Das könnte Ihnen auch gefallen
- Eric Liou Contributions PDFDokument8 SeitenEric Liou Contributions PDFteju patneediNoch keine Bewertungen
- DentistryDokument1 SeiteDentistryKevin QuintanillaNoch keine Bewertungen
- IVOJI-Contemporary Management of AnDokument8 SeitenIVOJI-Contemporary Management of AnivojiNoch keine Bewertungen
- Guidelines For The Orthodontic Management of The Traumatised ToothDokument8 SeitenGuidelines For The Orthodontic Management of The Traumatised ToothSaumya SinghNoch keine Bewertungen
- Wjoud 2017 08 343Dokument8 SeitenWjoud 2017 08 343meghaNoch keine Bewertungen
- Amo OsDokument5 SeitenAmo OsSooraj SNoch keine Bewertungen
- Curs DR TroianiDokument1 SeiteCurs DR TroianirfandreiNoch keine Bewertungen
- Implant ArticleDokument20 SeitenImplant ArticleArun PrasadNoch keine Bewertungen
- On A of The Appropriate Timing For Surgical Intervention in Orthognathic SurgeryDokument10 SeitenOn A of The Appropriate Timing For Surgical Intervention in Orthognathic SurgeryKira LagoNoch keine Bewertungen
- Orthodontic Books CollectionDokument4 SeitenOrthodontic Books CollectionRamzi ghalipNoch keine Bewertungen
- 0 Orthotics Bhargava Et Al 2023Dokument11 Seiten0 Orthotics Bhargava Et Al 2023David MonroyNoch keine Bewertungen
- Orthodntics MicroimplantsDokument11 SeitenOrthodntics Microimplantsdruzair007Noch keine Bewertungen
- Evaluation of The Association of Lips Competency With Different Skeletal, Dental, and Soft Tissue Components of The Face in The RaichurPopulationDokument4 SeitenEvaluation of The Association of Lips Competency With Different Skeletal, Dental, and Soft Tissue Components of The Face in The RaichurPopulationInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- 1 s2.0 S2468785522003457 MainDokument6 Seiten1 s2.0 S2468785522003457 MainDANTE DELEGUERYNoch keine Bewertungen
- Liou JOMS I 2011Dokument10 SeitenLiou JOMS I 2011dra.merchealbaNoch keine Bewertungen
- Interim Prosthetic Phase of Multidisciplinary Management of Cleidocranial Dysplasia: "The Bronx Approach"Dokument6 SeitenInterim Prosthetic Phase of Multidisciplinary Management of Cleidocranial Dysplasia: "The Bronx Approach"Akanksha MahajanNoch keine Bewertungen
- Renton Forum Implantologicum 9-2 en 1308076Dokument6 SeitenRenton Forum Implantologicum 9-2 en 1308076Franz Willman Chiguala MixanNoch keine Bewertungen
- 1 s2.0 S246878552200338X MainDokument7 Seiten1 s2.0 S246878552200338X MainJuliana ÁlvarezNoch keine Bewertungen
- Management of Deep BiteDokument125 SeitenManagement of Deep BiteAjay ChhetriNoch keine Bewertungen
- Current Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDokument10 SeitenCurrent Practice For Transverse Mandibular and Maxillary Discrepancies in The NetherlandsDONGXU LIUNoch keine Bewertungen
- Reference 1Dokument9 SeitenReference 1sssrao575Noch keine Bewertungen
- Recommendations On The Use of Oral Orthotic Occlusal Appliance Therapý For TMJDokument11 SeitenRecommendations On The Use of Oral Orthotic Occlusal Appliance Therapý For TMJAngie HernándezNoch keine Bewertungen
- Influence of Orthodontic Appliance-Derived Artifacts On 3-T MRI MoviesDokument9 SeitenInfluence of Orthodontic Appliance-Derived Artifacts On 3-T MRI MoviesCelso Antonio Paredes TéllezNoch keine Bewertungen
- Preparation and Evaluation of Orthodontic Setup PDFDokument20 SeitenPreparation and Evaluation of Orthodontic Setup PDFLiezty VioLen'sNoch keine Bewertungen
- Comparison of Osseous Healing After Sagittal Split Ramus Osteotomy and Intraoral Vertical Ramus OsteotomyDokument6 SeitenComparison of Osseous Healing After Sagittal Split Ramus Osteotomy and Intraoral Vertical Ramus OsteotomySoal KoasNoch keine Bewertungen
