Das könnte Ihnen auch gefallen
- Kaiser Permanente California Plans and Benefits Brochure KPIF 2011Dokument6 SeitenKaiser Permanente California Plans and Benefits Brochure KPIF 2011DennisNoch keine Bewertungen
- 2010 UHC Medical Plan ComparisonDokument2 Seiten2010 UHC Medical Plan Comparisonapi-20618861Noch keine Bewertungen
- Core MVDokument1 SeiteCore MVGowell SupportNoch keine Bewertungen
- First Help PlanDokument1 SeiteFirst Help PlanIvan QuevedoNoch keine Bewertungen
- 2022 Steven Charles BAG - CODokument4 Seiten2022 Steven Charles BAG - COAlejuanchis Kamacho GarciaNoch keine Bewertungen
- 2023 Talent BAAGDokument3 Seiten2023 Talent BAAGThi HanNoch keine Bewertungen
- Benefit Highlights: AARP Medicare Advantage Choice (PPO)Dokument3 SeitenBenefit Highlights: AARP Medicare Advantage Choice (PPO)EstherNoch keine Bewertungen
- Kaiser Permanente Compare Plans CA 2011 KPIFDokument1 SeiteKaiser Permanente Compare Plans CA 2011 KPIFDennis AlexanderNoch keine Bewertungen
- Choice MVDokument1 SeiteChoice MVGowell SupportNoch keine Bewertungen
- EmblemHealth Benefits 2019Dokument7 SeitenEmblemHealth Benefits 2019Jorge Luis Rivera AgostoNoch keine Bewertungen
- Summary of 2022 Benefit Changes: MedicalDokument5 SeitenSummary of 2022 Benefit Changes: MedicalChinnu SalimathNoch keine Bewertungen
- Pet Insurance ComparisonsDokument2 SeitenPet Insurance ComparisonsHSVC50% (2)
- ProductsDokument3 SeitenProductsYaseenNoch keine Bewertungen
- Harmonic ScalpelDokument2 SeitenHarmonic ScalpelHerman HalimNoch keine Bewertungen
- M2A1 US Census Data SearchDokument6 SeitenM2A1 US Census Data SearchragcajunNoch keine Bewertungen
- Summary of Benefits: Silver Trio Hmo 2300/70 OffexDokument12 SeitenSummary of Benefits: Silver Trio Hmo 2300/70 OffexjaroopaitummaiNoch keine Bewertungen
- The Essential Plan Chart WnyDokument1 SeiteThe Essential Plan Chart WnyJavier GramajoNoch keine Bewertungen
- Blueshield Gold Trio HMO 1500:35Dokument14 SeitenBlueshield Gold Trio HMO 1500:35jaroopaitummaiNoch keine Bewertungen
- Benefit at A GlanceDokument2 SeitenBenefit at A GlanceShiv ChauhanNoch keine Bewertungen
- Schedule of BenefitsDokument7 SeitenSchedule of BenefitsMaddy CruzNoch keine Bewertungen
- AARP UHC 2024 Benefit Highlights LA 004P FocusDokument4 SeitenAARP UHC 2024 Benefit Highlights LA 004P FocusAlaa ZaidNoch keine Bewertungen
- Book1 (Version 1)Dokument1 SeiteBook1 (Version 1)agulabNoch keine Bewertungen
- Generic Open Enrollment KitDokument22 SeitenGeneric Open Enrollment KitSteve BarrowsNoch keine Bewertungen
- Benefits Highlights 2018Dokument5 SeitenBenefits Highlights 2018Marcus CosmeNoch keine Bewertungen
- Keystone HMO Gold Preferred 4080650Dokument11 SeitenKeystone HMO Gold Preferred 4080650ANKIT SINGHNoch keine Bewertungen
- Medical Comparison Chart 2020Dokument3 SeitenMedical Comparison Chart 2020hollingermikeNoch keine Bewertungen
- Young Adult BrochureDokument5 SeitenYoung Adult BrochureahsanNoch keine Bewertungen
- Summary of Benefits: Bronze Trio Hmo 7000/70 OffexDokument12 SeitenSummary of Benefits: Bronze Trio Hmo 7000/70 OffexjaroopaitummaiNoch keine Bewertungen
- Unitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageDokument9 SeitenUnitedhealthcare Dental Hmo Plan 2022 Summary of Benefits and CoverageAdam CliftonNoch keine Bewertungen
- ConvertDokument2 SeitenConvertpham_thu_hangNoch keine Bewertungen
- Cardea Schedule of Benefits Effective Jan 1st 2021Dokument4 SeitenCardea Schedule of Benefits Effective Jan 1st 2021Wayne GajadharNoch keine Bewertungen
- Women's Reproductive Health Free Clinic: Personnel ExpensesDokument2 SeitenWomen's Reproductive Health Free Clinic: Personnel ExpensesHujale MaxamedNoch keine Bewertungen
