Das könnte Ihnen auch gefallen
- Lower Limb Neurological Examination OSCE GuideDokument15 SeitenLower Limb Neurological Examination OSCE GuideLeen abusarhanNoch keine Bewertungen
- PDII Checklist Musculoskeletal StudentDokument3 SeitenPDII Checklist Musculoskeletal Studentmre07Noch keine Bewertungen
- Neonatal Case Presentation 2Dokument6 SeitenNeonatal Case Presentation 2Rabi SyedNoch keine Bewertungen
- History & Exam in SurgeryDokument22 SeitenHistory & Exam in Surgerystephen X-SILVERNoch keine Bewertungen
- Osce Stations - Blogspot.com Paediatric Respiratory ExamDokument2 SeitenOsce Stations - Blogspot.com Paediatric Respiratory ExamrohitNoch keine Bewertungen
- System Exams - Promotion Exam MusculoskeletalDokument4 SeitenSystem Exams - Promotion Exam Musculoskeletalespo176Noch keine Bewertungen
- Paeds Physical ExaminationDokument10 SeitenPaeds Physical Examinationdrwra0% (1)
- Shoulder ExamDokument24 SeitenShoulder ExamMuhammad FahmyNoch keine Bewertungen
- Paeds Complete PDFDokument176 SeitenPaeds Complete PDFjljoioiuNoch keine Bewertungen
- Neuro ProformaDokument20 SeitenNeuro ProformaPraneetha NouduriNoch keine Bewertungen
- Physical Exam Final Written Exam Study Guide 2Dokument51 SeitenPhysical Exam Final Written Exam Study Guide 2pelly3190100% (2)
- AFP Surveillance - HF Dec 1 2017Dokument39 SeitenAFP Surveillance - HF Dec 1 2017Abbi Nathi100% (1)
- History Physical FormatDokument3 SeitenHistory Physical FormatfilchibuffNoch keine Bewertungen
- YEAR 1 and 2 OSCE Revision: Author: DR Thomas PayneDokument30 SeitenYEAR 1 and 2 OSCE Revision: Author: DR Thomas Payneminayoki100% (1)
- Paediatric Notes - Moodle/Text: Paediatric Emergencies (Textbook Ch.5)Dokument6 SeitenPaediatric Notes - Moodle/Text: Paediatric Emergencies (Textbook Ch.5)Jana AldourNoch keine Bewertungen
- OSCE Checklist Newborn Baby Assessment NIPEDokument3 SeitenOSCE Checklist Newborn Baby Assessment NIPETauqeer Ahmed0% (1)
- GDD ? H@Qka A9Fk KMJ? GFK H9Cakl9F: Clinical & Toacs Fcps Examination PaediatricsDokument3 SeitenGDD ? H@Qka A9Fk KMJ? GFK H9Cakl9F: Clinical & Toacs Fcps Examination PaediatricsBabarNaeemNoch keine Bewertungen
- Case Presentation: NeurologyDokument19 SeitenCase Presentation: NeurologySydrex SarmientoNoch keine Bewertungen
- Pediatric History & Physical ExamDokument7 SeitenPediatric History & Physical ExamMelodia Turqueza GandezaNoch keine Bewertungen
- Paediatric Neurological ExaminationDokument17 SeitenPaediatric Neurological ExaminationPrabuPandianNoch keine Bewertungen
- PNS Examination 15Dokument17 SeitenPNS Examination 15NolanNoch keine Bewertungen
- Gemp3 Paediatric Clinical Examination SkillsDokument13 SeitenGemp3 Paediatric Clinical Examination SkillsAnna-Tammy HumanNoch keine Bewertungen
- RDU On Poisoning and CancerDokument24 SeitenRDU On Poisoning and CancerATHENA MINERVA MORDENONoch keine Bewertungen
- Emed - BLS - FBAO - First Aid Part2Dokument87 SeitenEmed - BLS - FBAO - First Aid Part2Princess Cate MercadoNoch keine Bewertungen
- Musculoskeletal Curriculum: History & Physical Exam of The ShoulderDokument60 SeitenMusculoskeletal Curriculum: History & Physical Exam of The Shoulderhis.thunder122100% (1)
- Procrastinotes: Rehabilitation Medicione Osce Reviewer 1Dokument14 SeitenProcrastinotes: Rehabilitation Medicione Osce Reviewer 1Edwin Elgar CruzNoch keine Bewertungen
