Das könnte Ihnen auch gefallen
- Stent Graft Versus Balloon Angioplasty For Failing Dialysis-Access GraftsDokument10 SeitenStent Graft Versus Balloon Angioplasty For Failing Dialysis-Access GraftsAra wildhaNoch keine Bewertungen
- Fana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Dokument8 SeitenFana Alemseged Endovascular Thrombectomy For Basil - 231118 - 114208Luis Guilherme ScalianteNoch keine Bewertungen
- Tonino 2009Dokument12 SeitenTonino 2009Paul CalbureanNoch keine Bewertungen
- PAD III TrialDokument8 SeitenPAD III TrialMary IvojdaNoch keine Bewertungen
- Articles: BackgroundDokument12 SeitenArticles: BackgroundJoshua BensonNoch keine Bewertungen
- Catheter Ablation in End Stage Heart FailureDokument10 SeitenCatheter Ablation in End Stage Heart FailureJose Gomez MorenoNoch keine Bewertungen
- Nej M Abbotts TentDokument11 SeitenNej M Abbotts TentWKYC.comNoch keine Bewertungen
- Pci Versus Cabg in Cad, Serruys (2009)Dokument12 SeitenPci Versus Cabg in Cad, Serruys (2009)Henrique MachadoNoch keine Bewertungen
- Fa y StrokeDokument11 SeitenFa y StrokeCatherine Galdames HinojosaNoch keine Bewertungen
- Metaanalisis FD en Agudo Ajnr 223 Pacientes CagnazoDokument7 SeitenMetaanalisis FD en Agudo Ajnr 223 Pacientes CagnazoangelNoch keine Bewertungen
- Lemus Rangel 2010Dokument2 SeitenLemus Rangel 2010audiNoch keine Bewertungen
- Minimally Invasive Cardiac Surgery: A Safe Alternative For Aortic Valve Replacement?Dokument2 SeitenMinimally Invasive Cardiac Surgery: A Safe Alternative For Aortic Valve Replacement?lkulacogluNoch keine Bewertungen
- Early Use of TIPS in Cirrhosis and Variceal BleedingDokument10 SeitenEarly Use of TIPS in Cirrhosis and Variceal Bleedingray liNoch keine Bewertungen
- Trial of Endovasculr Treatment of Acute Basilar Artery OcclusionDokument12 SeitenTrial of Endovasculr Treatment of Acute Basilar Artery OcclusionVictorNoch keine Bewertungen
- Castle AfDokument11 SeitenCastle AfgustavoNoch keine Bewertungen
- Percutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaDokument6 SeitenPercutaneous Transluminal Angioplasty and Stenting As First-Choice Treatment in Patients With Chronic Mesenteric IschemiaCotaga IgorNoch keine Bewertungen
- The Barrow Ruptured Aneurysm Trial - 6-Year ResultsDokument9 SeitenThe Barrow Ruptured Aneurysm Trial - 6-Year ResultsJulieta PereyraNoch keine Bewertungen
- Safety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaDokument9 SeitenSafety and Ef Ficacy of An Endovascular-First Approach To Acute Limb IschemiaSisca Dwi AgustinaNoch keine Bewertungen
- Catheter Ablationin in AF With CHFDokument11 SeitenCatheter Ablationin in AF With CHFKristian Sudana HartantoNoch keine Bewertungen
- Aspirine Vs LMWH Nejm2023Dokument11 SeitenAspirine Vs LMWH Nejm2023Esteban DavidNoch keine Bewertungen
- Closure of Patent Foramen Ovale Versus Medical Therapy After Cryptogenic StrokeDokument9 SeitenClosure of Patent Foramen Ovale Versus Medical Therapy After Cryptogenic StrokelaurasheerNoch keine Bewertungen
- Record 1 - THRDokument11 SeitenRecord 1 - THRNorhamdan Mohd YahayaNoch keine Bewertungen
- Stich IDokument11 SeitenStich IKevin Mora BañosNoch keine Bewertungen
- Long-Term Outcome After Thrombolysis For Acute Lower Limb IschaemiaDokument9 SeitenLong-Term Outcome After Thrombolysis For Acute Lower Limb IschaemiaIdham Adyasa Manggala PutraNoch keine Bewertungen
