Das könnte Ihnen auch gefallen
- Natural & Safe: The Handbook: Family Planning with SensiplanVon EverandNatural & Safe: The Handbook: Family Planning with SensiplanBewertung: 5 von 5 Sternen5/5 (3)
- HO 4 Essential Intrapartum Care 6may2013Dokument12 SeitenHO 4 Essential Intrapartum Care 6may2013Maedine Urbano-Briones100% (1)
- Peace Corps MTG 700 General Medicine 2Dokument191 SeitenPeace Corps MTG 700 General Medicine 2Accessible Journal Media: Peace Corps DocumentsNoch keine Bewertungen
- CHN FinalsDokument15 SeitenCHN FinalsLuna sibilityNoch keine Bewertungen
- Explain 4Dokument21 SeitenExplain 4CHACHACHACHAAAAANoch keine Bewertungen
- Prenatal Practice Guidelines: Primary Source: AAP/ACOG Guidelines For Perinatal Care, 5 Edition, 2002Dokument5 SeitenPrenatal Practice Guidelines: Primary Source: AAP/ACOG Guidelines For Perinatal Care, 5 Edition, 2002filberts.girl9025Noch keine Bewertungen
- Objectives: Common Medications in Obstetrics & GynecologyDokument9 SeitenObjectives: Common Medications in Obstetrics & Gynecologygazi haseebNoch keine Bewertungen
- Detailed Activities of Service ProviderDokument7 SeitenDetailed Activities of Service ProviderJahin KhanNoch keine Bewertungen
- Practical General Practice Ebook Guidelines For E... - (PG 242 - 244)Dokument3 SeitenPractical General Practice Ebook Guidelines For E... - (PG 242 - 244)Sarah UddinNoch keine Bewertungen
- Module 4 - Contraception and Family PlanningDokument18 SeitenModule 4 - Contraception and Family PlanningKath NambuNoch keine Bewertungen
- Comprehensive PAC - ProfAlisonDokument56 SeitenComprehensive PAC - ProfAlisonMajigs IdNoch keine Bewertungen
- Antenatal Care IsDokument19 SeitenAntenatal Care IsShivani Shah100% (1)
- Venous Thromboembolism (VTE) Prophylaxis inDokument24 SeitenVenous Thromboembolism (VTE) Prophylaxis inVesna EfremNoch keine Bewertungen
- Empo Tech Group 1Dokument14 SeitenEmpo Tech Group 1Michael AysonNoch keine Bewertungen
- Reproductive Health PowerNotes by KT SirDokument2 SeitenReproductive Health PowerNotes by KT Sirjumihuss08Noch keine Bewertungen
- Reproductive HealthDokument6 SeitenReproductive HealthAdesh BhullarNoch keine Bewertungen
- Multiple Pregnancy GuidelineDokument12 SeitenMultiple Pregnancy GuidelineAlia BangeshNoch keine Bewertungen
- Kami Export - I Am Sharing 'PCEP - Book 4 - Specialized Newborn Care - 4th Edition' With YouDokument260 SeitenKami Export - I Am Sharing 'PCEP - Book 4 - Specialized Newborn Care - 4th Edition' With YouZeljka Dobric KelecevicNoch keine Bewertungen
- MCNCHP 1 NotesDokument3 SeitenMCNCHP 1 Noteshannahabigael.cajesNoch keine Bewertungen
- WOMENâ S HEALTHnewDokument52 SeitenWOMENâ S HEALTHnewHossen AliNoch keine Bewertungen
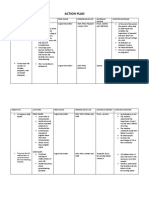
- Maternal and child health action planDokument4 SeitenMaternal and child health action planJosette Mae Atanacio67% (3)
- Action PlanDokument4 SeitenAction PlanJosette Mae Atanacio100% (4)
- Guide: Opioids in LabourDokument2 SeitenGuide: Opioids in LabourSarah AlharbiNoch keine Bewertungen
- Pedia Midterm ReviewerDokument17 SeitenPedia Midterm ReviewerRheyshelle Angela AnchetaNoch keine Bewertungen
- Maternal Aspects of ENC - FEU2014Dokument79 SeitenMaternal Aspects of ENC - FEU2014Rinah GonzagaNoch keine Bewertungen
- Placenta Previa HandoutDokument2 SeitenPlacenta Previa HandoutjuanNoch keine Bewertungen
- Contraceptives FINAL NFHS-4 TOTDokument62 SeitenContraceptives FINAL NFHS-4 TOTRajat JainNoch keine Bewertungen
- Best Practices in Maternity CareDokument32 SeitenBest Practices in Maternity CareFev BanataoNoch keine Bewertungen
- Ilovepdf MergedDokument125 SeitenIlovepdf MergedinnyNoch keine Bewertungen
