Das könnte Ihnen auch gefallen
- Mastitis 2Dokument25 SeitenMastitis 2Riana Pasca RoshianNoch keine Bewertungen
- Breech PresentationDokument85 SeitenBreech Presentationwidya vannesaNoch keine Bewertungen
- Early Initiation of BreastfeedingDokument2 SeitenEarly Initiation of BreastfeedingMutia Salindri Putri100% (1)
- Describes Difficulty During Labor.: EtiologyDokument6 SeitenDescribes Difficulty During Labor.: EtiologyRudelsa Agcolicol LangamanNoch keine Bewertungen
- A Study To Assess Effectiveness of Information Booklet Regarding Use of Partograph Among Midwives Working in Labour Room of Selected Hospital of Bhopal M.PDokument8 SeitenA Study To Assess Effectiveness of Information Booklet Regarding Use of Partograph Among Midwives Working in Labour Room of Selected Hospital of Bhopal M.PEditor IJTSRDNoch keine Bewertungen
- Cs On TefDokument10 SeitenCs On TefArchana SahuNoch keine Bewertungen
- Antenatal Case SheetDokument4 SeitenAntenatal Case SheetRichard SnellNoch keine Bewertungen
- Case PresentationDokument36 SeitenCase PresentationSaba TariqNoch keine Bewertungen
- Postnatal CareDokument62 SeitenPostnatal CareKonstantinos Papadakis100% (1)
- Intrauterine Growth Restriction IUGR: TH THDokument2 SeitenIntrauterine Growth Restriction IUGR: TH THZahra AlaradiNoch keine Bewertungen
- Case Study 29-APHDokument31 SeitenCase Study 29-APHZarul Naim Mohd TamiziNoch keine Bewertungen
- Placenta PreviaDokument2 SeitenPlacenta PreviaAnonymous 0C4OZmRNoch keine Bewertungen
- Post Natal CareDokument94 SeitenPost Natal CareZekariyas MulunehNoch keine Bewertungen
- Anorectal Malformations: Presented by Khushveer KaurDokument91 SeitenAnorectal Malformations: Presented by Khushveer KaurKataria DavinNoch keine Bewertungen
- Breast Pumps: PRESENTED BY: Shristi PanthaDokument16 SeitenBreast Pumps: PRESENTED BY: Shristi PanthaShristi PanthaNoch keine Bewertungen
- Breast Feeding Health TalkDokument12 SeitenBreast Feeding Health TalkSanjeet DuhanNoch keine Bewertungen
- Hyper Emesis GravidarumDokument22 SeitenHyper Emesis Gravidarumchandu ranaNoch keine Bewertungen
- Nutritional Composition of Breast MilkDokument24 SeitenNutritional Composition of Breast MilkSamuel Bagas Wahyu SantosoNoch keine Bewertungen
- Labor-Vaginal Delivery Anne Jones, 17 Years Old Case Study With Complete Solutions 2023Dokument13 SeitenLabor-Vaginal Delivery Anne Jones, 17 Years Old Case Study With Complete Solutions 2023CHARLES MAINANoch keine Bewertungen
- WHO Labour Care GuideDokument34 SeitenWHO Labour Care GuideAnkita Singh100% (1)
- 2.development of Normal PlacentaDokument55 Seiten2.development of Normal PlacentapriyaNoch keine Bewertungen
- CTG Booklet: A Quick Reference Guide For Managing CtgsDokument16 SeitenCTG Booklet: A Quick Reference Guide For Managing Ctgscirlce:twoworldsconnectedNoch keine Bewertungen
- NCP Ovarian CancerDokument6 SeitenNCP Ovarian Cancerwendy gaetosNoch keine Bewertungen
- Extremely Low Birth Weight (ELBW) InfantDokument48 SeitenExtremely Low Birth Weight (ELBW) InfanthannanyusofNoch keine Bewertungen
- Seminar On Minor DisorderDokument23 SeitenSeminar On Minor Disorderpriti pallabi100% (1)
