Das könnte Ihnen auch gefallen
- Hospital Claim - Template24 - Page4Dokument1 SeiteHospital Claim - Template24 - Page4chamuditha dilshanNoch keine Bewertungen
- Pediatric History Taking EditDokument6 SeitenPediatric History Taking EditWayNoch keine Bewertungen
- Medical History FormDokument4 SeitenMedical History FormevalinadrNoch keine Bewertungen
- L Q Q O P E R A::::: 教育::::::: Travel: Pet: Contact: Community: Medical Hx Dx Other (手術,日常用藥)Dokument2 SeitenL Q Q O P E R A::::: 教育::::::: Travel: Pet: Contact: Community: Medical Hx Dx Other (手術,日常用藥)jamieNoch keine Bewertungen
- Medical Examination Form 2022-2023Dokument5 SeitenMedical Examination Form 2022-2023Linh ĐặngNoch keine Bewertungen
- S1P3G3 IgnacioDokument8 SeitenS1P3G3 IgnacioJose Mari S IgnacioNoch keine Bewertungen
- S1P2G3 IgnacioDokument9 SeitenS1P2G3 IgnacioJose Mari S IgnacioNoch keine Bewertungen
- SANDIGAN - Case #1 AY21-22 - 2nd SemDokument9 SeitenSANDIGAN - Case #1 AY21-22 - 2nd SemHazelle Joyce SandiganNoch keine Bewertungen
- Neurology Clinical History FormDokument2 SeitenNeurology Clinical History FormZainab JawadNoch keine Bewertungen
- NDR 325 (Provider of Care I: Adult & Elder Health) : Case Study PresentationDokument14 SeitenNDR 325 (Provider of Care I: Adult & Elder Health) : Case Study PresentationR GhNoch keine Bewertungen
- Legal History and PEDokument1 SeiteLegal History and PELoreto District Hospital LDHNoch keine Bewertungen
- Nmanisce@ibew - On.ca: Street City Postal CodeDokument1 SeiteNmanisce@ibew - On.ca: Street City Postal Code100135007Noch keine Bewertungen
- Health I StoryDokument1 SeiteHealth I StorySuzanne DeaultNoch keine Bewertungen
- PONR Assessment ToolDokument9 SeitenPONR Assessment ToolNeirfla WassabiNoch keine Bewertungen
- Pedia HST TemplateDokument9 SeitenPedia HST TemplateRyan Loyd MarquezNoch keine Bewertungen
- Smart Sheet For History Taking in SurgeryDokument7 SeitenSmart Sheet For History Taking in Surgerymahmoud selimNoch keine Bewertungen
- Medical HistoryDokument2 SeitenMedical HistoryMiguel San JuanNoch keine Bewertungen
- Peds WW Form1 - 1Dokument17 SeitenPeds WW Form1 - 1Karess AvilloNoch keine Bewertungen
- Infant Assessment FormDokument2 SeitenInfant Assessment FormteuuuuNoch keine Bewertungen
- Healthhistoryform 2018Dokument2 SeitenHealthhistoryform 2018iwasan991Noch keine Bewertungen
- Medicalhistoryformpg 1Dokument2 SeitenMedicalhistoryformpg 1reynanfrancebernabeNoch keine Bewertungen
- CompiledDokument9 SeitenCompiledcogiezamoraNoch keine Bewertungen
- Simple Nutrition Questionnaire in PDFDokument10 SeitenSimple Nutrition Questionnaire in PDFYezha HiterozaNoch keine Bewertungen
- Jaundice: TypesDokument23 SeitenJaundice: TypesSaranya DeviNoch keine Bewertungen
- JaundiceDokument5 SeitenJaundiceshyft1611Noch keine Bewertungen
- Health History 3Dokument2 SeitenHealth History 3boinkjilijoyNoch keine Bewertungen
- Physical Assessment of An Ulcer PatientDokument4 SeitenPhysical Assessment of An Ulcer PatientNevoj_Nygrin_3313Noch keine Bewertungen
- History Taking SurgeryDokument8 SeitenHistory Taking SurgeryKingston HoNoch keine Bewertungen
- Sickle-Cell Anemia: Chloe Agnes Regina L. AranasDokument19 SeitenSickle-Cell Anemia: Chloe Agnes Regina L. AranasJon AbalosNoch keine Bewertungen
- New Patient/Consultation Form: AllergiesDokument2 SeitenNew Patient/Consultation Form: AllergiesAlexander Flores SaraviaNoch keine Bewertungen
- Signs N Symptoms of GEHDokument83 SeitenSigns N Symptoms of GEHDdh2812Noch keine Bewertungen
