Das könnte Ihnen auch gefallen
- Oba NikoleDokument1 SeiteOba NikoleraudneimNoch keine Bewertungen
- Artigo 41Dokument9 SeitenArtigo 41raudneimNoch keine Bewertungen
- LMP1 Expression Prognostic Biomarker EBV CancersDokument13 SeitenLMP1 Expression Prognostic Biomarker EBV CancersraudneimNoch keine Bewertungen
- Artigo 34Dokument15 SeitenArtigo 34raudneimNoch keine Bewertungen
- Role of EBV, Bcl-2, p53, c-Myc, Rb in NHL PathogenesisDokument5 SeitenRole of EBV, Bcl-2, p53, c-Myc, Rb in NHL PathogenesisraudneimNoch keine Bewertungen
- Artigo 31Dokument14 SeitenArtigo 31raudneimNoch keine Bewertungen
- Artigo 30Dokument7 SeitenArtigo 30raudneimNoch keine Bewertungen
- Artigo 38Dokument8 SeitenArtigo 38raudneimNoch keine Bewertungen
- Artigo 36 PDFDokument9 SeitenArtigo 36 PDFraudneimNoch keine Bewertungen
- Artigo 33Dokument21 SeitenArtigo 33raudneimNoch keine Bewertungen
- Artigo 7 PDFDokument7 SeitenArtigo 7 PDFraudneimNoch keine Bewertungen
- Artigo 22 PDFDokument5 SeitenArtigo 22 PDFraudneimNoch keine Bewertungen
- Artigo 32Dokument8 SeitenArtigo 32raudneimNoch keine Bewertungen
- Role of EBV, Bcl-2, p53, c-Myc, Rb in NHL PathogenesisDokument5 SeitenRole of EBV, Bcl-2, p53, c-Myc, Rb in NHL PathogenesisraudneimNoch keine Bewertungen
- Artigo 29Dokument5 SeitenArtigo 29raudneimNoch keine Bewertungen
- Artigo 21Dokument13 SeitenArtigo 21raudneimNoch keine Bewertungen
- Artigo 19Dokument15 SeitenArtigo 19raudneimNoch keine Bewertungen
- Artigo 21Dokument13 SeitenArtigo 21raudneimNoch keine Bewertungen
- Artigo 20Dokument7 SeitenArtigo 20raudneimNoch keine Bewertungen
- Artigo 16Dokument8 SeitenArtigo 16raudneimNoch keine Bewertungen
- Minireview: Epstein-Barr Virus EntryDokument8 SeitenMinireview: Epstein-Barr Virus EntryraudneimNoch keine Bewertungen
- Artigo 18Dokument8 SeitenArtigo 18raudneimNoch keine Bewertungen
- Enfermedad Linfoproliferativa Difusa Postrasplante en Adultos: Comunicación de Un Caso y Revisión de La LiteraturaDokument4 SeitenEnfermedad Linfoproliferativa Difusa Postrasplante en Adultos: Comunicación de Un Caso y Revisión de La LiteraturaraudneimNoch keine Bewertungen
- Artigo 14Dokument14 SeitenArtigo 14raudneimNoch keine Bewertungen
- Artigo 8Dokument9 SeitenArtigo 8raudneimNoch keine Bewertungen
- Artigo 10Dokument5 SeitenArtigo 10raudneimNoch keine Bewertungen
- Artigo 12Dokument12 SeitenArtigo 12raudneimNoch keine Bewertungen
- Artigo 11Dokument14 SeitenArtigo 11raudneimNoch keine Bewertungen
- Artigo 7 PDFDokument7 SeitenArtigo 7 PDFraudneimNoch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5783)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (587)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (72)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (119)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Understanding Plasma Cell Dyscrasias: MGUS, Myeloma, Waldenstrom's and AmyloidosisDokument41 SeitenUnderstanding Plasma Cell Dyscrasias: MGUS, Myeloma, Waldenstrom's and AmyloidosisDr MonikaNoch keine Bewertungen
- HOW TO USE SACRED CODES FOR HEALING AND PROSPERITYDokument14 SeitenHOW TO USE SACRED CODES FOR HEALING AND PROSPERITYnikanor1100% (2)
- Lecture 12 Cardio Intensive CasesDokument32 SeitenLecture 12 Cardio Intensive Casesraul0% (1)
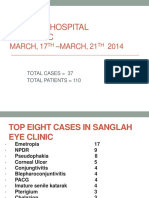