- Reproductive Health-Problems & StrategiesDokument11 SeitenReproductive Health-Problems & StrategiesUtkarsh SinghNoch keine Bewertungen
- Preventive Pediatrics Part 3Dokument5 SeitenPreventive Pediatrics Part 3mkct111Noch keine Bewertungen
- 12.family Planning PDFDokument36 Seiten12.family Planning PDFSadia YousafNoch keine Bewertungen
- Family Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Dokument73 SeitenFamily Planning: By: Khalid Jemal (MD, Assistant Prof. of Obstetrics & Gynecology)Degefaw BikoyNoch keine Bewertungen
- Drug Use During Pregnancy and LactationDokument31 SeitenDrug Use During Pregnancy and LactationAddisieNoch keine Bewertungen
- REPRODUCTIVE HEALTH CHAPTER CLASS XIIDokument16 SeitenREPRODUCTIVE HEALTH CHAPTER CLASS XIIShazia Khatoon100% (1)
- Clinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineDokument10 SeitenClinical Guideline: Prelabour Rupture of The Membranes (PROM) 37 Weeks Clinical GuidelineUtomo BudidarmoNoch keine Bewertungen
- Contraception Final Presentation 1 2Dokument24 SeitenContraception Final Presentation 1 2api-506215635Noch keine Bewertungen
- Emonc ProtocolDokument38 SeitenEmonc ProtocolXerxes MalagaNoch keine Bewertungen
- Womens HealthDokument23 SeitenWomens Healthtaty jatyNoch keine Bewertungen
- Adult Contraception Cue CardsDokument28 SeitenAdult Contraception Cue CardsJohanna ValentinaNoch keine Bewertungen
- Reproductive HealthDokument80 SeitenReproductive HealthSreejithKumarNoch keine Bewertungen
- Emergency Contraception and LARC Access in the ERDokument31 SeitenEmergency Contraception and LARC Access in the ERVeronica M. Alvarez-GalianaNoch keine Bewertungen
- Framework For Maternal and Child Health NursingDokument1 SeiteFramework For Maternal and Child Health NursingSeth Josiah E. MacalaladNoch keine Bewertungen
- Epilepsy in Pregnancy 5.1Dokument10 SeitenEpilepsy in Pregnancy 5.1Guntur AntonNoch keine Bewertungen
- Antenatal Care Guidelines: Doctors of The WorldDokument16 SeitenAntenatal Care Guidelines: Doctors of The WorldNadiah FtrNoch keine Bewertungen
- OB 0101D Preconceptional Counseling and Prenatal CareDokument10 SeitenOB 0101D Preconceptional Counseling and Prenatal CarevincejavierNoch keine Bewertungen
- Breastfeeding without birthing guideDokument6 SeitenBreastfeeding without birthing guideMark Terence Padua AbrenicaNoch keine Bewertungen
- QI Basic Training Participant Hand Out 2021Dokument257 SeitenQI Basic Training Participant Hand Out 2021drkefyalewtayeNoch keine Bewertungen
- Chapter 6 Lecture Health, The BasicsDokument58 SeitenChapter 6 Lecture Health, The BasicsWenzy CruzNoch keine Bewertungen
- Perineal Care: South Australian Perinatal Practice GuidelineDokument11 SeitenPerineal Care: South Australian Perinatal Practice GuidelineAshley Jay Bulda BarbosaNoch keine Bewertungen
- 3.3 Family PlanningDokument9 Seiten3.3 Family PlanningGayle Regine DaquialNoch keine Bewertungen
- Essential Intrapartum Care: From Evidence To PracticeDokument78 SeitenEssential Intrapartum Care: From Evidence To PracticeGeline Joy D. SamillanoNoch keine Bewertungen
- Placenta Previa Incidence and OutcomesDokument5 SeitenPlacenta Previa Incidence and OutcomeshumairohimaniaNoch keine Bewertungen
- Nursing Care of Mother With Complications During PregnancyDokument32 SeitenNursing Care of Mother With Complications During Pregnancydad112389Noch keine Bewertungen
- MCH Newborn and Family Planning PriyaDokument54 SeitenMCH Newborn and Family Planning PriyaPrethy PhilipNoch keine Bewertungen
- After Miscarriage 250320Dokument3 SeitenAfter Miscarriage 250320Putu Gede WidyatamaNoch keine Bewertungen