- Evolving Approaches To The Iliacs, Femorals, Popliteals, and RenalsDokument12 SeitenEvolving Approaches To The Iliacs, Femorals, Popliteals, and RenalsSohil ElfarNoch keine Bewertungen
- Platelet Glycoprotein Iib/Iiia Inhibition With Coronary Stenting For Acute Myocardial InfarctionDokument9 SeitenPlatelet Glycoprotein Iib/Iiia Inhibition With Coronary Stenting For Acute Myocardial InfarctionJanuar RezkyNoch keine Bewertungen
- Left Atrial Appendage Occlusion During Cadiac Surgery To Prevent StrokeDokument11 SeitenLeft Atrial Appendage Occlusion During Cadiac Surgery To Prevent Strokengoc tin nguyenNoch keine Bewertungen
- New England Journal Medicine: The ofDokument10 SeitenNew England Journal Medicine: The ofNatalia ArizaNoch keine Bewertungen
- ATTENTION TrialDokument12 SeitenATTENTION TrialmrabhilekhNoch keine Bewertungen
- 62 2020 Article 898Dokument7 Seiten62 2020 Article 898sinamirjaniNoch keine Bewertungen
- Recent Advances and Future Trends in Cardiology: Upendra Kaul, Parneesh AroraDokument4 SeitenRecent Advances and Future Trends in Cardiology: Upendra Kaul, Parneesh Arorashamir naazNoch keine Bewertungen
- Results of Heparin-Bonded ePTFE-covered Stents For Chronic Occlusive Superficial Femoral Artery DiseaseDokument8 SeitenResults of Heparin-Bonded ePTFE-covered Stents For Chronic Occlusive Superficial Femoral Artery DiseaseNurul Azmi Rosmala PutriNoch keine Bewertungen
- Trial of Endovascular Thrombectomy For Large Ischemic StrokesDokument13 SeitenTrial of Endovascular Thrombectomy For Large Ischemic StrokesMABEL LUCERO OLARTE JURADONoch keine Bewertungen
- 82 cases-Tub-multicenter-2018-ChanghaiDokument10 Seiten82 cases-Tub-multicenter-2018-Changhaiying huangNoch keine Bewertungen
- Emboli ParuDokument10 SeitenEmboli Paruindry_purnamasariNoch keine Bewertungen
- Kring JournalDokument3 SeitenKring JournalcbanguisNoch keine Bewertungen
- Resuscitation of Endotheliopathy and Bleeding in Thoracic Aortic Dissections: The VIPER-OCTA Randomized Clinical Pilot TrialDokument8 SeitenResuscitation of Endotheliopathy and Bleeding in Thoracic Aortic Dissections: The VIPER-OCTA Randomized Clinical Pilot TrialDanang Bagus UntoroNoch keine Bewertungen
- Goyal Et Al-2015-Annals of NeurologyDokument7 SeitenGoyal Et Al-2015-Annals of NeurologyWinda Wahyu IkaputriNoch keine Bewertungen
- New England Journal Medicine: The ofDokument10 SeitenNew England Journal Medicine: The ofPablo BarraganNoch keine Bewertungen
- Articol ExempluDokument12 SeitenArticol ExempluVlad NeagoeNoch keine Bewertungen
- Fassbender 2020Dokument10 SeitenFassbender 2020widyadariNoch keine Bewertungen
- EFNS Congress Vienna Semax AbstractDokument60 SeitenEFNS Congress Vienna Semax AbstractnontjeNoch keine Bewertungen
- Stenting Versus Aggressive Medical Therapy For Intracranial Arterial StenosisDokument11 SeitenStenting Versus Aggressive Medical Therapy For Intracranial Arterial StenosisariNoch keine Bewertungen
- Endovascular Stentgraft Placement in Aortic Dissection A MetaanalysisDokument10 SeitenEndovascular Stentgraft Placement in Aortic Dissection A MetaanalysisCiubuc AndrianNoch keine Bewertungen
- Management of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDokument6 SeitenManagement of Epistaxis in Patients With Ventricular Assist Device: A Retrospective ReviewDenta HaritsaNoch keine Bewertungen
- Dorner Av ShuntDokument13 SeitenDorner Av ShuntClaudia TiffanyNoch keine Bewertungen
