Das könnte Ihnen auch gefallen
- TM 55 1520 236 23P 1Dokument843 SeitenTM 55 1520 236 23P 1Tod A. Wulff100% (1)
- Scorpio PDFDokument3 SeitenScorpio PDFnimi2364010Noch keine Bewertungen
- High Myopia and Glaucoma Susceptibility The Beijing Eye StudyDokument5 SeitenHigh Myopia and Glaucoma Susceptibility The Beijing Eye StudyDickyStevanoZukhriNoch keine Bewertungen
- Supergene High Yield Introgressed Hybrid Oil Palm MalaysiaDokument16 SeitenSupergene High Yield Introgressed Hybrid Oil Palm MalaysiaYangSern Lim100% (13)
- Broadway CafeDokument13 SeitenBroadway CafeIoana Taon100% (1)
- Astm E1975 - 1 (En)Dokument17 SeitenAstm E1975 - 1 (En)Dinesh Sai100% (1)
- Jurnal MataDokument7 SeitenJurnal MatafaniaapriskaNoch keine Bewertungen
- AstigmatismDokument29 SeitenAstigmatismAmjad bbsulkNoch keine Bewertungen
- Intracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryDokument5 SeitenIntracameral Mydriatics Versus Topical Mydriatics in Pupil Dilation For Phacoemulsification Cataract SurgeryGlaucoma UnhasNoch keine Bewertungen
- Intermittent Exotropia Our Experience in Surgical Outcomes 2155 9570 1000722Dokument3 SeitenIntermittent Exotropia Our Experience in Surgical Outcomes 2155 9570 1000722Ikmal ShahromNoch keine Bewertungen
- Jurnal Mata Sodium Hyaluronate PDFDokument7 SeitenJurnal Mata Sodium Hyaluronate PDFAstrid RumbiaNoch keine Bewertungen
- Jurnal MataDokument4 SeitenJurnal MatamarinarizkiNoch keine Bewertungen
- Clinical Characteristics of Intermittent Exotropia1Dokument7 SeitenClinical Characteristics of Intermittent Exotropia1Ikmal ShahromNoch keine Bewertungen
- Incision and Curettage Versus Steroid Injection For The Treatment of Chalazia: A Meta-AnalysisDokument5 SeitenIncision and Curettage Versus Steroid Injection For The Treatment of Chalazia: A Meta-AnalysisbellaleonoraNoch keine Bewertungen
- Mills 2004Dokument8 SeitenMills 2004Tari RiyastiNoch keine Bewertungen
- Ahmed Glaucoma Valve and Single-Plate Molteno Implants in Treatment of Refractory Glaucoma: A Comparative StudyDokument10 SeitenAhmed Glaucoma Valve and Single-Plate Molteno Implants in Treatment of Refractory Glaucoma: A Comparative StudyVlady BordaNoch keine Bewertungen
- Jurnal Mata 5Dokument6 SeitenJurnal Mata 5Dahru KinanggaNoch keine Bewertungen
- PIIS0002939422004184Dokument7 SeitenPIIS0002939422004184Anca Florina GaceaNoch keine Bewertungen
- Comparison of Canaloplasty and Trabeculectomy For Open Angle Glaucoma: A Meta-AnalysisDokument6 SeitenComparison of Canaloplasty and Trabeculectomy For Open Angle Glaucoma: A Meta-AnalysisGesti Pratiwi HerlambangNoch keine Bewertungen
- Transient Corneal Edema After Phacoemulsification: Original ArticleDokument5 SeitenTransient Corneal Edema After Phacoemulsification: Original ArticlesarassashaNoch keine Bewertungen
- 1 s2.0 S2452232516302165 MainDokument9 Seiten1 s2.0 S2452232516302165 MainIndah Nur LathifahNoch keine Bewertungen
- Development and Evaluation of A Measure of Patient-Reported Symptoms of BlepharitisDokument6 SeitenDevelopment and Evaluation of A Measure of Patient-Reported Symptoms of BlepharitisYulia MagdalenaNoch keine Bewertungen