- Photon Benefits 2022 (August)Dokument7 SeitenPhoton Benefits 2022 (August)sojithesouljaNoch keine Bewertungen
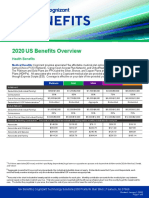
- 2020 US Benefits OverviewDokument5 Seiten2020 US Benefits OverviewrdmNoch keine Bewertungen
- Silver EssentialDokument4 SeitenSilver EssentialVasikaran PrabaharanNoch keine Bewertungen
- Special Care and Adultbasic: Comparison ChartDokument1 SeiteSpecial Care and Adultbasic: Comparison ChartjhsmalankaNoch keine Bewertungen
- Group Project 1Dokument21 SeitenGroup Project 1api-547174770Noch keine Bewertungen
- Bronze HSA 5000Dokument4 SeitenBronze HSA 5000Vasikaran PrabaharanNoch keine Bewertungen
- 2023 Open Enrollment Benefit Presenation - 11142022Dokument30 Seiten2023 Open Enrollment Benefit Presenation - 11142022margreen5Noch keine Bewertungen
- Plan ComparisonDokument4 SeitenPlan Comparisontth79hj4dvNoch keine Bewertungen
- LTIM - USA Employees Benefits Overview - 2024Dokument20 SeitenLTIM - USA Employees Benefits Overview - 2024Ramesh Kumar KNoch keine Bewertungen
- ViewyoursbcdocumentDokument12 SeitenViewyoursbcdocumentapi-531507901Noch keine Bewertungen
- 2017 Employee Benefit Highlights - Support StaffDokument8 Seiten2017 Employee Benefit Highlights - Support StaffJohn AcardoNoch keine Bewertungen
- Your Total Rewards at Newyork-PresbyterianDokument20 SeitenYour Total Rewards at Newyork-PresbyterianweiweiahNoch keine Bewertungen
- Aurora - Baseline Option 2019 SOBIDokument4 SeitenAurora - Baseline Option 2019 SOBISean MurrayNoch keine Bewertungen
- KP - Plan Summary Medical - PPODokument3 SeitenKP - Plan Summary Medical - PPOshanegbaker51Noch keine Bewertungen
- Trinity Health 020 Traditional Ppo Plan 10202021Dokument10 SeitenTrinity Health 020 Traditional Ppo Plan 10202021emily WNoch keine Bewertungen
- What You Pay in The PPO PlanDokument2 SeitenWhat You Pay in The PPO Plannathan wongNoch keine Bewertungen
- Eb 2019 Oe Guideplussbc GenericDokument19 SeitenEb 2019 Oe Guideplussbc GenericCybernaughtNoch keine Bewertungen
- Everyday Extras: Get The Same Amount Back Each Time You VisitDokument2 SeitenEveryday Extras: Get The Same Amount Back Each Time You Visitfrank.wangNoch keine Bewertungen
- Plan ComparisonDokument2 SeitenPlan ComparisonSahil JindalNoch keine Bewertungen
- Fhpv23apr231218j7r2 Veasna UkDokument6 SeitenFhpv23apr231218j7r2 Veasna UkSela SinNoch keine Bewertungen
- Kaiser Permanente: Good Health Is No SecretDokument6 SeitenKaiser Permanente: Good Health Is No SecretThomas Dominic CazneauNoch keine Bewertungen
- Plan Comparison Chart Seniorcare Hip AetnaDokument5 SeitenPlan Comparison Chart Seniorcare Hip AetnaRamonita GarciaNoch keine Bewertungen
- 76962CT0010006-01 en USDokument98 Seiten76962CT0010006-01 en USKathy ApergisNoch keine Bewertungen
- Cs Plus NYC Area Epo 2q 2009Dokument1 SeiteCs Plus NYC Area Epo 2q 2009KristieNoch keine Bewertungen
- Protect What You Treasure Most: HealthDokument12 SeitenProtect What You Treasure Most: HealthNelly HNoch keine Bewertungen
- Tricare Costs and Fees: TRICARE PRIME® COSTS (Jan. 1-Dec. 31) Tricare Select Costs (Jan. 1-Dec. 31)Dokument4 SeitenTricare Costs and Fees: TRICARE PRIME® COSTS (Jan. 1-Dec. 31) Tricare Select Costs (Jan. 1-Dec. 31)FRANKLYN TRONCONoch keine Bewertungen
- Brochure - EZCare (Nov 2022)Dokument11 SeitenBrochure - EZCare (Nov 2022)Darren ChenNoch keine Bewertungen
- Radiology of Chest Wall MassesDokument11 SeitenRadiology of Chest Wall MassesDevina BumiNoch keine Bewertungen
- Color Doppler Ultrasound System: Datasheet Release 1.0Dokument17 SeitenColor Doppler Ultrasound System: Datasheet Release 1.0Jairo Alberto Sarria VargasNoch keine Bewertungen