- Govt College of Nursig Mbs Hospital, Kota: A Case Study On EclampsiaDokument21 SeitenGovt College of Nursig Mbs Hospital, Kota: A Case Study On EclampsiaShalabh JoharyNoch keine Bewertungen
- Uterine AtonyDokument20 SeitenUterine AtonyKpiebakyene Sr. MercyNoch keine Bewertungen
- Abnormal Delivery - Zhahrullail ShahidDokument12 SeitenAbnormal Delivery - Zhahrullail ShahidBadrul MunirNoch keine Bewertungen
- Harika Priyanka. K Asst. Professor AconDokument30 SeitenHarika Priyanka. K Asst. Professor AconArchana MoreyNoch keine Bewertungen
- EpisiotomyDokument18 SeitenEpisiotomyAnnapurna DangetiNoch keine Bewertungen
- Vaginal Exam GuidelineDokument6 SeitenVaginal Exam GuidelinerohitNoch keine Bewertungen
- The PlacentaDokument3 SeitenThe PlacentaLiezelNoch keine Bewertungen
- East FeedingDokument5 SeitenEast FeedingJeya vanithaNoch keine Bewertungen
- Cord Prolapse: Case ReportDokument37 SeitenCord Prolapse: Case ReportMica CumigadNoch keine Bewertungen
- PROM SANJIDA FInal 2Dokument32 SeitenPROM SANJIDA FInal 2Saiful islam RonyNoch keine Bewertungen
- Engorgement PDFDokument1 SeiteEngorgement PDFrevathidadam55555Noch keine Bewertungen
- Ectopic Pregnancy: DR .Urmila KarkiDokument27 SeitenEctopic Pregnancy: DR .Urmila KarkiBasudev chNoch keine Bewertungen
- Nursing Process Antental1Dokument11 SeitenNursing Process Antental1MANOJNoch keine Bewertungen
- 2antenatal CareDokument10 Seiten2antenatal CareuouoNoch keine Bewertungen
- Forceps DeliveryDokument13 SeitenForceps DeliveryStar AlvarezNoch keine Bewertungen
- Objectives of Aph:: To Define About APH. To List The Causes of APHDokument42 SeitenObjectives of Aph:: To Define About APH. To List The Causes of APHReena TyagiNoch keine Bewertungen
- PREMATURITYDokument40 SeitenPREMATURITYBlykeBantuganNoch keine Bewertungen
- Destructive Operation and Caesarian SectionDokument53 SeitenDestructive Operation and Caesarian SectionVijith.V.kumar0% (1)
- RH Incompatibility: Go ToDokument4 SeitenRH Incompatibility: Go ToFadhila AnasNoch keine Bewertungen
- Pap Smear: IntroductionDokument10 SeitenPap Smear: IntroductionPallaviNoch keine Bewertungen
- Breast Feeding Is The Normal Way of Providing Young Infants With The Nutrients They Need For Healthy Growth and DevelopmentDokument8 SeitenBreast Feeding Is The Normal Way of Providing Young Infants With The Nutrients They Need For Healthy Growth and Developmentdanee しNoch keine Bewertungen
- Multiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesDokument33 SeitenMultiple Pregnancy: Dr. A. Farid Abdullah, SP - OG, M.KesAndi Farid ANoch keine Bewertungen
- Fetal Biophysical Profile PDFDokument2 SeitenFetal Biophysical Profile PDFVickiNoch keine Bewertungen
- Routine Antenatal Screening DR - Amy MellorDokument3 SeitenRoutine Antenatal Screening DR - Amy MellorYwagar Ywagar100% (1)
- NCP1 - Latent PhaseDokument14 SeitenNCP1 - Latent PhasepriyankaNoch keine Bewertungen
- OB GDM CasepresDokument102 SeitenOB GDM Casepreskitten garciaNoch keine Bewertungen
- Dietary Guidelines For A Healthy Postnatal DietDokument4 SeitenDietary Guidelines For A Healthy Postnatal DietAkhila Basu100% (1)
- Evidence Based Obstetrics CareDokument49 SeitenEvidence Based Obstetrics CareSANANoch keine Bewertungen