- Blepharochalasis: Clinical and Epidemiological Characteristics, Surgical Strategy and Prognosis - A Retrospective Cohort Study With 93 CasesDokument7 SeitenBlepharochalasis: Clinical and Epidemiological Characteristics, Surgical Strategy and Prognosis - A Retrospective Cohort Study With 93 CasesSaqar SharepourNoch keine Bewertungen
- The Central Vein Oclussion Study - Baseline and Early Natural History ReportDokument9 SeitenThe Central Vein Oclussion Study - Baseline and Early Natural History ReportAlan Gaytan LNoch keine Bewertungen
- Therapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismDokument7 SeitenTherapeutic Effectiveness of Toric Implantable Collamer Lens in Treating Ultrahigh Myopic AstigmatismStephanie PfengNoch keine Bewertungen
- Effects of Orthokeratology On The Progression of Low To Moderate Myopia in Chinese ChildrenDokument8 SeitenEffects of Orthokeratology On The Progression of Low To Moderate Myopia in Chinese ChildrenOtniel GeofanoNoch keine Bewertungen
- Evaluation of Umbilical Cord Serum Therapy in Acute Ocular Chemical BurnsDokument6 SeitenEvaluation of Umbilical Cord Serum Therapy in Acute Ocular Chemical BurnsDebby Astasya AnnisaNoch keine Bewertungen
- Comparison of Two Transconjunctival and Transcutaneous Approaches in The Incidence of Scleral Show During Lower Eyelid BlepharoplastyDokument6 SeitenComparison of Two Transconjunctival and Transcutaneous Approaches in The Incidence of Scleral Show During Lower Eyelid BlepharoplastyBobby KristiantoNoch keine Bewertungen
- Myopia Control During Orthokeratology Lens Wear in Children Using A Novel Study DesignDokument11 SeitenMyopia Control During Orthokeratology Lens Wear in Children Using A Novel Study DesignLisa WidiasmokoNoch keine Bewertungen
- Eye 2011154 ADokument7 SeitenEye 2011154 AAmba PutraNoch keine Bewertungen
- The Role of Head Elevation in Treatment of Vitreous HaemorrhageDokument7 SeitenThe Role of Head Elevation in Treatment of Vitreous HaemorrhageMuhammad Imam NoorNoch keine Bewertungen
- Rajavi 2015Dokument7 SeitenRajavi 2015Sherry CkyNoch keine Bewertungen
- 15 DaysDokument9 Seiten15 DayshersainaNoch keine Bewertungen
- Phacoemulsification Versus Manual Small Incision Cataract Surgery in Patients With Fuchs Heterochromic IridocyclitisDokument5 SeitenPhacoemulsification Versus Manual Small Incision Cataract Surgery in Patients With Fuchs Heterochromic IridocyclitisMichael Christopher KadangNoch keine Bewertungen
- Michael Chuka OkosaDokument5 SeitenMichael Chuka OkosaKaisun TeoNoch keine Bewertungen
- F (GH) PF1 (VsuGH)Dokument5 SeitenF (GH) PF1 (VsuGH)Vijay KautilyaNoch keine Bewertungen
- Monovision Lasik in Emmetropic Presbyopic PatientsDokument7 SeitenMonovision Lasik in Emmetropic Presbyopic PatientsIvana Ester Sinta UliNoch keine Bewertungen
- Reliability and Validity of The Ocular Surface Disease IndexDokument7 SeitenReliability and Validity of The Ocular Surface Disease Indexpompoo posmmspNoch keine Bewertungen
