Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Mental Health Effects of ObesityDokument7 SeitenMental Health Effects of ObesityMohd FaizNoch keine Bewertungen
- Kanski Clinical Ophthalmology Chapter 3 ORBITDokument43 SeitenKanski Clinical Ophthalmology Chapter 3 ORBITSekar Ayu WulandariNoch keine Bewertungen
- Waxing Full Leg (Final)Dokument5 SeitenWaxing Full Leg (Final)Lionel YdeNoch keine Bewertungen
- Assessment Techniques Normal Findings Abnormal Findings A. Gait InspectionDokument12 SeitenAssessment Techniques Normal Findings Abnormal Findings A. Gait Inspectionshannon c. lewisNoch keine Bewertungen
- Thyroid DisordersDokument104 SeitenThyroid DisordersShashwat Johri100% (1)
- Hematologic DisorderDokument8 SeitenHematologic DisorderRayan AhmedNoch keine Bewertungen
- PAS Kls 5 InggrisDokument2 SeitenPAS Kls 5 Inggriswidya afiyatiNoch keine Bewertungen
- A Machine Learning Perspective: Prediction of Chronic Kidney DiseaseDokument22 SeitenA Machine Learning Perspective: Prediction of Chronic Kidney DiseaseSadiNoch keine Bewertungen
- Disorders of Esophagus and StomachDokument29 SeitenDisorders of Esophagus and StomachSamuel kuriaNoch keine Bewertungen
- Drug Study HaloperidolDokument3 SeitenDrug Study HaloperidolKrizzia FosterNoch keine Bewertungen
- Drug Study (Ceftriaxone)Dokument2 SeitenDrug Study (Ceftriaxone)Keij Araneta93% (15)
- Akut Retina Nekrosis (ARN)Dokument5 SeitenAkut Retina Nekrosis (ARN)Harsianti Yuni YudaNoch keine Bewertungen
- Peter Fraser Using Miasms in Homoeopathy: Reading ExcerptDokument5 SeitenPeter Fraser Using Miasms in Homoeopathy: Reading ExcerptMd AslamNoch keine Bewertungen
- A 17 Year Old With Becker Muscular Dystrophy and UDokument5 SeitenA 17 Year Old With Becker Muscular Dystrophy and UagamerocallejasNoch keine Bewertungen
- Confidential: Iom Minimum Medical Review QuestionnaireDokument3 SeitenConfidential: Iom Minimum Medical Review QuestionnairePochieNoch keine Bewertungen
- BADBREATHDokument23 SeitenBADBREATHBilly TrầnNoch keine Bewertungen
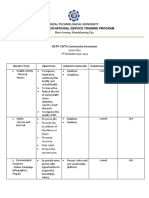
- Rizal Technological University Center For National Service Training ProgramDokument2 SeitenRizal Technological University Center For National Service Training ProgramAbegail CatindigNoch keine Bewertungen
- Yerba BuenaDokument2 SeitenYerba BuenaLloydNoch keine Bewertungen
- Study of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyDokument6 SeitenStudy of Sociodemographic Profile, Maternal, Fetal Outcome in Preeclamptic and Eclamptic Women A Prospective StudyHarvey MatbaganNoch keine Bewertungen
- Ethereal Crystals 1 - 9 Revised ManualDokument52 SeitenEthereal Crystals 1 - 9 Revised ManualBelanitaAbreu100% (1)
- Gaurang - Reportory LectureDokument42 SeitenGaurang - Reportory LectureJayakrishnaNoch keine Bewertungen
- Nephritis Virus in PoultryDokument13 SeitenNephritis Virus in Poultrynasih hamadNoch keine Bewertungen
- RCP - Post Stroke Scalp Acupuncture Research PDFDokument64 SeitenRCP - Post Stroke Scalp Acupuncture Research PDFIstiqomah Flx100% (1)
- 2013 - Conceitos Na Abordagem Da Concussão No Desporto - Abordagem MultidisciplinarDokument9 Seiten2013 - Conceitos Na Abordagem Da Concussão No Desporto - Abordagem MultidisciplinarLuis Miguel MartinsNoch keine Bewertungen
- Test - Report 24 - 01 - 2022Dokument3 SeitenTest - Report 24 - 01 - 2022Habib Ur RahmanNoch keine Bewertungen
- Familial Dilated Cardiomyopathy of Young Portuguese Water DogsDokument9 SeitenFamilial Dilated Cardiomyopathy of Young Portuguese Water DogsJessareth Atilano CapacioNoch keine Bewertungen
- ReportDokument10 SeitenReportAnkita GoyalNoch keine Bewertungen
- Coronavirus Disease (Covid-19) : Mandatory QuarantineDokument2 SeitenCoronavirus Disease (Covid-19) : Mandatory QuarantineNinya PileNoch keine Bewertungen
- Childwell Training - Food Hygiene Level 2 Course ManualDokument14 SeitenChildwell Training - Food Hygiene Level 2 Course ManualJohnNoch keine Bewertungen
- Stomach-Esophagus MedCosmos Surgery - MCQDokument39 SeitenStomach-Esophagus MedCosmos Surgery - MCQMike G100% (1)