- Approach To A Child With Cough and Difficulty in BreathingDokument23 SeitenApproach To A Child With Cough and Difficulty in BreathingKashif Burki100% (2)
- Diabetes Exam - OSCE - McMaster PresentationDokument14 SeitenDiabetes Exam - OSCE - McMaster PresentationHeather BoatsNoch keine Bewertungen
- History Taking in Pediatric Cardiac PatientDokument2 SeitenHistory Taking in Pediatric Cardiac PatientsyududNoch keine Bewertungen
- Lower Respiratory Tract Diseases - KeyDokument45 SeitenLower Respiratory Tract Diseases - KeyYugmaPandyaNoch keine Bewertungen
- Special Tests LeDokument9 SeitenSpecial Tests Lenurasyikah0% (1)
- Newborn NotesDokument44 SeitenNewborn NotesHaziq KamardinNoch keine Bewertungen
- Approach To Limping ChildDokument3 SeitenApproach To Limping ChildShamen KohNoch keine Bewertungen
- Brachial Plexus: Summary Mnemonics Clinical RelationsDokument19 SeitenBrachial Plexus: Summary Mnemonics Clinical RelationsGulmehr NoorNoch keine Bewertungen
- All Orthopedic TestsDokument7 SeitenAll Orthopedic Testschandran2679Noch keine Bewertungen
- KYPHOSCOLIOSISDokument21 SeitenKYPHOSCOLIOSISKeren SafawilNoch keine Bewertungen
- Group II Makati Medical Center m8 1Dokument107 SeitenGroup II Makati Medical Center m8 1CASSANDRAJUL VARINNoch keine Bewertungen
- Trendelenburg Test:: Hip Special TestsDokument3 SeitenTrendelenburg Test:: Hip Special TestsIulia ElenaNoch keine Bewertungen
- Neurological Examination of The Limbs TextDokument8 SeitenNeurological Examination of The Limbs Textvidur_talrejaNoch keine Bewertungen
- Meniscal Tear IE KMGDokument6 SeitenMeniscal Tear IE KMGjoanna gurtiza0% (1)
- GIT Examination - Clinical Skills With DRDokument8 SeitenGIT Examination - Clinical Skills With DRNaveen KovalNoch keine Bewertungen
- Step-Wise Approaches in Clinical Examination - SampleDokument8 SeitenStep-Wise Approaches in Clinical Examination - Samplecsbully913Noch keine Bewertungen
- Taking History in PaediatricsDokument7 SeitenTaking History in PaediatricsNikola IgnjatovicNoch keine Bewertungen
- Revalida Reviewer AsmphDokument237 SeitenRevalida Reviewer AsmphShey ShocNoch keine Bewertungen
- Examination of The Peripheral Neurological SystemDokument2 SeitenExamination of The Peripheral Neurological Systemkenners100% (12)
- Haematological Profile of Severe Acute Malnourished Children Admitted at Our InstitutionDokument4 SeitenHaematological Profile of Severe Acute Malnourished Children Admitted at Our InstitutionIJAR JOURNALNoch keine Bewertungen
- Classification of The Epilepsies: Purpose: For Clinical DiagnosisDokument25 SeitenClassification of The Epilepsies: Purpose: For Clinical Diagnosisayu rifqiNoch keine Bewertungen
- Problem-based Approach to Gastroenterology and HepatologyVon EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNoch keine Bewertungen
- Suggested Order For History and Physical Examination DocumentationDokument2 SeitenSuggested Order For History and Physical Examination DocumentationNicole BrassingtonNoch keine Bewertungen
- Grand Revalida Study Guide PDFDokument4 SeitenGrand Revalida Study Guide PDFJuanitoCabatañaLimIII100% (1)
- Obstetrics History Taking in and Examination PowerpointDokument15 SeitenObstetrics History Taking in and Examination Powerpointياسر كوثر هانيNoch keine Bewertungen
- PRO 2012 Short Case (Surgical) CompilationDokument24 SeitenPRO 2012 Short Case (Surgical) CompilationvijayaNoch keine Bewertungen