- Nipple Pain Incidence, The Predisposing Factors, The Recovery Period After Care Management, and The Exclusive Breastfeeding OutcomeDokument5 SeitenNipple Pain Incidence, The Predisposing Factors, The Recovery Period After Care Management, and The Exclusive Breastfeeding OutcomeCarmine XanderNoch keine Bewertungen
- Contraception: Amanda White Madelaine YatesDokument29 SeitenContraception: Amanda White Madelaine YatesAmandaWonnacottNoch keine Bewertungen
- ANC2Dokument33 SeitenANC2JoebestNoch keine Bewertungen
- Panna Dhai Maa Subharti Nursing College, Meerut: Seminar On AbortionDokument31 SeitenPanna Dhai Maa Subharti Nursing College, Meerut: Seminar On Abortionriya singhNoch keine Bewertungen
- TextDokument1 SeiteTextLot RositNoch keine Bewertungen
- Cover LetterDokument2 SeitenCover LetterLot RositNoch keine Bewertungen
- SLRC Handouts CHN OutlineDokument11 SeitenSLRC Handouts CHN OutlineLot RositNoch keine Bewertungen
- Cover LetterDokument2 SeitenCover LetterLot RositNoch keine Bewertungen
- A Typology of Nursing Problems in Family Nursing Practice - RNpediaDokument8 SeitenA Typology of Nursing Problems in Family Nursing Practice - RNpediaLot RositNoch keine Bewertungen
- Nursing Test Questions Nursing ResearchDokument2 SeitenNursing Test Questions Nursing ResearchLot RositNoch keine Bewertungen
- TextDokument1 SeiteTextLot RositNoch keine Bewertungen
- NCLEX Practice Exam For Pediatric Nursing 2 - RNpediaDokument14 SeitenNCLEX Practice Exam For Pediatric Nursing 2 - RNpediaLot RositNoch keine Bewertungen
- TextDokument2 SeitenTextLot RositNoch keine Bewertungen
- PNLE: Community Health Nursing Exam 5 - RNpediaDokument13 SeitenPNLE: Community Health Nursing Exam 5 - RNpediaLot RositNoch keine Bewertungen
- Nclex 4Dokument5 SeitenNclex 4Lot RositNoch keine Bewertungen
- Nursing Test Questions Nursing ResearchDokument4 SeitenNursing Test Questions Nursing ResearchLot RositNoch keine Bewertungen
- TextDokument23 SeitenTextLot RositNoch keine Bewertungen
- Maternal & Child Practice Exam 9 (Intrapartum)Dokument29 SeitenMaternal & Child Practice Exam 9 (Intrapartum)Lot Rosit100% (1)
- Lab ValuesDokument1 SeiteLab ValuesKathy Real VillsNoch keine Bewertungen
- NCLEX Practice Exam For Pediatric Nursing 1: Start StartDokument9 SeitenNCLEX Practice Exam For Pediatric Nursing 1: Start StartLot RositNoch keine Bewertungen
- PNLE: Community Health Nursing Exam 1 - RNpediaDokument13 SeitenPNLE: Community Health Nursing Exam 1 - RNpediaLot Rosit100% (2)
- PNLE III For Medical Surgical Nursing - RNpediaDokument13 SeitenPNLE III For Medical Surgical Nursing - RNpediaLot RositNoch keine Bewertungen
- Read MeDokument1 SeiteRead MeLot RositNoch keine Bewertungen
- Nclex 4Dokument5 SeitenNclex 4Lot RositNoch keine Bewertungen
- PNLE III For Medical Surgical Nursing - RNpediaDokument13 SeitenPNLE III For Medical Surgical Nursing - RNpediaLot RositNoch keine Bewertungen
- PNLE: Medical Surgical Nursing Exam 3Dokument9 SeitenPNLE: Medical Surgical Nursing Exam 3Lot RositNoch keine Bewertungen
- Nursing Test Questions Nursing ResearchDokument4 SeitenNursing Test Questions Nursing ResearchLot RositNoch keine Bewertungen
- PNLE: Maternal and Child Health Nursing Exam 3Dokument41 SeitenPNLE: Maternal and Child Health Nursing Exam 3Lot Rosit50% (2)
- Nursing Bullets: Pediatric Nursing IDokument3 SeitenNursing Bullets: Pediatric Nursing ILot RositNoch keine Bewertungen
- PNLE IV Nursing PracticeDokument15 SeitenPNLE IV Nursing PracticeLot RositNoch keine Bewertungen
- Maternal & Child Practice Exam 9 (Intrapartum)Dokument29 SeitenMaternal & Child Practice Exam 9 (Intrapartum)Lot Rosit100% (1)
- PNLE: Medical Surgical Nursing Exam 3Dokument9 SeitenPNLE: Medical Surgical Nursing Exam 3Lot RositNoch keine Bewertungen