- Boyd, Robert - Treatment of Deep and Open Bite With Clear AlignersDokument27 SeitenBoyd, Robert - Treatment of Deep and Open Bite With Clear Alignerstravolta0Noch keine Bewertungen
- 3D Diagnosis and Treatment Planning in Orthodontics: An Atlas for the ClinicianVon Everand3D Diagnosis and Treatment Planning in Orthodontics: An Atlas for the ClinicianJean-Marc RetrouveyNoch keine Bewertungen
- Association Between Incisor Positions and Amount of Interdental Stripping in Patients Undergoing Orthodontic TreatmentDokument10 SeitenAssociation Between Incisor Positions and Amount of Interdental Stripping in Patients Undergoing Orthodontic TreatmentJean-Philippe MercierNoch keine Bewertungen
- Comparing Clinical Efficacy of Orthodontic TechniquesDokument14 SeitenComparing Clinical Efficacy of Orthodontic TechniquesNataliaNoch keine Bewertungen
- Screenshot 2022-12-22 at 6.21.43 PMDokument80 SeitenScreenshot 2022-12-22 at 6.21.43 PMdr.teethdentalclinic2019Noch keine Bewertungen
- An Overview of The Surgical Correction of Dentofacial DeformityDokument9 SeitenAn Overview of The Surgical Correction of Dentofacial DeformityAhmad AssariNoch keine Bewertungen
- 2018 3D Family BrochureDokument27 Seiten2018 3D Family BrochureSam Al AbabNoch keine Bewertungen
- J Odw 2016 11 006Dokument6 SeitenJ Odw 2016 11 006Ahmed ElsharkawyNoch keine Bewertungen
- AlNowaisser Et AlDokument4 SeitenAlNowaisser Et AlMishellKarelisMorochoSegarraNoch keine Bewertungen
- Piezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegeDokument36 SeitenPiezosurgery: By, Prathusha.U CRI Department of Public Health Dentistry Chettinad Dental CollegePrathusha Umakhanth100% (1)
- Mini-Implant Corrects Deep OverbiteDokument9 SeitenMini-Implant Corrects Deep OverbiteAnurtha AnuNoch keine Bewertungen
- Junior Prosthodontics III AIDM SGDokument16 SeitenJunior Prosthodontics III AIDM SGbenrejebyahiaNoch keine Bewertungen
- Adult bimaxillary protrusion treated with corticotomyDokument9 SeitenAdult bimaxillary protrusion treated with corticotomyMuruganandam EswaranNoch keine Bewertungen
- Comparing Flap Designs for Impacted Tooth RemovalDokument6 SeitenComparing Flap Designs for Impacted Tooth RemovalArindam DuttaNoch keine Bewertungen
- Dentos Mi Catalogue 2014Dokument20 SeitenDentos Mi Catalogue 2014chorzesiaNoch keine Bewertungen
- Dentos Mi Catalogue 2014Dokument20 SeitenDentos Mi Catalogue 2014chorzesiaNoch keine Bewertungen
- APOSTrendsOrthod75230-7177823 195618Dokument12 SeitenAPOSTrendsOrthod75230-7177823 195618abeNoch keine Bewertungen
- 2016 Issue 1Dokument86 Seiten2016 Issue 1Fareesha KhanNoch keine Bewertungen
- The Surgery-First Orthognathic Approach: With discussion of occlusal plane-altering orthognathic surgeryVon EverandThe Surgery-First Orthognathic Approach: With discussion of occlusal plane-altering orthognathic surgeryNoch keine Bewertungen
- Association Between Incisor Positions and Amount of Interdental Stripping in Patients Undergoing Orthodontic Treatment-1Dokument10 SeitenAssociation Between Incisor Positions and Amount of Interdental Stripping in Patients Undergoing Orthodontic Treatment-1Aly OsmanNoch keine Bewertungen
- A Survey of Orthodontic Treatment in Team Care For Patients With Syndromic Craniosynostosis in JapanDokument8 SeitenA Survey of Orthodontic Treatment in Team Care For Patients With Syndromic Craniosynostosis in Japansaja IssaNoch keine Bewertungen
- Interdisciplinary Management of An Orthodontic Patient With Temporomandibular DisorderDokument12 SeitenInterdisciplinary Management of An Orthodontic Patient With Temporomandibular DisorderMiguel Walter Ramón NeyraNoch keine Bewertungen
- Interferences, Centric Occlusion, ImplantsDokument35 SeitenInterferences, Centric Occlusion, ImplantsDuncan MakNoch keine Bewertungen