- Newborn AssessmentDokument9 SeitenNewborn AssessmentSusmita HalderNoch keine Bewertungen
- Fontanela AnormalDokument6 SeitenFontanela AnormalYac EsparrouNoch keine Bewertungen
- Neurology Exam Checklist1Dokument6 SeitenNeurology Exam Checklist1Syed AfzalNoch keine Bewertungen
- History Taking Physical ExamininationDokument41 SeitenHistory Taking Physical ExamininationAya AmerNoch keine Bewertungen
- CP UpdatedDokument45 SeitenCP UpdatedSivakumar Kathuu KarthikeyanNoch keine Bewertungen
- Normal Pediatric Developmental MilestonesDokument2 SeitenNormal Pediatric Developmental MilestonesJoel CastilloNoch keine Bewertungen
- PharmacologyDokument120 SeitenPharmacologyFluffy_iceNoch keine Bewertungen
- CNS Examination: Done by DR/ Abdullah Mohd. Jan MBBS, InternDokument37 SeitenCNS Examination: Done by DR/ Abdullah Mohd. Jan MBBS, InternBrajesh MouryaNoch keine Bewertungen
- Full Nice EpilepsyDokument152 SeitenFull Nice EpilepsywalidNoch keine Bewertungen
- Basic Medical Sciences (3rd Ed)Dokument442 SeitenBasic Medical Sciences (3rd Ed)aeyousefNoch keine Bewertungen
- Development Assessment MRCPCH Website PDFDokument1 SeiteDevelopment Assessment MRCPCH Website PDFTONY GO AWAYNoch keine Bewertungen
- 100 ECG For AKP - With AnswersDokument102 Seiten100 ECG For AKP - With AnswersaeyousefNoch keine Bewertungen
- Videos Station Collections (F) - 1Dokument25 SeitenVideos Station Collections (F) - 1aeyousefNoch keine Bewertungen
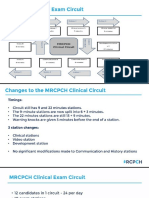
- MRCPH Clinical Exam Changes From September 2019Dokument42 SeitenMRCPH Clinical Exam Changes From September 2019aeyousefNoch keine Bewertungen
- Neurological Conditions Revison Table1Dokument8 SeitenNeurological Conditions Revison Table1aeyousefNoch keine Bewertungen
- NRPDokument8 SeitenNRPaeyousefNoch keine Bewertungen
- The Big Six Clinical GuidelineDokument41 SeitenThe Big Six Clinical GuidelineaeyousefNoch keine Bewertungen
- Clinical Cases Mrcpch1Dokument223 SeitenClinical Cases Mrcpch1aeyousef100% (1)
- Dka GuidelineDokument16 SeitenDka GuidelineGhada HusseinNoch keine Bewertungen
- DERMA TAS Pastest Derma Part 1bDokument128 SeitenDERMA TAS Pastest Derma Part 1baeyousefNoch keine Bewertungen
- Clinical Cases For MRCPCH PART 2 Applied Knowledge in PracticeDokument218 SeitenClinical Cases For MRCPCH PART 2 Applied Knowledge in Practiceaeyousef88% (16)
- Causes of Obesity in ChildrenDokument2 SeitenCauses of Obesity in ChildrenaeyousefNoch keine Bewertungen
- 10 Fluids and Electrolytes: Cleveland Clinic Intensive Review of Pediatrics, The, 2nd EditionDokument12 Seiten10 Fluids and Electrolytes: Cleveland Clinic Intensive Review of Pediatrics, The, 2nd EditionaeyousefNoch keine Bewertungen
- Pathology of The CnsDokument38 SeitenPathology of The Cnscy lifeNoch keine Bewertungen
- Nervous Tissue: Elwathiq Khalid Ibrahim Department of Anatomy University of Kassala March, 2011Dokument30 SeitenNervous Tissue: Elwathiq Khalid Ibrahim Department of Anatomy University of Kassala March, 2011Wathiq Khalid IbrahimNoch keine Bewertungen
- Febrile SeizuresDokument24 SeitenFebrile SeizuresShrikant Hemant JoshiNoch keine Bewertungen
- Ibn Sina (Avicenna) On Pathogenesis ofDokument5 SeitenIbn Sina (Avicenna) On Pathogenesis ofashfaqamarNoch keine Bewertungen
- Viral EncephalitisDokument36 SeitenViral Encephalitishqayq100% (1)
