Das könnte Ihnen auch gefallen
- Hemiarthroplasty For Proximal Humerus FracturesDokument6 SeitenHemiarthroplasty For Proximal Humerus FracturesEllan Giulianno FerreiraNoch keine Bewertungen
- Fatty Infiltration and Atrophy of The Rotator Cuff Do Not Improve After Rotator Cuff Repair and Correlate With Poor Functional Outcome PDFDokument10 SeitenFatty Infiltration and Atrophy of The Rotator Cuff Do Not Improve After Rotator Cuff Repair and Correlate With Poor Functional Outcome PDFEllan Giulianno FerreiraNoch keine Bewertungen
- Distal Triceps RupturesDokument5 SeitenDistal Triceps RupturesEllan Giulianno FerreiraNoch keine Bewertungen
- Difference in Vascular Patterns Between Transosseous-Equivalent and Transosseous Rotator Cuff RepairDokument8 SeitenDifference in Vascular Patterns Between Transosseous-Equivalent and Transosseous Rotator Cuff RepairEllan Giulianno FerreiraNoch keine Bewertungen
- Effects of Glenoid Inclination and Acromion Index On Humeral Head Translation and Glenoid Articular Cartilage StrainDokument8 SeitenEffects of Glenoid Inclination and Acromion Index On Humeral Head Translation and Glenoid Articular Cartilage StrainEllan Giulianno FerreiraNoch keine Bewertungen
- Current Concepts in Elbow ArthroplastyDokument6 SeitenCurrent Concepts in Elbow ArthroplastyEllan Giulianno FerreiraNoch keine Bewertungen
- Economical and Efficacious Beach Chair Traction Positioning For Shoulder ArthrosDokument7 SeitenEconomical and Efficacious Beach Chair Traction Positioning For Shoulder ArthrosEllan Giulianno FerreiraNoch keine Bewertungen
- Evolving Concept of Bipolar Bone Loss and The Hill-Sachs Lesion - From Engaging-Non-Engaging Lesion To On-Track-Off-Track Lesion PDFDokument9 SeitenEvolving Concept of Bipolar Bone Loss and The Hill-Sachs Lesion - From Engaging-Non-Engaging Lesion To On-Track-Off-Track Lesion PDFEllan Giulianno FerreiraNoch keine Bewertungen
- Double-Row, Transosseous-Equivalent Suture-Bridge Repair For Supraspinatus Tears - Power Up The HealingDokument9 SeitenDouble-Row, Transosseous-Equivalent Suture-Bridge Repair For Supraspinatus Tears - Power Up The HealingEllan Giulianno FerreiraNoch keine Bewertungen
- Distal Biceps Tendon InjuriesDokument9 SeitenDistal Biceps Tendon InjuriesEllan Giulianno FerreiraNoch keine Bewertungen
- Coracoclavicular Ligament Reconstruction Using The Lateral Half of The Conjoined TendonDokument5 SeitenCoracoclavicular Ligament Reconstruction Using The Lateral Half of The Conjoined TendonEllan Giulianno FerreiraNoch keine Bewertungen
- Disorders of The Long Head of Biceps TendonDokument10 SeitenDisorders of The Long Head of Biceps TendonEllan Giulianno FerreiraNoch keine Bewertungen
- Complications in Reverse Shoulder ArthroplastyDokument9 SeitenComplications in Reverse Shoulder ArthroplastyEllan Giulianno FerreiraNoch keine Bewertungen
- Contribution of Osseous and Muscular Stabilizing Effects With The Latarjet Procedure For Anterior Instability Without Glenoid Bone LossDokument6 SeitenContribution of Osseous and Muscular Stabilizing Effects With The Latarjet Procedure For Anterior Instability Without Glenoid Bone LossEllan Giulianno FerreiraNoch keine Bewertungen
- Chronic Medial Instability of The ElbowDokument6 SeitenChronic Medial Instability of The ElbowEllan Giulianno FerreiraNoch keine Bewertungen
- Classification of Full-Thickness Rotator Cuff Lesions - A ReviewDokument11 SeitenClassification of Full-Thickness Rotator Cuff Lesions - A ReviewEllan Giulianno FerreiraNoch keine Bewertungen
- Biomechanics of A Novel Technique For Suprapectoral Intraosseous Biceps TenodesisDokument9 SeitenBiomechanics of A Novel Technique For Suprapectoral Intraosseous Biceps TenodesisEllan Giulianno FerreiraNoch keine Bewertungen
- Complex Elbow Instability - Surgical Management of Elbow Fracture DislocationsDokument8 SeitenComplex Elbow Instability - Surgical Management of Elbow Fracture DislocationsEllan Giulianno FerreiraNoch keine Bewertungen
- Biomechanical Evaluation of Two Arthroscopic Techniques For Biceps Tenodesis - Triple Loop Suture Versus Simple SutureDokument5 SeitenBiomechanical Evaluation of Two Arthroscopic Techniques For Biceps Tenodesis - Triple Loop Suture Versus Simple SutureEllan Giulianno FerreiraNoch keine Bewertungen
- Biomechanical Analysis of The Modified Bristow Procedure For Anterior Shoulder Instability - Is The Bone Block NecessaryDokument8 SeitenBiomechanical Analysis of The Modified Bristow Procedure For Anterior Shoulder Instability - Is The Bone Block NecessaryEllan Giulianno FerreiraNoch keine Bewertungen