- Abnormal Uterine ActionDokument27 SeitenAbnormal Uterine ActionSameer KumarNoch keine Bewertungen
- Medical Termination of PregnencyDokument19 SeitenMedical Termination of PregnencyTijilNoch keine Bewertungen
- ContractedDokument15 SeitenContractedswapnil3250Noch keine Bewertungen
- Uterine Malformations PDFDokument6 SeitenUterine Malformations PDFsaritha OrugantiNoch keine Bewertungen
- Breech PresentationDokument35 SeitenBreech PresentationPrince Jhessie L. AbellaNoch keine Bewertungen
- Abortion II ND Yr MSC NursingDokument121 SeitenAbortion II ND Yr MSC Nursingesthereugenia100% (1)
- Fetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsVon EverandFetal Physiological Measurements: Proceedings of the Second International Conference on Fetal and Neonatal Physiological MeasurementsPeter RolfeNoch keine Bewertungen
- Padma 25012024Dokument3 SeitenPadma 25012024Geetha SoundaryaNoch keine Bewertungen
- LA Systemic Toxicity Current PerspectiveDokument10 SeitenLA Systemic Toxicity Current PerspectiveGeetha SoundaryaNoch keine Bewertungen
- 10 1 1 550 8023 PDFDokument11 Seiten10 1 1 550 8023 PDFGeetha SoundaryaNoch keine Bewertungen
- CE (Ra1) F (SHU) PF1 (HJ VI) (KR) PFA (HJ KM) PN (KM)Dokument2 SeitenCE (Ra1) F (SHU) PF1 (HJ VI) (KR) PFA (HJ KM) PN (KM)Geetha SoundaryaNoch keine Bewertungen
- Rectal Sedation: Chapter OutlineDokument1 SeiteRectal Sedation: Chapter OutlineGeetha SoundaryaNoch keine Bewertungen
- Dr.D.K.Sriram Medical Director Dr.V.Revathi Chief Medical Officer S.No Name Morning Evening Visiting Days Our Medical TeamDokument5 SeitenDr.D.K.Sriram Medical Director Dr.V.Revathi Chief Medical Officer S.No Name Morning Evening Visiting Days Our Medical TeamGeetha SoundaryaNoch keine Bewertungen
- Blackmoney Form2Dokument2 SeitenBlackmoney Form2Geetha SoundaryaNoch keine Bewertungen
- Gi1 Teaching Staff ClinicalDokument21 SeitenGi1 Teaching Staff ClinicalGeetha SoundaryaNoch keine Bewertungen
- Medical Liquid Oxygen Tcm410-55834Dokument12 SeitenMedical Liquid Oxygen Tcm410-55834Geetha SoundaryaNoch keine Bewertungen
- LKG Holiday Assignment PDFDokument5 SeitenLKG Holiday Assignment PDFGeetha SoundaryaNoch keine Bewertungen
- INVOICEHHHDokument1 SeiteINVOICEHHHGeetha SoundaryaNoch keine Bewertungen
- TNEB Online Payment PDFDokument2 SeitenTNEB Online Payment PDFGeetha SoundaryaNoch keine Bewertungen
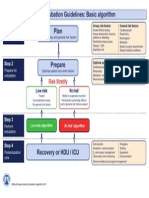
- DASExtubation Guidelines Basic AlgorithmDokument1 SeiteDASExtubation Guidelines Basic AlgorithmGeetha SoundaryaNoch keine Bewertungen
- Kannil Theriyuthu Oru Thothram NilaDokument230 SeitenKannil Theriyuthu Oru Thothram NilaSavi80% (5)
- Glossopharyngeal NeuralgiaDokument36 SeitenGlossopharyngeal NeuralgiaGeetha SoundaryaNoch keine Bewertungen
- DR AhilaDokument2 SeitenDR AhilaGeetha SoundaryaNoch keine Bewertungen
- AdenomyosisDokument1 SeiteAdenomyosisVictor GomoiuNoch keine Bewertungen
- Drug Study SitagliptinDokument3 SeitenDrug Study SitagliptinEzron Kendrick Duran50% (2)
- Electrolyte ReplacementDokument3 SeitenElectrolyte ReplacementRatih Dwi OctariaNoch keine Bewertungen
- Personal Accident Claim Form: Particulars of Insured (Company / Individual)Dokument2 SeitenPersonal Accident Claim Form: Particulars of Insured (Company / Individual)Robbie Chan100% (1)