- Clinical Features of Herpes Simplex Keratitis in A Korean Tertiary Referral Center: Efficacy of Oral Antiviral and Ascorbic Acid On RecurrenceDokument8 SeitenClinical Features of Herpes Simplex Keratitis in A Korean Tertiary Referral Center: Efficacy of Oral Antiviral and Ascorbic Acid On RecurrenceGiorgos MousterisNoch keine Bewertungen
- Surgical Intervention of Periocular Infantile Hemangiomas in the Era of β-BlockersDokument4 SeitenSurgical Intervention of Periocular Infantile Hemangiomas in the Era of β-BlockersLuisa Fernanda ArboledaNoch keine Bewertungen
- Ni Hms 436399Dokument18 SeitenNi Hms 436399Devanti EkaNoch keine Bewertungen
- Glaucoma After Congenital Cataract SurgeryDokument6 SeitenGlaucoma After Congenital Cataract SurgerySamawi RamudNoch keine Bewertungen
- Single-Step Transepithelial PHDokument9 SeitenSingle-Step Transepithelial PHlenniNoch keine Bewertungen
- Original Article Limbal Ischemia: Reliability of Clinical Assessment and Implications in The Management of Ocular BurnsDokument5 SeitenOriginal Article Limbal Ischemia: Reliability of Clinical Assessment and Implications in The Management of Ocular BurnsJosé Eduardo Zaragoza LópezNoch keine Bewertungen
- Comparison of A Preservative Free Nonsteroidal.Dokument7 SeitenComparison of A Preservative Free Nonsteroidal.Danty IndriastutyNoch keine Bewertungen
- Effectiveness and Safety of The Clareon Monofocal Intraocular Lens: Outcomes From A 12-Month Single-Arm Clinical Study in A Large SampleDokument11 SeitenEffectiveness and Safety of The Clareon Monofocal Intraocular Lens: Outcomes From A 12-Month Single-Arm Clinical Study in A Large SampleHariom ShuklaNoch keine Bewertungen
- Jurnal 2Dokument5 SeitenJurnal 2Asniar RNoch keine Bewertungen
- Clinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsDokument6 SeitenClinical Study: XEN Glaucoma Implant With Mitomycin C 1-Year Follow-Up: Result and ComplicationsAldoNoch keine Bewertungen
- Research ArticleDokument7 SeitenResearch ArticlePhei Qing TjangNoch keine Bewertungen
- Ebn RugayDokument6 SeitenEbn RugayJeffrey Barcelon TanglaoNoch keine Bewertungen
- Glaukoma Setelah Operasi Katarak KongenitalDokument21 SeitenGlaukoma Setelah Operasi Katarak KongenitalAgustianeMawarniAlyNoch keine Bewertungen
- Epilepsia - 2023 - SmithDokument9 SeitenEpilepsia - 2023 - SmithYenny MaharaniNoch keine Bewertungen
- One-Year Results of Health-Related and Vision-Related Quality of Life After Clear Lens Extraction and Multifocal Intraocular Lens ImplantationDokument5 SeitenOne-Year Results of Health-Related and Vision-Related Quality of Life After Clear Lens Extraction and Multifocal Intraocular Lens ImplantationDanty IndriastutyNoch keine Bewertungen
- Pawar 2014Dokument7 SeitenPawar 2014Dinda SaviraNoch keine Bewertungen
- Editorial: The Management of Retinal Detachment: Techniques and PerspectivesDokument3 SeitenEditorial: The Management of Retinal Detachment: Techniques and PerspectivesSarahNoch keine Bewertungen
- Jogi - Basic Ophthalmology, 4th Edition (Ussama Maqbool)Dokument7 SeitenJogi - Basic Ophthalmology, 4th Edition (Ussama Maqbool)pipikafiyaNoch keine Bewertungen
