Das könnte Ihnen auch gefallen
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- Preparation Guidelines PDFDokument2 SeitenPreparation Guidelines PDFSourav PoddarNoch keine Bewertungen
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- MedicalPassenger TravelGuidelineDokument5 SeitenMedicalPassenger TravelGuidelinenitinNoch keine Bewertungen
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5794)
- Practice Exercises & Answers: Compiled From The Manual by Sivaram Pusapati, Japan, 2016Dokument75 SeitenPractice Exercises & Answers: Compiled From The Manual by Sivaram Pusapati, Japan, 2016SutharthanMariyappanNoch keine Bewertungen
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Application For Carriage of Medical Passengers: Passenger'S DetailDokument3 SeitenApplication For Carriage of Medical Passengers: Passenger'S DetailnitinNoch keine Bewertungen
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- File 5 - GD CaseletsDokument8 SeitenFile 5 - GD Caseletsraja89Noch keine Bewertungen
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- Eps NewsletterDokument5 SeitenEps NewsletternitinNoch keine Bewertungen
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- Domestic Travel PolicyDokument10 SeitenDomestic Travel PolicynitinNoch keine Bewertungen
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Age DataDokument40 SeitenAge DatanitinNoch keine Bewertungen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
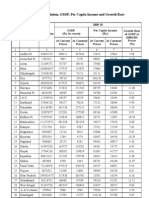
- Statewise GSDP PCI and G.RDokument3 SeitenStatewise GSDP PCI and G.RArchit SingalNoch keine Bewertungen
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- India: WHO and UNICEF Estimates of Immunization Coverage: 2016 RevisionDokument18 SeitenIndia: WHO and UNICEF Estimates of Immunization Coverage: 2016 RevisionnitinNoch keine Bewertungen
- Talk Infants Color Office PDFDokument4 SeitenTalk Infants Color Office PDFnitinNoch keine Bewertungen
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Factsheet JharkhandDokument132 SeitenFactsheet Jharkhandnitin0% (1)
- ITC's E-ChoupalDokument13 SeitenITC's E-ChoupalRonakpokharna0% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- Annual Health Report 2012-13 NewDokument58 SeitenAnnual Health Report 2012-13 NewnitinNoch keine Bewertungen
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (73)
- Factsheet JharkhandDokument132 SeitenFactsheet Jharkhandnitin0% (1)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (344)
- Etah - PIP ReportDokument29 SeitenEtah - PIP ReportnitinNoch keine Bewertungen
- RC TonesDokument2 SeitenRC TonesnitinNoch keine Bewertungen
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- RC TonesDokument2 SeitenRC TonesnitinNoch keine Bewertungen
- Assignment 3 Sec B PGP 21 215 & 076Dokument1 SeiteAssignment 3 Sec B PGP 21 215 & 076nitinNoch keine Bewertungen
- Nashik 1Dokument3 SeitenNashik 1JayshreeNoch keine Bewertungen
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- FlightDokument2 SeitenFlightMalai SelvanNoch keine Bewertungen
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1090)
- Adamson University: Budget and Operating Procedures of Barangay 66 Zone 8 Pasay City, Metro ManilaDokument30 SeitenAdamson University: Budget and Operating Procedures of Barangay 66 Zone 8 Pasay City, Metro ManilaJohn Mark EsguerraNoch keine Bewertungen
- 2GO Group, Inc. - SMIC SEC Form 19-1 (Tender Offer Report) (Copy Furnished 2GO) 22march2021Dokument69 Seiten2GO Group, Inc. - SMIC SEC Form 19-1 (Tender Offer Report) (Copy Furnished 2GO) 22march2021Roze JustinNoch keine Bewertungen