- HRCT Thorax Protocol Vs Low Dose CTDokument21 SeitenHRCT Thorax Protocol Vs Low Dose CTchristianhasudungan319Noch keine Bewertungen
- GENDEX 9200,9200 DDE - Service Manual - EN PDFDokument207 SeitenGENDEX 9200,9200 DDE - Service Manual - EN PDFPeter Yli100% (1)
- Project Proposal Rolands Strozs 20264Dokument21 SeitenProject Proposal Rolands Strozs 20264ivo RodriguesNoch keine Bewertungen
- Notes On Liver Colon CancerDokument16 SeitenNotes On Liver Colon CancerElleNoch keine Bewertungen
- Basics of Ecg: DR Shyama Assistant Professor General Medicine Aiims, PatnaDokument117 SeitenBasics of Ecg: DR Shyama Assistant Professor General Medicine Aiims, PatnaSimran KothariNoch keine Bewertungen
- S9 Quick Manual Version 1.0Dokument2 SeitenS9 Quick Manual Version 1.0Hea CHNoch keine Bewertungen
- Rheumatoid ArthritisDokument29 SeitenRheumatoid ArthritisvijitajayaminiNoch keine Bewertungen
- Ultrasound Criteria For Lipedema DiagnosisDokument8 SeitenUltrasound Criteria For Lipedema DiagnosisAlexandre Campos Moraes AmatoNoch keine Bewertungen
- 2 TAHPI Service PlaningDokument32 Seiten2 TAHPI Service PlaningMuhammad Ali TariqNoch keine Bewertungen
- European Tomo QC Protocol Version 1-01Dokument82 SeitenEuropean Tomo QC Protocol Version 1-01Radoi Sandina RodicaNoch keine Bewertungen
- ROOM ASSIGNMENT-RAD TECH and X-RAY - Wo Applic - JMS PDFDokument11 SeitenROOM ASSIGNMENT-RAD TECH and X-RAY - Wo Applic - JMS PDFPhilBoardResults100% (1)
- 2020 Classic Lectures in Clinical Ultrasound: Release Date: June 15, 2020 - 31.75 AMA PRA Category 1 Credit(s)Dokument5 Seiten2020 Classic Lectures in Clinical Ultrasound: Release Date: June 15, 2020 - 31.75 AMA PRA Category 1 Credit(s)Muhammad SyammNoch keine Bewertungen
- Siemens Aristos FX - Datasheet (Eng)Dokument12 SeitenSiemens Aristos FX - Datasheet (Eng)StanTofeNoch keine Bewertungen
- Z6Dokument4 SeitenZ6Carlos OjedaNoch keine Bewertungen
- Ultherapy System Instructions For UseDokument72 SeitenUltherapy System Instructions For UseEmilija Minova100% (1)
- Image Weighting and ContrastDokument30 SeitenImage Weighting and ContrastNaseem Al tajerNoch keine Bewertungen
- Liver Fibrosis ProgressDokument9 SeitenLiver Fibrosis ProgressTaufik Rizkian AsirNoch keine Bewertungen
- DC 40 Brochure - En.esDokument8 SeitenDC 40 Brochure - En.esMoi KoNoch keine Bewertungen
- Guidelines AEPCDokument9 SeitenGuidelines AEPCAlina SarbuNoch keine Bewertungen
- Time of Flight: T T 2×Dc D CDokument2 SeitenTime of Flight: T T 2×Dc D CالشاعرالطبيبالمريNoch keine Bewertungen
- Thesis RadiodiagnosisDokument8 SeitenThesis Radiodiagnosisgcq5c1pv100% (2)
- Catalogo Acuson X300Dokument8 SeitenCatalogo Acuson X300Oscar CorreaNoch keine Bewertungen
- Y-S A 3.0PL: Organization of Multi-Specialist Medical Care and Physiotherapy For Patients With TinnitusDokument13 SeitenY-S A 3.0PL: Organization of Multi-Specialist Medical Care and Physiotherapy For Patients With TinnitusPaulomds1991Noch keine Bewertungen
- Research Ism 2Dokument3 SeitenResearch Ism 2api-434957773Noch keine Bewertungen
- The Hospital: - Professional Adjustment in Nursing - LEVEL 100Dokument47 SeitenThe Hospital: - Professional Adjustment in Nursing - LEVEL 100Anning HagarNoch keine Bewertungen
- Zollinger-Ellison SyndromeDokument21 SeitenZollinger-Ellison Syndromerogelio cruzNoch keine Bewertungen
- ESR Ebook For Undergraduate Education in Radiology - 03 Contrast Agents PDFDokument113 SeitenESR Ebook For Undergraduate Education in Radiology - 03 Contrast Agents PDFANAS ALINoch keine Bewertungen
- KV-CBCT MVCTDokument6 SeitenKV-CBCT MVCTapi-280277788Noch keine Bewertungen