- PNLE II Nursing PracticeDokument25 SeitenPNLE II Nursing PracticeLot RositNoch keine Bewertungen
- NCLEX Practice Exam For Maternal and Child Health Nursing 1Dokument15 SeitenNCLEX Practice Exam For Maternal and Child Health Nursing 1Lot RositNoch keine Bewertungen
- SDLC - Agile ModelDokument3 SeitenSDLC - Agile ModelMuhammad AkramNoch keine Bewertungen
- Intrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Dokument12 SeitenIntrinsic Resistance and Unusual Phenotypes Tables v3.2 20200225Roy MontoyaNoch keine Bewertungen
- Historyofluthera01morg PDFDokument420 SeitenHistoryofluthera01morg PDFJhonNoch keine Bewertungen
- We Don't Eat Our: ClassmatesDokument35 SeitenWe Don't Eat Our: ClassmatesChelle Denise Gumban Huyaban85% (20)
- Handout of English For PsychologyDokument75 SeitenHandout of English For PsychologyRivan Dwi AriantoNoch keine Bewertungen
- Life Convict Laxman Naskar Vs State of West Bengal & Anr On 1 September, 2000Dokument6 SeitenLife Convict Laxman Naskar Vs State of West Bengal & Anr On 1 September, 2000Kimberly HardyNoch keine Bewertungen
- Semi-Detailed Lesson Plan Template: Pagsanjan Intergrated National High School 8Dokument3 SeitenSemi-Detailed Lesson Plan Template: Pagsanjan Intergrated National High School 8Mae Ganate RoblesNoch keine Bewertungen
- Leading a Community Through Integrity and CourageDokument2 SeitenLeading a Community Through Integrity and CourageGretchen VenturaNoch keine Bewertungen
- Speed of Sound and its Relationship with TemperatureDokument2 SeitenSpeed of Sound and its Relationship with TemperatureBENNY CALLONoch keine Bewertungen
- Thin Layer Chromatograph1Dokument25 SeitenThin Layer Chromatograph12581974Noch keine Bewertungen
- GSM ZTE Paging Feature GuideDokument17 SeitenGSM ZTE Paging Feature Guidemikepadilla82100% (1)
- 2 NDDokument52 Seiten2 NDgal02lautNoch keine Bewertungen
- Book Review Reclaim Your HeartDokument7 SeitenBook Review Reclaim Your HeartShaheer KhanNoch keine Bewertungen
- Formula Sheet For Astronomy 1 - Paper 1 and Stars & PlanetsDokument2 SeitenFormula Sheet For Astronomy 1 - Paper 1 and Stars & PlanetsprashinNoch keine Bewertungen
- Prophetic Prayer Declarations - September, 2021Dokument5 SeitenProphetic Prayer Declarations - September, 2021Jelo RichNoch keine Bewertungen
- 6 Strategies For Effective Financial Management Trends in K12 SchoolsDokument16 Seiten6 Strategies For Effective Financial Management Trends in K12 SchoolsRainiel Victor M. CrisologoNoch keine Bewertungen
- Unit Test, Part 2: Literature With A Purpose: Total Score: - of 40 PointsDokument3 SeitenUnit Test, Part 2: Literature With A Purpose: Total Score: - of 40 PointsAriana Stephanya Anguiano VelazquezNoch keine Bewertungen
- 600 2 Sub-Zero Built-In Series Refrigerator Service ManualDokument188 Seiten600 2 Sub-Zero Built-In Series Refrigerator Service Manual911servicetechNoch keine Bewertungen
- Silvianita - LK 0.1 Modul 2 English For Personal CommunicationDokument3 SeitenSilvianita - LK 0.1 Modul 2 English For Personal CommunicationSilvianita RetnaningtyasNoch keine Bewertungen
- Discuss in Details With Appropriate Examples What Factors Could Lead To Sympatric and Allopatric SpeciationDokument5 SeitenDiscuss in Details With Appropriate Examples What Factors Could Lead To Sympatric and Allopatric SpeciationKhairul ShahmiNoch keine Bewertungen
- Code of Conduct GuidanceDokument17 SeitenCode of Conduct GuidanceMuhammad RidwanNoch keine Bewertungen
- Origin and Development of Law of Sea PDFDokument135 SeitenOrigin and Development of Law of Sea PDFkimmiahujaNoch keine Bewertungen