- Medical Management of in Children: A Delphi Consensus: BlepharokeratoconjunctivitisDokument8 SeitenMedical Management of in Children: A Delphi Consensus: Blepharokeratoconjunctivitisriskab123Noch keine Bewertungen
- Scheimpflug Corneal Densitometry Changes After TrabeculectomyDokument7 SeitenScheimpflug Corneal Densitometry Changes After TrabeculectomyFernando MartínezNoch keine Bewertungen
- Jurnal New3Dokument9 SeitenJurnal New3Nurul Qomariah TNoch keine Bewertungen
- Amniotic Membrane Transplantation As An Adjunct To Medical Therapy in Acute Ocular BurnsDokument8 SeitenAmniotic Membrane Transplantation As An Adjunct To Medical Therapy in Acute Ocular BurnsDebby Astasya AnnisaNoch keine Bewertungen
- Jurnal 4Dokument8 SeitenJurnal 4Putri kartiniNoch keine Bewertungen
- The Visual Evoked Potential in Glaucoma and Ocular Hypertension: Effects of Check Size, Field Size, and Stimulation RateDokument9 SeitenThe Visual Evoked Potential in Glaucoma and Ocular Hypertension: Effects of Check Size, Field Size, and Stimulation RateBianca AdelinaNoch keine Bewertungen
- A Comparison of Laser Photocoagulation With Cryotherapy For Threshold Retinopathy of Prematurity at 10 Years Part 2. Refractive OutcomeDokument6 SeitenA Comparison of Laser Photocoagulation With Cryotherapy For Threshold Retinopathy of Prematurity at 10 Years Part 2. Refractive OutcomeSalma HamdyNoch keine Bewertungen
- 10 1097@MD 0000000000008003Dokument6 Seiten10 1097@MD 0000000000008003asfwegereNoch keine Bewertungen
- The Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersVon EverandThe Actions and Uses of Ophthalmic Drugs: A Textbook for Students and PractitionersNoch keine Bewertungen
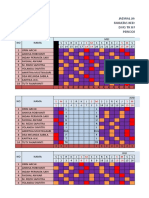
- Jadwal Jaga Kepaniteraan Anak Fakultas Kedokteran Universitas Yarsi Di Rs TK Ii Moh Ridwan Meuraksa Periode 13 Mei - 27 Juli 2019Dokument5 SeitenJadwal Jaga Kepaniteraan Anak Fakultas Kedokteran Universitas Yarsi Di Rs TK Ii Moh Ridwan Meuraksa Periode 13 Mei - 27 Juli 2019Dea Melinda SabilaNoch keine Bewertungen
- The Antipyretic Efficacy and Safety of Propacetamol Compared With Dexibuprofen PDFDokument7 SeitenThe Antipyretic Efficacy and Safety of Propacetamol Compared With Dexibuprofen PDFDea Melinda SabilaNoch keine Bewertungen
- Jurnal: Efikasi Kombinasi Artesunate-Amodiaquine Pada Pengobatan Malaria Falciparum Tanpa Komplikasi Di MadagaskarDokument26 SeitenJurnal: Efikasi Kombinasi Artesunate-Amodiaquine Pada Pengobatan Malaria Falciparum Tanpa Komplikasi Di MadagaskarDea Melinda SabilaNoch keine Bewertungen
- Presentasi Kasus Ppok: Oleh: Annisa Robiyanti 1102011038 Dea Melinda Sabila 1102013072 Pembimbing: DR - Endah A. SP.PDokument3 SeitenPresentasi Kasus Ppok: Oleh: Annisa Robiyanti 1102011038 Dea Melinda Sabila 1102013072 Pembimbing: DR - Endah A. SP.PDea Melinda SabilaNoch keine Bewertungen
- Jurnal Fix IpdDokument4 SeitenJurnal Fix IpdDea Melinda SabilaNoch keine Bewertungen
- Laparoscopic Versus Open Transhiatal Esophagectomy For Distal and Junction CancerDokument6 SeitenLaparoscopic Versus Open Transhiatal Esophagectomy For Distal and Junction CancerDea Melinda SabilaNoch keine Bewertungen
