Das könnte Ihnen auch gefallen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Role of Room RatesDokument5 SeitenRole of Room RatesJonathan JacquezNoch keine Bewertungen
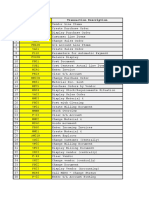
- # Transaction Code Transaction DescriptionDokument6 Seiten# Transaction Code Transaction DescriptionVivek Shashikant SonawaneNoch keine Bewertungen
- JhdsjkduijhsbsgdDokument3 SeitenJhdsjkduijhsbsgdRanvidsNoch keine Bewertungen
- Acc Topic 8Dokument2 SeitenAcc Topic 8BM10622P Nur Alyaa Nadhirah Bt Mohd RosliNoch keine Bewertungen
- Delhi To AhmedabadDokument2 SeitenDelhi To Ahmedabad02 Raihan Ahmedi 2997Noch keine Bewertungen
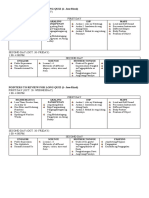
- TOURISM AND HOSPITALITY ORGANIZATIONS Di Pa Tapooos 1 1Dokument101 SeitenTOURISM AND HOSPITALITY ORGANIZATIONS Di Pa Tapooos 1 1Dianne EvangelistaNoch keine Bewertungen
- Vampire - Habent Sua Fata Libelli - by Hanns Heinz EwersDokument2 SeitenVampire - Habent Sua Fata Libelli - by Hanns Heinz EwersJoe E BandelNoch keine Bewertungen
- Humanrigtsni: Human Rights: Developmen in IndiaDokument71 SeitenHumanrigtsni: Human Rights: Developmen in IndiaAastha AgarwalNoch keine Bewertungen
- Pointers To Review For Long QuizDokument1 SeitePointers To Review For Long QuizJoice Ann PolinarNoch keine Bewertungen
- Caste Endogamy A Multidimensional Analogy of Caste in The Indian SocietyDokument12 SeitenCaste Endogamy A Multidimensional Analogy of Caste in The Indian SocietyRakshith L1Noch keine Bewertungen
- A Master Budget Case (Project-2)Dokument16 SeitenA Master Budget Case (Project-2)Shaikh Junaid50% (2)
- Session 1 Introduction To Operations Management 3.0Dokument48 SeitenSession 1 Introduction To Operations Management 3.0Aryan DwivediNoch keine Bewertungen
- Blockchain PaperDokument33 SeitenBlockchain PaperAyeshas KhanNoch keine Bewertungen
- Devel Goth ArchDokument512 SeitenDevel Goth ArchAmiee Groundwater100% (2)
- Capacity Planning FinalizeDokument85 SeitenCapacity Planning FinalizeHansel Ramirez BaruelaNoch keine Bewertungen
- Home / Publications / Questions and AnswersDokument81 SeitenHome / Publications / Questions and AnswersMahmoudNoch keine Bewertungen
- EPLC Annual Operational Analysis TemplateDokument8 SeitenEPLC Annual Operational Analysis TemplateHussain ElarabiNoch keine Bewertungen
- Koalatext 4Dokument8 SeitenKoalatext 4YolandaOrduñaNoch keine Bewertungen
- Congressional Record - House H104: January 6, 2011Dokument1 SeiteCongressional Record - House H104: January 6, 2011olboy92Noch keine Bewertungen
- Historical Perspective of Financial Reporting Regulations in MalaysiaDokument2 SeitenHistorical Perspective of Financial Reporting Regulations in Malaysiauglore100% (6)
- Internal Assignment Applicable For June 2017 Examination: Course: Cost and Management AccountingDokument2 SeitenInternal Assignment Applicable For June 2017 Examination: Course: Cost and Management Accountingnbala.iyerNoch keine Bewertungen
- Garment Manufacturing TechnologyDokument3 SeitenGarment Manufacturing TechnologyamethiaexportNoch keine Bewertungen
- Unit Test 7A: 1 Choose The Correct Form of The VerbDokument4 SeitenUnit Test 7A: 1 Choose The Correct Form of The VerbAmy PuenteNoch keine Bewertungen
- Chapter 2-Futurecast Applied To TourismDokument5 SeitenChapter 2-Futurecast Applied To TourismAsya KnNoch keine Bewertungen
- Marketing Case - Cowgirl ChocolatesDokument14 SeitenMarketing Case - Cowgirl Chocolatessarah_alexandra2100% (4)
- BVP651 Installation ManualDokument12 SeitenBVP651 Installation ManualAnonymous qDCftTW5MNoch keine Bewertungen
- UPS Full ProofDokument1 SeiteUPS Full Proofyotel52289Noch keine Bewertungen
- Indira Gandhi BiographyDokument4 SeitenIndira Gandhi BiographySocial SinghNoch keine Bewertungen
- The Economic Burden of ObesityDokument13 SeitenThe Economic Burden of ObesityNasir Ali100% (1)
- Seminar On HackingDokument21 SeitenSeminar On Hackingpandu16550% (2)