- School For Good and EvilDokument4 SeitenSchool For Good and EvilHaizyn RizoNoch keine Bewertungen
- Hospital Registration Orientation 3 - EQRs With Operating ManualDokument33 SeitenHospital Registration Orientation 3 - EQRs With Operating ManualElshaimaa AbdelfatahNoch keine Bewertungen
- Foundation of Special and Inclusive EducationDokument25 SeitenFoundation of Special and Inclusive Educationmarjory empredoNoch keine Bewertungen
- PIC16 F 1619Dokument594 SeitenPIC16 F 1619Francisco Martinez AlemanNoch keine Bewertungen
- People v Gemoya and Tionko - Supreme Court upholds murder convictionDokument7 SeitenPeople v Gemoya and Tionko - Supreme Court upholds murder convictionLASNoch keine Bewertungen
- Philhis Handouts Week 1Dokument5 SeitenPhilhis Handouts Week 1Jeen JeenNoch keine Bewertungen
- The Perfect Prayer by by Jon Courson - Matthew 6 9-13 The Lords PrayerDokument6 SeitenThe Perfect Prayer by by Jon Courson - Matthew 6 9-13 The Lords PrayerRobert Beaupre100% (1)
- DRR Module 4 Detailed Lesson PlanDokument8 SeitenDRR Module 4 Detailed Lesson PlanFe Annalie Sacal100% (2)
- Perimenopause Power: Navigating your hormones on the journey to menopauseVon EverandPerimenopause Power: Navigating your hormones on the journey to menopauseBewertung: 4 von 5 Sternen4/5 (2)
- The Menopause Manifesto: Own Your Health With Facts and FeminismVon EverandThe Menopause Manifesto: Own Your Health With Facts and FeminismBewertung: 4 von 5 Sternen4/5 (18)
- The Pain Gap: How Sexism and Racism in Healthcare Kill WomenVon EverandThe Pain Gap: How Sexism and Racism in Healthcare Kill WomenBewertung: 4 von 5 Sternen4/5 (153)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisVon EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisBewertung: 3 von 5 Sternen3/5 (2)
- What No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodVon EverandWhat No One Tells You: A Guide to Your Emotions from Pregnancy to MotherhoodBewertung: 4.5 von 5 Sternen4.5/5 (30)
- Younger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondVon EverandYounger Next Year, 2nd Edition: Live Strong, Fit, Sexy, and Smart-Until You're 80 and BeyondBewertung: 4 von 5 Sternen4/5 (110)
- Sacred Womb Healing Meditation Divine feminine alignment: heal ancestral traumas deep wounds, release blocked sexual energies, flow to creativity, overcome the energies of birthing, joy love happyVon EverandSacred Womb Healing Meditation Divine feminine alignment: heal ancestral traumas deep wounds, release blocked sexual energies, flow to creativity, overcome the energies of birthing, joy love happyBewertung: 5 von 5 Sternen5/5 (1)
- What to Expect When You’re Expecting (5th Edition)Von EverandWhat to Expect When You’re Expecting (5th Edition)Bewertung: 5 von 5 Sternen5/5 (1)
- A Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersVon EverandA Radical Guide for Women with ADHD: Embrace Neurodiversity, Live Boldly, and Break Through BarriersBewertung: 4.5 von 5 Sternen4.5/5 (71)
- I'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionVon EverandI'll Start Again Monday: Break the Cycle of Unhealthy Eating Habits with Lasting Spiritual SatisfactionBewertung: 4.5 von 5 Sternen4.5/5 (124)
- Brain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfVon EverandBrain Body Diet: 40 Days to a Lean, Calm, Energized, and Happy SelfBewertung: 5 von 5 Sternen5/5 (2)
- The Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouVon EverandThe Autoimmune Cure: Healing the Trauma and Other Triggers That Have Turned Your Body Against YouNoch keine Bewertungen
- ADHD Women: A Holistic Approach To ADHD ManagementVon EverandADHD Women: A Holistic Approach To ADHD ManagementBewertung: 5 von 5 Sternen5/5 (4)