- Surat Sponsor Orang TuaDokument1 SeiteSurat Sponsor Orang TuaDea Melinda SabilaNoch keine Bewertungen
- Chemical Bath DepositionDokument6 SeitenChemical Bath DepositionJune AlapaNoch keine Bewertungen
- 2022 Specimen Paper 1 Mark Scheme 1Dokument4 Seiten2022 Specimen Paper 1 Mark Scheme 1Herman HermanNoch keine Bewertungen
- 2019 MIPS Quality Historic BenchmarksDokument158 Seiten2019 MIPS Quality Historic BenchmarksJoe GellatlyNoch keine Bewertungen
- Nestle SWOT AnalysisDokument3 SeitenNestle SWOT AnalysisMubeen AbdulshakoorNoch keine Bewertungen
- Our School Broke Up For The Winter VacationsDokument7 SeitenOur School Broke Up For The Winter VacationsprinceNoch keine Bewertungen
- MKRS Training ProfileDokument10 SeitenMKRS Training ProfileZafri MKRS100% (1)
- 100G OTN Muxponder: Cost-Efficient Transport of 10x10G Over 100G in Metro NetworksDokument2 Seiten100G OTN Muxponder: Cost-Efficient Transport of 10x10G Over 100G in Metro NetworkshasNoch keine Bewertungen
- Single Nozzle Air-Jet LoomDokument7 SeitenSingle Nozzle Air-Jet LoomRakeahkumarDabkeyaNoch keine Bewertungen
- Snapping TurtleDokument1 SeiteSnapping Turtleapi-379174072Noch keine Bewertungen
- Provisional Restorations in Fixed ProsthodonticsDokument4 SeitenProvisional Restorations in Fixed ProsthodonticsPhoebe David100% (1)
- MHR PreCal 12 Textbook CH 1 SolutionsDokument57 SeitenMHR PreCal 12 Textbook CH 1 SolutionsBryan LowNoch keine Bewertungen
- Animal Cells PDFDokument4 SeitenAnimal Cells PDFFalah HabibNoch keine Bewertungen
- Cug, Ugdp, Pag-Asa, NurseryDokument5 SeitenCug, Ugdp, Pag-Asa, NurseryRaymund Joshua Pre�aNoch keine Bewertungen
- HOconsDokument14 SeitenHOconsMax PradoNoch keine Bewertungen
- Aakash Zoology Study Package 3 SolutionsssssssDokument104 SeitenAakash Zoology Study Package 3 SolutionsssssssRishika PaulNoch keine Bewertungen
- Designing New Vanillin Schiff Bases and Their Antibacterial StudiesDokument4 SeitenDesigning New Vanillin Schiff Bases and Their Antibacterial StudiesAvinash PurohitNoch keine Bewertungen
- What Is Kpag?: Table of ContentsDokument2 SeitenWhat Is Kpag?: Table of Contentsangelito bernalNoch keine Bewertungen
- Crane Inspection ChecklistDokument1 SeiteCrane Inspection ChecklistsudhakarNoch keine Bewertungen
- ClimateDokument38 SeitenClimateCristine CaguiatNoch keine Bewertungen
- Comprensión Lectora en Inglés Clecv Plus 3: Unit 11: The Natural World Unit 12: Music: Influence and InnovationDokument66 SeitenComprensión Lectora en Inglés Clecv Plus 3: Unit 11: The Natural World Unit 12: Music: Influence and InnovationJorge Talavera AnayaNoch keine Bewertungen
- Naskah Drama Beauty and The BeastDokument39 SeitenNaskah Drama Beauty and The BeastAyu Rose75% (4)
- Apexification Using Different Approaches - Case Series Report With A Brief Literature ReviewDokument12 SeitenApexification Using Different Approaches - Case Series Report With A Brief Literature ReviewIJAR JOURNALNoch keine Bewertungen
- AlasDokument3 SeitenAlasdara HinariNoch keine Bewertungen
- Question Bank For Chapter#6Dokument11 SeitenQuestion Bank For Chapter#6krishnam rajuNoch keine Bewertungen