- Gynae HistoriesDokument2 SeitenGynae HistoriesZahraa Al-SayedNoch keine Bewertungen
- POMER - Dengue Case PresentationDokument53 SeitenPOMER - Dengue Case Presentationdenzel0711Noch keine Bewertungen
- Im Case 4Dokument49 SeitenIm Case 4PARADISE JanoNoch keine Bewertungen
- History Taking For FeverDokument13 SeitenHistory Taking For FeverAfiQsyazwan Abd RaniNoch keine Bewertungen
- Patient InformationDokument2 SeitenPatient Informationsteve6621Noch keine Bewertungen
- NCM 112 - Renal DisordersDokument4 SeitenNCM 112 - Renal DisordersCailah Sofia SelausoNoch keine Bewertungen
- Case Study Male MSW 1Dokument27 SeitenCase Study Male MSW 1JONAMAY RAMIREZNoch keine Bewertungen
- S1P4G3 IgnacioDokument10 SeitenS1P4G3 IgnacioJose Mari S IgnacioNoch keine Bewertungen
- OB-GYN Patient History and PEDokument4 SeitenOB-GYN Patient History and PEAngelique TongsonNoch keine Bewertungen
- Recognition of Stis: Differential Diagnosis Ectopic PregnancyDokument2 SeitenRecognition of Stis: Differential Diagnosis Ectopic PregnancyLing101Noch keine Bewertungen
- Medicine History and CounsellingDokument13 SeitenMedicine History and Counsellingpranjl100% (1)
- Drexel Medicine New Patient Questionnaire 20160504Dokument7 SeitenDrexel Medicine New Patient Questionnaire 20160504Sameer shetyeNoch keine Bewertungen
- Up Form No2Dokument2 SeitenUp Form No2Mitch Elle InfanteNoch keine Bewertungen
- 2021 03 19 - Test Go - Co-Morbidity DeclarationDokument1 Seite2021 03 19 - Test Go - Co-Morbidity Declarationyinka omojesuNoch keine Bewertungen
- King Khaled Eye Specialist Hospital: Patient Referral FormDokument5 SeitenKing Khaled Eye Specialist Hospital: Patient Referral Formفيصل الرباحNoch keine Bewertungen
- اسسمنت ١Dokument7 Seitenاسسمنت ١almayasa2002Noch keine Bewertungen
- Pediatric History - TemplateDokument5 SeitenPediatric History - TemplateJolaine ValloNoch keine Bewertungen
- Pediatric Test 2Dokument28 SeitenPediatric Test 2Nurse JonesNoch keine Bewertungen
- DiabetesDefects Cleared PDFDokument1 SeiteDiabetesDefects Cleared PDFAtla sai keshava reddyNoch keine Bewertungen
- Infectious Disease ConferenceDokument35 SeitenInfectious Disease ConferenceKatrina CajigalNoch keine Bewertungen
- CONCEPT MAP Bipedal EdemaDokument2 SeitenCONCEPT MAP Bipedal EdemaVineeNoch keine Bewertungen
- Im DkaDokument16 SeitenIm DkaTrisNoch keine Bewertungen
- GI Bleeding HXDokument3 SeitenGI Bleeding HXBitu JaaNoch keine Bewertungen
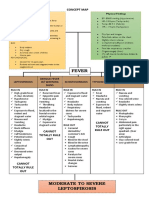
- IM - Leptospirosis Concept MapDokument3 SeitenIM - Leptospirosis Concept MapTrisNoch keine Bewertungen
- Meedical History FormDokument3 SeitenMeedical History FormSonja OsmanovićNoch keine Bewertungen
- Health Declaration Form14 - 2022Dokument3 SeitenHealth Declaration Form14 - 2022DawnNoch keine Bewertungen
- Bleeding DisordersDokument4 SeitenBleeding DisordersRitz CelsoNoch keine Bewertungen
- PoliomyelitisDokument13 SeitenPoliomyelitiscasandra morante100% (2)
- JAAOS - Volume 11 - Issue 01 January & February 2003Dokument77 SeitenJAAOS - Volume 11 - Issue 01 January & February 2003kenthepaNoch keine Bewertungen
- Self-Assessment Quiz: Introduction To Epidemiology Page 1-85Dokument75 SeitenSelf-Assessment Quiz: Introduction To Epidemiology Page 1-85Coy Nuñez100% (4)
- Community Health Education AssignmentDokument9 SeitenCommunity Health Education AssignmentLeenCo TechNoch keine Bewertungen
- Essay ELPTDokument4 SeitenEssay ELPTGalang HashfiansyahNoch keine Bewertungen