- Journal of Cranio-Maxillo-Facial Surgery: Mohammad Zandi, Amirfarhang Miresmaeili, Ali HeidariDokument6 SeitenJournal of Cranio-Maxillo-Facial Surgery: Mohammad Zandi, Amirfarhang Miresmaeili, Ali HeidariYeraldin EspañaNoch keine Bewertungen
- Spurrier 1990Dokument5 SeitenSpurrier 1990Andres CoboNoch keine Bewertungen
- Comparison of Orthodontic Space Closure Using Micro-Osteoperforation and Passive Self-Ligating Appliances or Conventional Fixed Appliances: A Randomized Controlled TrialDokument6 SeitenComparison of Orthodontic Space Closure Using Micro-Osteoperforation and Passive Self-Ligating Appliances or Conventional Fixed Appliances: A Randomized Controlled TrialakNoch keine Bewertungen
- Cone BeamDokument4 SeitenCone BeamESTEBAN RODRIGO CUELLAR TORRESNoch keine Bewertungen
- Paediatric Laser Dentistry. Part 3: Dental Trauma: Laser in Dental Traumatology: Hard Tissues and PulpDokument4 SeitenPaediatric Laser Dentistry. Part 3: Dental Trauma: Laser in Dental Traumatology: Hard Tissues and PulpbaridinoNoch keine Bewertungen
- Different Types of Occlusal Splint Used in Management of Temporomandibular Joint Disorders-A ReviewDokument8 SeitenDifferent Types of Occlusal Splint Used in Management of Temporomandibular Joint Disorders-A ReviewnomanNoch keine Bewertungen
- Load Distribution On Abutment Tooth, Implant and Residual Ridge With Distal-Extension Implant-Supported Removable Partial DentureDokument7 SeitenLoad Distribution On Abutment Tooth, Implant and Residual Ridge With Distal-Extension Implant-Supported Removable Partial DenturedentureNoch keine Bewertungen
- Best Orthopedic Doctor in VisakhapatnamDokument4 SeitenBest Orthopedic Doctor in VisakhapatnamPrathyusha PulamarasettiNoch keine Bewertungen
- Comparison of orthodontic space closure using micro-osteoperforation and passive self-ligating appliances or conventional fixed appliances: A randomized controlled trialDokument6 SeitenComparison of orthodontic space closure using micro-osteoperforation and passive self-ligating appliances or conventional fixed appliances: A randomized controlled trialDiana ElíasNoch keine Bewertungen
- Restoring a Fractured Front ToothDokument8 SeitenRestoring a Fractured Front ToothIbramanto WarganegaraNoch keine Bewertungen
- Two - and Three-Dimensional Orthodontic Imaging UsingDokument9 SeitenTwo - and Three-Dimensional Orthodontic Imaging UsingElzaMMartinsNoch keine Bewertungen
- Comparison PiezoDokument13 SeitenComparison PiezoMiguel ChanNoch keine Bewertungen
- Diagnostic Criteria Examination Form PDFDokument2 SeitenDiagnostic Criteria Examination Form PDFNor Nadia Zakaria50% (2)
- Extraction of The Deciduous Canine As An Interceptive Treatment in Children With Palatal Displaced Canines-Part I: Shall We Extract The Deciduous Canine or Not?Dokument10 SeitenExtraction of The Deciduous Canine As An Interceptive Treatment in Children With Palatal Displaced Canines-Part I: Shall We Extract The Deciduous Canine or Not?Nor Nadia ZakariaNoch keine Bewertungen
- Diagnostic Criteria Decision Tree PDFDokument2 SeitenDiagnostic Criteria Decision Tree PDFNor Nadia ZakariaNoch keine Bewertungen
- An Audit of The Turnaround Time of Fixed Prosthodontics Cases in The Ceramic LaboratoryDokument8 SeitenAn Audit of The Turnaround Time of Fixed Prosthodontics Cases in The Ceramic LaboratoryNor Nadia ZakariaNoch keine Bewertungen
- ASTM G1 Standard PracticeDokument8 SeitenASTM G1 Standard PracticeHeri SusantoNoch keine Bewertungen
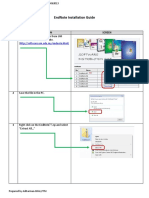
- Endnote X7 Installation GuideDokument5 SeitenEndnote X7 Installation GuideNor Nadia ZakariaNoch keine Bewertungen