- Nejmoa 1805374Dokument10 SeitenNejmoa 1805374Lia Diana RaileanuNoch keine Bewertungen
- S126 FullDokument12 SeitenS126 FullIago CarvalhoNoch keine Bewertungen
- Hemodialysis Internal Jugular Vein Versus Subclavian Vein Catheters: Complications, Patients' Comfort, Tolerance and Cost-EffectivenessDokument5 SeitenHemodialysis Internal Jugular Vein Versus Subclavian Vein Catheters: Complications, Patients' Comfort, Tolerance and Cost-EffectivenessYolanda IrawatiNoch keine Bewertungen
- Onwudike 2020Dokument10 SeitenOnwudike 2020Han's OfficialNoch keine Bewertungen
- ESC Hot Line: European Heart Journal (2015) 36, 3359-3367 Doi:10.1093/eurheartj/ehv444Dokument9 SeitenESC Hot Line: European Heart Journal (2015) 36, 3359-3367 Doi:10.1093/eurheartj/ehv444maranzazuuNoch keine Bewertungen
- s41598 019 45312 XDokument8 Seitens41598 019 45312 XrakaNoch keine Bewertungen
- Resumption of Antithrombotic Agents in C PDFDokument28 SeitenResumption of Antithrombotic Agents in C PDFNurul FajriNoch keine Bewertungen
- Icvts Ivv355 FullDokument7 SeitenIcvts Ivv355 FullAldo AtjehNoch keine Bewertungen
- Piis1051044322007734 1Dokument18 SeitenPiis1051044322007734 1Nachchakorn DellNoch keine Bewertungen
- Chronic SDHDokument8 SeitenChronic SDHAnonymous A9R0aLsNoch keine Bewertungen
- Comparative Efficacy of 2 Zotarolimus-Eluting Stent Generations: Resolute Versus Endeavor Stents in Patients With Coronary Artery DiseaseDokument7 SeitenComparative Efficacy of 2 Zotarolimus-Eluting Stent Generations: Resolute Versus Endeavor Stents in Patients With Coronary Artery Diseaseanindia wardhaniNoch keine Bewertungen
- New England Journal Medicine: The ofDokument13 SeitenNew England Journal Medicine: The ofAlexei Ricse JiménezNoch keine Bewertungen
- Aspirina Después de Fractura Art Ing 2023Dokument4 SeitenAspirina Después de Fractura Art Ing 2023roman rodriguezNoch keine Bewertungen
- Best Practices of Apheresis in Hematopoietic Cell TransplantationVon EverandBest Practices of Apheresis in Hematopoietic Cell TransplantationSyed A. AbutalibNoch keine Bewertungen
- Ni Hms 358630Dokument27 SeitenNi Hms 358630Kartikeya SinghNoch keine Bewertungen
- Tokyo Ghoul Zakki Helvetica ScansDokument86 SeitenTokyo Ghoul Zakki Helvetica ScansReza Ishak Estiko50% (4)
- Liang 2017Dokument6 SeitenLiang 2017Reza Ishak EstikoNoch keine Bewertungen
- CONSORT 2010 ChecklistDokument2 SeitenCONSORT 2010 ChecklistReza Ishak EstikoNoch keine Bewertungen
- Chinas Strategy in The Middle East The Silk RoadDokument16 SeitenChinas Strategy in The Middle East The Silk RoadReza Ishak EstikoNoch keine Bewertungen
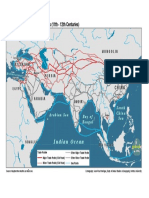
- The Silk Road and Arab Sea Routes (11th - 12th Centuries) : Indian OceanDokument1 SeiteThe Silk Road and Arab Sea Routes (11th - 12th Centuries) : Indian OceanReza Ishak EstikoNoch keine Bewertungen
- art3A10.10072Fs10943 013 9780 41 PDFDokument13 Seitenart3A10.10072Fs10943 013 9780 41 PDFReza Ishak EstikoNoch keine Bewertungen
- Odor Taste Integration and The Perception of Flavor 1Dokument14 SeitenOdor Taste Integration and The Perception of Flavor 1Reza Ishak EstikoNoch keine Bewertungen
- Basic Upper Preparation StepsDokument7 SeitenBasic Upper Preparation StepsumidgrtNoch keine Bewertungen
- Air Preparation Products: Parker Pneumatic Section EDokument11 SeitenAir Preparation Products: Parker Pneumatic Section EPartsGopher.comNoch keine Bewertungen