- Abnormal MoCA and Normal Range MMSE Scores in Parkinson D Without DementiaDokument15 SeitenAbnormal MoCA and Normal Range MMSE Scores in Parkinson D Without DementiadquebradasNoch keine Bewertungen
- Neural Foundations of Ayres Sensory Integration®Dokument15 SeitenNeural Foundations of Ayres Sensory Integration®Muskaan KhannaNoch keine Bewertungen
- Gait Disorders in Adults and The Elderly: A Clinical GuideDokument15 SeitenGait Disorders in Adults and The Elderly: A Clinical GuideAziznavii AmegoNoch keine Bewertungen
- Dr. Ziad Arandi (Psychiatric MCQS)Dokument16 SeitenDr. Ziad Arandi (Psychiatric MCQS)Firas Anaya100% (1)
- Welcome To My Case Study Presentation: BHPI, CRP, Savar DhakaDokument19 SeitenWelcome To My Case Study Presentation: BHPI, CRP, Savar DhakaKaushik Dipto RoyNoch keine Bewertungen
- Science 6 Nat ReviewerDokument40 SeitenScience 6 Nat ReviewerDONA FE SIADENNoch keine Bewertungen
- Conciousness As Integrated Information - Giulio Tononi PDFDokument27 SeitenConciousness As Integrated Information - Giulio Tononi PDFpetercetNoch keine Bewertungen
- Types of Cerebral Herniation and ImagingDokument13 SeitenTypes of Cerebral Herniation and ImagingPaulo LuizNoch keine Bewertungen
- Conversion (Hysteria)Dokument76 SeitenConversion (Hysteria)Viren SolankiNoch keine Bewertungen
- Frontal Lobe and Temporal Lobe Functions and SyndromesDokument48 SeitenFrontal Lobe and Temporal Lobe Functions and SyndromesShreya SharmaNoch keine Bewertungen
- Neurulation, OrganogenesisDokument2 SeitenNeurulation, OrganogenesisClaire BolalinNoch keine Bewertungen
- 243 AuditoryProcessing PDFDokument2 Seiten243 AuditoryProcessing PDFAna SousaNoch keine Bewertungen
- Biology Capsule PDFDokument15 SeitenBiology Capsule PDFShubhneetNoch keine Bewertungen
- Unconscious and Comatose Patients DR Moses KazevuDokument17 SeitenUnconscious and Comatose Patients DR Moses KazevuMoses Jr KazevuNoch keine Bewertungen
- Cerebrovascular AccidentDokument17 SeitenCerebrovascular Accidentmanisha paikarayNoch keine Bewertungen
- Movement Disorders & Multiple Sclerosis-Kumar & Clark'sDokument8 SeitenMovement Disorders & Multiple Sclerosis-Kumar & Clark'sindia2puppyNoch keine Bewertungen
- McKenzie Explained PDFDokument4 SeitenMcKenzie Explained PDFItai IzhakNoch keine Bewertungen
- Calcium Control of Neurotransmitter Release PDFDokument15 SeitenCalcium Control of Neurotransmitter Release PDFNisa Yulianti SuprahmanNoch keine Bewertungen
- Test Bank For Meeting The Physical Therapy Needs of Children 2nd Edition Susan K EffgenDokument10 SeitenTest Bank For Meeting The Physical Therapy Needs of Children 2nd Edition Susan K Effgenmonicafarmerbxtaznmodw100% (19)
- Spatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectDokument9 SeitenSpatial Neglect - Overview, Etiology, Mechanisms and Morbidities in Spatial NeglectRivulet1Noch keine Bewertungen
- Acute Vestibular Syndrome: Kevin A. Kerber, MD, MSDokument8 SeitenAcute Vestibular Syndrome: Kevin A. Kerber, MD, MSBagus Pithu Ha SpingNoch keine Bewertungen
- Brain Based Compatible Learning FinalDokument83 SeitenBrain Based Compatible Learning FinalVanessa Pangan Keller100% (1)
- Dementia in Clinical Practice PDFDokument404 SeitenDementia in Clinical Practice PDFadriricalde100% (1)
- Jezicki MozakDokument36 SeitenJezicki MozakSinisa RisticNoch keine Bewertungen
- C8e 49 Test BankDokument12 SeitenC8e 49 Test BankSali Iqra0% (1)