch keine Bewertungen
- This Is Your Presentation TitleDokument28 SeitenThis Is Your Presentation TitleStephanie AcarapiNoch keine Bewertungen
- CSSBI Tablas de Carga Perfiles PDFDokument60 SeitenCSSBI Tablas de Carga Perfiles PDFRamón RocaNoch keine Bewertungen
- 3-Ph Induction MotorDokument246 Seiten3-Ph Induction MotorAn00pgadzillaNoch keine Bewertungen
- SPECIFIC GRAVITY - DENSITY OF HYDRAULIC CEMENT (IS - 4031-Part 11-1988)Dokument6 SeitenSPECIFIC GRAVITY - DENSITY OF HYDRAULIC CEMENT (IS - 4031-Part 11-1988)Pritha DasNoch keine Bewertungen
- Meditations on Ancient Astrology Principles from Brihat Parashari HorāDokument87 SeitenMeditations on Ancient Astrology Principles from Brihat Parashari HorāPrasanna KumarNoch keine Bewertungen
- 32776Dokument6 Seiten32776Muqtar KhanNoch keine Bewertungen
- Surface Roughness Measurement - MitutoyoDokument2 SeitenSurface Roughness Measurement - MitutoyoSelvaraj BalasundramNoch keine Bewertungen
- 2nd Semester All Courses-100Dokument194 Seiten2nd Semester All Courses-100Ejiade PeterNoch keine Bewertungen
- Anorexia NervosaDokument2 SeitenAnorexia NervosaDhea Mae MadisNoch keine Bewertungen
- Sharp LC 50le440u ProspectoDokument2 SeitenSharp LC 50le440u ProspectovwcxlNoch keine Bewertungen
- Scheme of Valuation and Key for Transportation Engineering ExamDokument3 SeitenScheme of Valuation and Key for Transportation Engineering ExamSivakumarNoch keine Bewertungen
- Structural Notes SampleDokument14 SeitenStructural Notes SampleNicole FrancisNoch keine Bewertungen
- General Biology 2: Quarter 3, Module 1 Genetic EngineeringDokument20 SeitenGeneral Biology 2: Quarter 3, Module 1 Genetic EngineeringRonalyn AndaganNoch keine Bewertungen
- THEORY of METAL CUTTING-Cutting Tool, Cutting Fluid & Machining EconomicsDokument17 SeitenTHEORY of METAL CUTTING-Cutting Tool, Cutting Fluid & Machining EconomicsIzi75% (4)
- Uv Spectrophotometric Estimation of Carvedilol Hydrochloride by First Order Derivative and Area Under Curve Methods in Bulk and PH PDFDokument7 SeitenUv Spectrophotometric Estimation of Carvedilol Hydrochloride by First Order Derivative and Area Under Curve Methods in Bulk and PH PDFMeilia SuhermanNoch keine Bewertungen
- Organization Structure Training KAJARIADokument30 SeitenOrganization Structure Training KAJARIAViswanth GanaparthiNoch keine Bewertungen
- English Task Resumido 2Dokument12 SeitenEnglish Task Resumido 2Luis ArmandoNoch keine Bewertungen
- Weekly Report 52Dokument196 SeitenWeekly Report 52Erceanu DanNoch keine Bewertungen
- El DoradoDokument12 SeitenEl Doradoandrewwilliampalileo@yahoocomNoch keine Bewertungen
- Personal Care Na Hair GuideDokument8 SeitenPersonal Care Na Hair GuideIsabellaNoch keine Bewertungen
- IB Chemistry HL Test 2nd FEBDokument13 SeitenIB Chemistry HL Test 2nd FEBprasad100% (1)