- All in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayVon EverandAll in Her Head: The Truth and Lies Early Medicine Taught Us About Women’s Bodies and Why It Matters TodayBewertung: 5 von 5 Sternen5/5 (2)
- Women, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainVon EverandWomen, Food, And Hormones: A 4-Week Plan to Achieve Hormonal Balance, Lose Weight, and Feel Like Yourself AgainBewertung: 4 von 5 Sternen4/5 (14)
- ROAR: How to Match Your Food and Fitness to Your Unique Female Physiology for Optimum Performance, Great Health, and a Strong, Lean Body for LifeVon EverandROAR: How to Match Your Food and Fitness to Your Unique Female Physiology for Optimum Performance, Great Health, and a Strong, Lean Body for LifeBewertung: 4.5 von 5 Sternen4.5/5 (44)
- I'm So Effing Hungry: Why We Crave What We Crave – and What to Do About ItVon EverandI'm So Effing Hungry: Why We Crave What We Crave – and What to Do About ItNoch keine Bewertungen
- You've Got to Be Kidding Me!: Perimenopause Symptoms, Stages & StrategiesVon EverandYou've Got to Be Kidding Me!: Perimenopause Symptoms, Stages & StrategiesNoch keine Bewertungen
- The First Forty Days: The Essential Art of Nourishing the New MotherVon EverandThe First Forty Days: The Essential Art of Nourishing the New MotherBewertung: 5 von 5 Sternen5/5 (5)
- The Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthVon EverandThe Mama Natural Week-by-Week Guide to Pregnancy and ChildbirthBewertung: 4.5 von 5 Sternen4.5/5 (21)
- The Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesVon EverandThe Better Period Food Solution: Eat Your Way to a Lifetime of Healthier CyclesNoch keine Bewertungen
- Menopause: All you need to know in one concise manualVon EverandMenopause: All you need to know in one concise manualBewertung: 5 von 5 Sternen5/5 (11)
- Dark Feminine Energy: Free Your Femme Fatale Ignite Your Irresistible Allure Through Mystique, Sexuality, Femininity, and Elegance to Become the Dark Diva No One Can IgnoreVon EverandDark Feminine Energy: Free Your Femme Fatale Ignite Your Irresistible Allure Through Mystique, Sexuality, Femininity, and Elegance to Become the Dark Diva No One Can IgnoreBewertung: 1 von 5 Sternen1/5 (1)
- The 21-Day Self-Love Challenge: Learn How to Love Yourself Unconditionally, Cultivate Confidence, Self-Compassion and Self-WorthVon EverandThe 21-Day Self-Love Challenge: Learn How to Love Yourself Unconditionally, Cultivate Confidence, Self-Compassion and Self-WorthNoch keine Bewertungen
- Rediscover Your Sparkle: Nourish Your SoulVon EverandRediscover Your Sparkle: Nourish Your SoulBewertung: 4.5 von 5 Sternen4.5/5 (4)
- I'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeVon EverandI'm So Effing Tired: A Proven Plan to Beat Burnout, Boost Your Energy, and Reclaim Your LifeBewertung: 4 von 5 Sternen4/5 (15)
- Breaking Free from Body Shame: Dare to Reclaim What God Has Named GoodVon EverandBreaking Free from Body Shame: Dare to Reclaim What God Has Named GoodBewertung: 5 von 5 Sternen5/5 (33)
- First Time Mom: A new Moms survival guide to prepare yourself for pregnancy,labor, childbirth, and New Born BabyVon EverandFirst Time Mom: A new Moms survival guide to prepare yourself for pregnancy,labor, childbirth, and New Born BabyBewertung: 4.5 von 5 Sternen4.5/5 (4)
- Call of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodVon EverandCall of the Wild: How We Heal Trauma, Awaken Our Own Power, and Use It For GoodNoch keine Bewertungen
- Menopausing: The positive roadmap to your second springVon EverandMenopausing: The positive roadmap to your second springBewertung: 5 von 5 Sternen5/5 (20)