- Adhesive CapsulitisDokument6 SeitenAdhesive CapsulitisEllan Giulianno FerreiraNoch keine Bewertungen
- A Posterosuperior Approach To The ShoulderDokument5 SeitenA Posterosuperior Approach To The ShoulderEllan Giulianno FerreiraNoch keine Bewertungen
- A Comprehensive Analysis of Pectoralis Major Transfer For Long Thoracic Nerve PalsyDokument11 SeitenA Comprehensive Analysis of Pectoralis Major Transfer For Long Thoracic Nerve PalsyEllan Giulianno FerreiraNoch keine Bewertungen
- Biceps Tenotomy Versus Tenodesis - A Review of Clinical Outcomes and Biomechanical ResultsDokument7 SeitenBiceps Tenotomy Versus Tenodesis - A Review of Clinical Outcomes and Biomechanical ResultsEllan Giulianno FerreiraNoch keine Bewertungen
- A Posterosuperior Approach To The ShoulderDokument5 SeitenA Posterosuperior Approach To The ShoulderEllan Giulianno FerreiraNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Fix Your Caveman Posture in 4 PartsDokument87 SeitenFix Your Caveman Posture in 4 PartsaskofsublimeNoch keine Bewertungen
- Positioning Checklist Revised Mar 3Dokument3 SeitenPositioning Checklist Revised Mar 3Justine Matthew Gavile CoronicaNoch keine Bewertungen
- P90X/P90X2 Hybrid Workout SchedulesDokument3 SeitenP90X/P90X2 Hybrid Workout SchedulesDragouilleNoch keine Bewertungen
- MRI Oblique Views Improve Joint AssessmentDokument53 SeitenMRI Oblique Views Improve Joint AssessmentCristián Martínez BocazNoch keine Bewertungen
- Body MeridianDokument65 SeitenBody Meridiandcf67my100% (1)
- Downward Movement - Left Hand Only: (Figure 3-7Dokument20 SeitenDownward Movement - Left Hand Only: (Figure 3-7mamun31Noch keine Bewertungen
- Trunk Stabilization ProgramDokument20 SeitenTrunk Stabilization ProgramLate ArtistNoch keine Bewertungen
- Clinical Massage Therapy - S. Jurch Hill, 2009) WWDokument562 SeitenClinical Massage Therapy - S. Jurch Hill, 2009) WWMohsen Bt92% (12)
- Fascial Stretch TherapyDokument294 SeitenFascial Stretch TherapyDiana Mariș93% (28)
- Upper/Lower Routine 3-4x Per Week Home WorkoutDokument8 SeitenUpper/Lower Routine 3-4x Per Week Home WorkoutSkate DudeNoch keine Bewertungen
- Revised Curriculum DPT-UHS (15!09!15)Dokument294 SeitenRevised Curriculum DPT-UHS (15!09!15)Iqra Iftikhar50% (2)
- MusculoskeletalDokument373 SeitenMusculoskeletalLoredana Elena Baltariu100% (1)
- TOSSM-APKASS 2020 - Conference ProgramDokument3 SeitenTOSSM-APKASS 2020 - Conference Programfajar alatasNoch keine Bewertungen
- Blades and Burs: Pocket Reference GuideDokument8 SeitenBlades and Burs: Pocket Reference GuideJosé Roberto MuraNoch keine Bewertungen
- Rotator Cuff InjuriesDokument26 SeitenRotator Cuff Injuriesanname_girlNoch keine Bewertungen
- Closed Fracture of Middle ClaviculaDokument12 SeitenClosed Fracture of Middle ClaviculachiciNoch keine Bewertungen
- Cachero vs. Manila Yellow TaxicabDokument5 SeitenCachero vs. Manila Yellow TaxicabMj BrionesNoch keine Bewertungen
- Biomechanics of The Shoulder ComplexDokument83 SeitenBiomechanics of The Shoulder Complexsundar prabhuNoch keine Bewertungen
- Shoulder Exercise Descriptions For BankartDokument10 SeitenShoulder Exercise Descriptions For BankartIlmuddin ApridhantikoNoch keine Bewertungen
- Dub Maddox Throwing MechanicsDokument5 SeitenDub Maddox Throwing MechanicsJerad Bixler100% (1)
- Lumbar Stabilization ProgramDokument4 SeitenLumbar Stabilization ProgramMomchil Pekov100% (1)
- Article 1 - Nantechonology-1Dokument19 SeitenArticle 1 - Nantechonology-1Alexander LuNoch keine Bewertungen
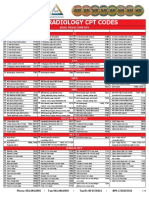
- 2019 Radiology CPT Codes: CT Bone DensitometryDokument2 Seiten2019 Radiology CPT Codes: CT Bone DensitometryDownsyndrome CyborgNoch keine Bewertungen
- The Physics of Fitness - Douglas BrignoleDokument531 SeitenThe Physics of Fitness - Douglas BrignoleПавел Кръстев100% (13)
- Effects of Scapular Stabilization Exercise Training OnDokument12 SeitenEffects of Scapular Stabilization Exercise Training OnNajoua SalomaoNoch keine Bewertungen
- Scapula Fracture ReviewDokument12 SeitenScapula Fracture Reviewakb601Noch keine Bewertungen
- Ministry of Health Price List for Medical ServicesDokument40 SeitenMinistry of Health Price List for Medical ServicesHåíthãm KhãtïßNoch keine Bewertungen
- Surgery (Ortho) NotesDokument155 SeitenSurgery (Ortho) NotesprestigeuniversaltradingNoch keine Bewertungen
- Examination and Investigation of Musculoskeletal SystemDokument15 SeitenExamination and Investigation of Musculoskeletal SystemofficialmidasNoch keine Bewertungen
- Muscles of the Head, Neck, and TrunkDokument8 SeitenMuscles of the Head, Neck, and TrunkJericho CarenaNoch keine Bewertungen