- Basantkumar - PNBDokument9 SeitenBasantkumar - PNBskhushbusahniNoch keine Bewertungen
- IFMIS Bill PreparationDokument7 SeitenIFMIS Bill PreparationAskani Kurumaiah0% (1)
- Muhammad ShahbazDokument30 SeitenMuhammad ShahbazKamran ArshafNoch keine Bewertungen
- S A 20190623Dokument4 SeitenS A 20190623Ralph Bernard Dela RosaNoch keine Bewertungen
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- GMM Application FormDokument2 SeitenGMM Application FormZaw Moe KhineNoch keine Bewertungen
- Definition of Bank: According To CrowtherDokument77 SeitenDefinition of Bank: According To CrowtherSonam KhanNoch keine Bewertungen
- Mercantile Law Bar Exam Q&ADokument26 SeitenMercantile Law Bar Exam Q&AVerdeth Marie Wagan100% (1)
- Chapter 10 Purchase and Payment Cycle: Learning ObjectivesDokument19 SeitenChapter 10 Purchase and Payment Cycle: Learning ObjectivesSweet EmmeNoch keine Bewertungen
- Volume02.indd 2Dokument3 SeitenVolume02.indd 2DanniNoch keine Bewertungen
- Maharashtra State Electricity Distribution Co. LTD.: For Any Queries On This Bill Please Contact MSEDCL CallDokument1 SeiteMaharashtra State Electricity Distribution Co. LTD.: For Any Queries On This Bill Please Contact MSEDCL CallRamboNoch keine Bewertungen
- Cases 5Dokument4 SeitenCases 5Thoughts and More ThoughtsNoch keine Bewertungen
- Wa0003Dokument81 SeitenWa0003irfanNoch keine Bewertungen
- Quickbooks Online CertificatDokument137 SeitenQuickbooks Online CertificatRandy Fernandez100% (6)
- BPML Master List-ALLDokument124 SeitenBPML Master List-ALLSurya Damarla100% (2)
- Exp 1Dokument2 SeitenExp 1Amey Pashte50% (2)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Bar Questions in Negotiable InstrumentDokument13 SeitenBar Questions in Negotiable InstrumentMary Neil GalvisoNoch keine Bewertungen
- Mystmt - 2022 11 09Dokument5 SeitenMystmt - 2022 11 09sylvia100% (2)
- Goa With Mahableshwar Lonavala Imagica - Compass Holidays & AdventureDokument7 SeitenGoa With Mahableshwar Lonavala Imagica - Compass Holidays & Adventureએકલોએન્જીનીયરNoch keine Bewertungen
- Bangladesh Automated Clearing House Payment and Settlement SystemsDokument4 SeitenBangladesh Automated Clearing House Payment and Settlement SystemsboderhaddiNoch keine Bewertungen
- Service AddressDokument1 SeiteService Addresskeogh takakoNoch keine Bewertungen
- 001jan172020 3 PDFDokument4 Seiten001jan172020 3 PDFSteven EnglishNoch keine Bewertungen
- Account StatementDokument12 SeitenAccount StatementbadramostuNoch keine Bewertungen
- Effective Small Business Management 10th Edition Scarborough Test BankDokument31 SeitenEffective Small Business Management 10th Edition Scarborough Test Bankreginagwyn0157y100% (32)
- Sosa V Atty. MendozaDokument6 SeitenSosa V Atty. MendozacyrinecalNoch keine Bewertungen
- Settlement LetterDokument1 SeiteSettlement LetterAmrish VenkatesanNoch keine Bewertungen
- Change Your Life PDF FreeDokument51 SeitenChange Your Life PDF FreeJochebed MukandaNoch keine Bewertungen
- When Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfVon EverandWhen Helping Hurts: How to Alleviate Poverty Without Hurting the Poor . . . and YourselfBewertung: 5 von 5 Sternen5/5 (36)
- Life at the Bottom: The Worldview That Makes the UnderclassVon EverandLife at the Bottom: The Worldview That Makes the UnderclassBewertung: 5 von 5 Sternen5/5 (30)
- The Great Displacement: Climate Change and the Next American MigrationVon EverandThe Great Displacement: Climate Change and the Next American MigrationBewertung: 4.5 von 5 Sternen4.5/5 (32)