- State Magazine, September 2003Dokument44 SeitenState Magazine, September 2003State MagazineNoch keine Bewertungen
- Tutorial 1.1 - Measuring Disease Occurence (Morbidity) - Students - UpdateDokument3 SeitenTutorial 1.1 - Measuring Disease Occurence (Morbidity) - Students - UpdateFebriansyah 'ebhi'100% (1)
- The Psychological and Health Risks of Tattoos: Tattooing 1Dokument7 SeitenThe Psychological and Health Risks of Tattoos: Tattooing 1Chris ProvostNoch keine Bewertungen
- Causes of Hearing LossDokument58 SeitenCauses of Hearing LossHalley MichelleNoch keine Bewertungen
- NCP Ineffective AirwayDokument3 SeitenNCP Ineffective AirwayCat San Gabriel AmuraoNoch keine Bewertungen
- Pityriasis Rosea SlideDokument13 SeitenPityriasis Rosea SlideHaninaAljufriMomentNoch keine Bewertungen
- Bacillus Anthracis: Basic Laboratory Protocols For The Presumptive Identification ofDokument16 SeitenBacillus Anthracis: Basic Laboratory Protocols For The Presumptive Identification ofMyro DarlandanNoch keine Bewertungen
- Bacterial Serological TestsDokument81 SeitenBacterial Serological TestsAffie SaikolNoch keine Bewertungen
- YES-INUIT GOT CANCER. PALEO NOW DEBUNKED. WESTON PRICE DEBUNKED - Inuit Greenland Mummies Confirmed Infested With Carcinoma, Bone Disease, Birth Defects, Lice, And Parasites, While on Wholly Native Meat Based Primal Natural Paleolithic DietDokument1 SeiteYES-INUIT GOT CANCER. PALEO NOW DEBUNKED. WESTON PRICE DEBUNKED - Inuit Greenland Mummies Confirmed Infested With Carcinoma, Bone Disease, Birth Defects, Lice, And Parasites, While on Wholly Native Meat Based Primal Natural Paleolithic DietFRAUDWATCHCOMMISSIONNoch keine Bewertungen
- Zika VirusDokument5 SeitenZika VirusStephanie Joy EscalaNoch keine Bewertungen
- Elastin TopicDokument29 SeitenElastin TopicAaveeza KhanumNoch keine Bewertungen
- Biostatistics and Role in DentistryDokument90 SeitenBiostatistics and Role in DentistryJyoti Sharma100% (1)
- Covid 19 Effects On The Society, Politics, Economy and CultureDokument12 SeitenCovid 19 Effects On The Society, Politics, Economy and CultureChris CharzNoch keine Bewertungen
- 2020-COR-TXT Planetary Emergency 2-0-Aug2020Dokument9 Seiten2020-COR-TXT Planetary Emergency 2-0-Aug2020Mika DeverinNoch keine Bewertungen
- Daftar PustakaDokument4 SeitenDaftar PustakaAnisa OktavianiNoch keine Bewertungen
- My Experience During COVID-19 LockdownDokument2 SeitenMy Experience During COVID-19 LockdownAmrish ThapaNoch keine Bewertungen
- Informal Letter DengueDokument2 SeitenInformal Letter DengueIrsyad IzzatNoch keine Bewertungen
- A Short History of The Stamford & Rutland HospitalDokument47 SeitenA Short History of The Stamford & Rutland HospitalJohn McKechnie100% (1)
- Clinical Tips Part - 1 PDFDokument4 SeitenClinical Tips Part - 1 PDFshclinic0% (1)
- Viruses, Viroids, and PrionsDokument45 SeitenViruses, Viroids, and PrionsJillian LaoNoch keine Bewertungen
- Some Common Special StainsDokument4 SeitenSome Common Special StainsDrramyRaafatNoch keine Bewertungen
- Autoimmune Abnormalities of Postpartum Thyroid DiseasesDokument8 SeitenAutoimmune Abnormalities of Postpartum Thyroid DiseasesIpan MahendriyansaNoch keine Bewertungen
- Health Education Counseling Unit of Anemia in Pregnant WomenDokument6 SeitenHealth Education Counseling Unit of Anemia in Pregnant WomenNofri mansaNoch keine Bewertungen
- Contoh AbstractDokument2 SeitenContoh AbstractFajar Tea JieNoch keine Bewertungen