- ATARAXIE S7 Cours Par CoursDokument251 SeitenATARAXIE S7 Cours Par CoursOussama Hamadi100% (1)
- C1 Introduction For Genzyme: Unlock Insights. Activate GrowthDokument8 SeitenC1 Introduction For Genzyme: Unlock Insights. Activate GrowthRobertFWainblatIIINoch keine Bewertungen
- Flower Horn DiseasesDokument4 SeitenFlower Horn DiseasesSandeep ModiNoch keine Bewertungen
- ATLSDokument15 SeitenATLSsouthstar9989% (9)
- Eac MsdsDokument2 SeitenEac Msdsteguh30Noch keine Bewertungen
- Proposal For Defense Group 3Dokument77 SeitenProposal For Defense Group 3Kristiene Kyle AquinoNoch keine Bewertungen
- Pathfinder 2nd Edition House Rules Compendium - GM BinderDokument119 SeitenPathfinder 2nd Edition House Rules Compendium - GM BinderBrandon PaulNoch keine Bewertungen
- Emr Policy and ProcedureDokument7 SeitenEmr Policy and Procedureapi-267965870Noch keine Bewertungen
- Astm E446 ReqDokument3 SeitenAstm E446 ReqwerwewmnlljlajkdNoch keine Bewertungen
- Ch06 Blocked Fallopian TubesDokument80 SeitenCh06 Blocked Fallopian TubesAasia Najaf SoomroNoch keine Bewertungen
- The Accidental AddictsDokument6 SeitenThe Accidental AddictsnorthandsouthnzNoch keine Bewertungen
- Site-Specific and Stoichiometric Modification of Antibodies by Bacterial TransglutaminaseDokument3 SeitenSite-Specific and Stoichiometric Modification of Antibodies by Bacterial Transglutaminasespamemail00Noch keine Bewertungen
- MSDS Berkat Saintifindo PDFDokument27 SeitenMSDS Berkat Saintifindo PDFDianSelviaNoch keine Bewertungen
- World Service Office PO Box 9999 Van Nuys, CA 91409 USADokument2 SeitenWorld Service Office PO Box 9999 Van Nuys, CA 91409 USAmustafa hezamNoch keine Bewertungen
- Journal B.cereus With PCR 2017Dokument10 SeitenJournal B.cereus With PCR 2017deryl sepradanaNoch keine Bewertungen
- PyodermaDokument19 SeitenPyodermaNewton LongjamNoch keine Bewertungen
- Autonomic Control of The Heart Cardiovascular Reflexes Student Version (7) - 2Dokument27 SeitenAutonomic Control of The Heart Cardiovascular Reflexes Student Version (7) - 2Mohammed MoghavelehNoch keine Bewertungen
- USMLE - VirusesDokument120 SeitenUSMLE - Viruseszeal7777100% (1)
- Hirayama Disease and HomoeopathyDokument11 SeitenHirayama Disease and HomoeopathyDr. Rajneesh Kumar Sharma MD Hom100% (3)
- Basic Offshore Safety Induction and Emergency Training (Bosiet) ScopeDokument31 SeitenBasic Offshore Safety Induction and Emergency Training (Bosiet) ScopePalaniraja Rajarathinam67% (6)
- Do You Know Me Flyer-Teacher VersionDokument1 SeiteDo You Know Me Flyer-Teacher VersionMaria Guy Del DucaNoch keine Bewertungen
- Ownership, Operation, Maintenance, and Inspection of Amusement Rides and DevicesDokument4 SeitenOwnership, Operation, Maintenance, and Inspection of Amusement Rides and DevicesMarlon Piarpuito Enriquez0% (1)
- Taema Monnal D2 Anaesthesia Machine - Users ManualDokument13 SeitenTaema Monnal D2 Anaesthesia Machine - Users ManualJuan carlosNoch keine Bewertungen
- Home Remedies Using Onion Prophet666Dokument2 SeitenHome Remedies Using Onion Prophet666Hussainz AliNoch keine Bewertungen
- LP + Askep CKD ON HDDokument51 SeitenLP + Askep CKD ON HDArista BaruNoch keine Bewertungen