- Sanglah Hospital Eye Clinic: MARCH, 17 - MARCH, 21 2014Dokument25 SeitenSanglah Hospital Eye Clinic: MARCH, 17 - MARCH, 21 2014krisadi30Noch keine Bewertungen
- Respi HemaDokument57 SeitenRespi Hemaniczdelosreyes8Noch keine Bewertungen
- Diarrhea: Types, Causes, and ManagementDokument7 SeitenDiarrhea: Types, Causes, and ManagementWen Jie LauNoch keine Bewertungen
- Maternal & Child Care Nursing ReviewDokument37 SeitenMaternal & Child Care Nursing Reviewɹǝʍdןnos98% (130)
- Chorea, Ataxia,: and Other Movement DisordersDokument35 SeitenChorea, Ataxia,: and Other Movement Disordersyusfi indra gunawanNoch keine Bewertungen
- Case Discussion on Right Hip AVN in a 26-Year-Old LadyDokument12 SeitenCase Discussion on Right Hip AVN in a 26-Year-Old LadyKyaw SwaNoch keine Bewertungen
- NewsRecord15 08 26Dokument24 SeitenNewsRecord15 08 26Kristina HicksNoch keine Bewertungen
- Neuromuscular Junction DisorderDokument10 SeitenNeuromuscular Junction DisorderZosmita Shane GalgaoNoch keine Bewertungen
- Obstructive UropathyDokument3 SeitenObstructive UropathyGerardLum100% (1)
- Goiter Investigation and Management PDFDokument5 SeitenGoiter Investigation and Management PDFjhoey83Noch keine Bewertungen
- Review of Imaging of Brain Naidich AJNRDokument3 SeitenReview of Imaging of Brain Naidich AJNRParthiban BalaNoch keine Bewertungen
- Nursing Licensure Exam Compilation of TipsDokument3 SeitenNursing Licensure Exam Compilation of TipsIkarishinNoch keine Bewertungen
- 4 - LDC Revised Grading of Acute Kidney Injury (1 5)Dokument7 Seiten4 - LDC Revised Grading of Acute Kidney Injury (1 5)kradoNoch keine Bewertungen
- Lecture Lesson 12. Serous, Duodenal, and Gastric FluidDokument4 SeitenLecture Lesson 12. Serous, Duodenal, and Gastric FluidHANA LUNARIANoch keine Bewertungen
- Neuro ReviewerDokument41 SeitenNeuro ReviewerKyla Shain GallegoNoch keine Bewertungen
- Ortho LMRP 2019Dokument44 SeitenOrtho LMRP 2019skNoch keine Bewertungen
- NSAIDSDokument19 SeitenNSAIDSDonna Kelly DuranNoch keine Bewertungen
- About Medical ResearchDokument21 SeitenAbout Medical ResearchMohebNoch keine Bewertungen
- Respiratory Distress SyndromeDokument7 SeitenRespiratory Distress SyndromeBilal RowaihiNoch keine Bewertungen
- Pathophysiology of Cataract 2Dokument8 SeitenPathophysiology of Cataract 2Samuel Wibowo100% (1)
- Medical Prefixes and SuffixesDokument12 SeitenMedical Prefixes and SuffixesKrishnanunni KLNoch keine Bewertungen
- Basics of Autonomic Nervous System Function: Loewy, 1990Dokument12 SeitenBasics of Autonomic Nervous System Function: Loewy, 1990fezaNoch keine Bewertungen
- Ortho NCLEX Questions 1 PDFDokument39 SeitenOrtho NCLEX Questions 1 PDFElizabella Henrietta TanaquilNoch keine Bewertungen
- MegakaryopoiesisDokument41 SeitenMegakaryopoiesisHazel FlorentinoNoch keine Bewertungen
- Endoscopic Evaluation of Aceclofenac Gastrointestinal SafetyDokument11 SeitenEndoscopic Evaluation of Aceclofenac Gastrointestinal SafetyMartin MoranNoch keine Bewertungen
- Echotech Reporting Guidelines Version 15Dokument30 SeitenEchotech Reporting Guidelines Version 15AbrahamNoch keine Bewertungen
- Drug Study For Multiple Sclerosis (Betaseron)Dokument4 SeitenDrug Study For Multiple Sclerosis (Betaseron)Leslie Lagat PaguioNoch keine Bewertungen