- Hiv 2006Dokument11 SeitenHiv 2006Nor Nadia ZakariaNoch keine Bewertungen
- Infection ControlDokument52 SeitenInfection ControlNor Nadia ZakariaNoch keine Bewertungen
- Goblet CellDokument4 SeitenGoblet CellMuhammad ZairulfikriNoch keine Bewertungen
- Mini Question Bank - Vety Sci - For Students PDFDokument106 SeitenMini Question Bank - Vety Sci - For Students PDFRakesh Prajapati100% (3)
- Doctors Roadmap To The UkDokument10 SeitenDoctors Roadmap To The Uksryh2012Noch keine Bewertungen
- 5 Weeks To 5km Beginner and Intermediate PDFDokument1 Seite5 Weeks To 5km Beginner and Intermediate PDFMutsai MusaNoch keine Bewertungen
- The Welfare of Cattle Kept For Beef ProductionDokument150 SeitenThe Welfare of Cattle Kept For Beef ProductionIsabel CarrilloNoch keine Bewertungen
- PCRL 627: Clinical Microbiology and Immunology 2016: Email: Shilling@uic - EduDokument45 SeitenPCRL 627: Clinical Microbiology and Immunology 2016: Email: Shilling@uic - Edui24youNoch keine Bewertungen
- Ocurest Plus2018Dokument4 SeitenOcurest Plus2018rotastrainNoch keine Bewertungen
- Jodi Halpern - From Detached Concern To EmpathyDokument188 SeitenJodi Halpern - From Detached Concern To Empathycobby174100% (1)
- 01 1 PDFDokument8 Seiten01 1 PDFpravikumar1989Noch keine Bewertungen
- De Gruchys Clinical Haematology PDFDokument1 SeiteDe Gruchys Clinical Haematology PDFShivanshi K0% (1)
- Hospital Job DescriptionsDokument48 SeitenHospital Job DescriptionsLoresita Amoranto Rebong RNNoch keine Bewertungen
- Thulium e Alopecia AndrogenéticaDokument9 SeitenThulium e Alopecia AndrogenéticacristianneNoch keine Bewertungen
- Stress (Biology) : 1 Etymology and Historical UsageDokument19 SeitenStress (Biology) : 1 Etymology and Historical UsageZiedTrikiNoch keine Bewertungen
- Amir Bin Tamin 2Dokument3 SeitenAmir Bin Tamin 2Akram KastiranNoch keine Bewertungen
- MSWORD PronunciationDokument3 SeitenMSWORD PronunciationStephen ThomsonNoch keine Bewertungen
- NCP OrthoDokument2 SeitenNCP OrthoJeyser T. GamutiaNoch keine Bewertungen
- Meier Et Al, 1996Dokument4 SeitenMeier Et Al, 1996boni_sebayangNoch keine Bewertungen
- Epidemiology of AsthmaDokument8 SeitenEpidemiology of AsthmaMaria Alejandra Siachoque JaraNoch keine Bewertungen
- Study The Herbalism of Thyme LeavesDokument7 SeitenStudy The Herbalism of Thyme Leavespronto4meNoch keine Bewertungen
- Not Eligible As No Experience of Teaching and ResearchDokument5 SeitenNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNoch keine Bewertungen
- Diagnostic Test - Pedia With Answer 50 Items Without RatioDokument4 SeitenDiagnostic Test - Pedia With Answer 50 Items Without RatioDennis Nabor Muñoz, RN,RMNoch keine Bewertungen
- Advances in Psychological and Social Support After DisastersDokument149 SeitenAdvances in Psychological and Social Support After DisastersjprewittdiazNoch keine Bewertungen
- Manila Standard Today - Friday (September 14, 2012) IssueDokument22 SeitenManila Standard Today - Friday (September 14, 2012) IssueManila Standard TodayNoch keine Bewertungen
- Cir 0000000000000899Dokument25 SeitenCir 0000000000000899hanifa ambNoch keine Bewertungen
- Principles of Tooth PreparationsDokument14 SeitenPrinciples of Tooth PreparationsMarrion Jules Sequitin MendozaNoch keine Bewertungen
- Post MBBS - Second Round Allotment Details PDFDokument89 SeitenPost MBBS - Second Round Allotment Details PDFRamaniNoch keine Bewertungen
- Angle. Ribbon Arch Introduction 1916Dokument26 SeitenAngle. Ribbon Arch Introduction 1916rrnotholtNoch keine Bewertungen
- Change TalkDokument9 SeitenChange Talkapi-346503081Noch keine Bewertungen
- Anemia: Differential DiagnosisDokument7 SeitenAnemia: Differential DiagnosisZaman MigozaradNoch keine Bewertungen