- CS410 Series and CS417: User's GuideDokument209 SeitenCS410 Series and CS417: User's Guident11Noch keine Bewertungen
- Measurement of Carbon Dioxide Content: Centec Process SensorsDokument2 SeitenMeasurement of Carbon Dioxide Content: Centec Process Sensorslaoying qdNoch keine Bewertungen
- International TradeDokument28 SeitenInternational TradeAmit Sharma0% (1)
- Avl Tree Definition: Avl Trees Are Balanced Anavltreeisa Such That For Every Internal Node V of T, TheDokument3 SeitenAvl Tree Definition: Avl Trees Are Balanced Anavltreeisa Such That For Every Internal Node V of T, TheSumanta DattaNoch keine Bewertungen
- DIFFERENTIALDokument4 SeitenDIFFERENTIALsaffrinNoch keine Bewertungen
- Bharat Heavy Electricals LimitedDokument19 SeitenBharat Heavy Electricals LimitedChandreshDharDubeyNoch keine Bewertungen
- Abinash Master SeminarDokument51 SeitenAbinash Master SeminarAGRICULTURE BOYNoch keine Bewertungen
- Mil STD 785BDokument90 SeitenMil STD 785BLaura Encinas EscobarNoch keine Bewertungen
- Alvit Catalog - EN - Only Ceramics.Dokument41 SeitenAlvit Catalog - EN - Only Ceramics.yves boussouNoch keine Bewertungen
- 06072G Chapter Sample PDFDokument11 Seiten06072G Chapter Sample PDFAnonymous 1hOgJqwZuzNoch keine Bewertungen
- Virgin Mobile Insurance BookletDokument51 SeitenVirgin Mobile Insurance BookletdanatheteacherNoch keine Bewertungen
- Computation of Area of A Closed TraversedDokument3 SeitenComputation of Area of A Closed TraversedDaryl Ballesteros100% (1)
- The Supply Chain For Electric Vehicle BatteriesDokument21 SeitenThe Supply Chain For Electric Vehicle BatteriesProbonogoya Erawan Sastroredjo100% (2)
- OBGYN Form 3 Answers KeyDokument2 SeitenOBGYN Form 3 Answers KeyGrace0% (1)
- 10TH Gseb PaperDokument10 Seiten10TH Gseb Paperkhushboo guptaNoch keine Bewertungen
- Cash Valve Product OverviewDokument16 SeitenCash Valve Product OverviewestebanNoch keine Bewertungen
- MetabolismDokument21 SeitenMetabolismNagendra NayakNoch keine Bewertungen
- RCCHEMDokument10 SeitenRCCHEMKartik PandeyNoch keine Bewertungen
- MM 361: Advanced Manufacturing: InstructionsDokument3 SeitenMM 361: Advanced Manufacturing: InstructionsSimLo Lulumani Ko'osiko Taloanimae'aNoch keine Bewertungen
- Report of Mechanics of Machines 1Dokument12 SeitenReport of Mechanics of Machines 1muhammaduzairNoch keine Bewertungen
- LC Passive Wireless Sensors Toward A Wireless Sensing Platform: Status, Prospects, and ChallengesDokument20 SeitenLC Passive Wireless Sensors Toward A Wireless Sensing Platform: Status, Prospects, and ChallengesCristian David Merchan VegaNoch keine Bewertungen
- Theories and philosophies that shaped early childhood educationDokument3 SeitenTheories and philosophies that shaped early childhood educationJamille Aira PascuaNoch keine Bewertungen
- Moral vs Non-Moral Standards ExplainedDokument2 SeitenMoral vs Non-Moral Standards ExplainedLee PascuaNoch keine Bewertungen
- Brother Printer GT-782Dokument126 SeitenBrother Printer GT-782vitprint22Noch keine Bewertungen
- Tuto Traktor Arduino enDokument11 SeitenTuto Traktor Arduino enlexetaNoch keine Bewertungen
- Neem CofA 141019-4Dokument1 SeiteNeem CofA 141019-4Rahayuteuk Elf100% (1)
- SAP Sales Order Store Returns (Intercompany)Dokument2 SeitenSAP Sales Order Store Returns (Intercompany)Donny CorleonNoch keine Bewertungen
- How To Use PathlossDokument32 SeitenHow To Use Pathlosspathlossanwar100% (9)