Das könnte Ihnen auch gefallen
- 2018 DystoniaDokument23 Seiten2018 DystoniaTony NgNoch keine Bewertungen
- Multiple Choice Questions Multiple Choice QuestionsDokument19 SeitenMultiple Choice Questions Multiple Choice QuestionsKay VinesNoch keine Bewertungen
- Neck Lumps, (Cervical Masses) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandNeck Lumps, (Cervical Masses) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Rotation in RadiologyDokument6 SeitenRotation in Radiologyminci sensei100% (3)
- Case Study On Prostate CancerDokument16 SeitenCase Study On Prostate Cancerferdz02100% (5)
- Extensive Research Proves Vaccines Are DeadlyDokument70 SeitenExtensive Research Proves Vaccines Are DeadlyVigilantCitizen100% (5)
- A Simple Guide to Different Types of Polyps, Diagnosis, Treatment and Related ConditionsVon EverandA Simple Guide to Different Types of Polyps, Diagnosis, Treatment and Related ConditionsNoch keine Bewertungen
- Uterine Myoma CPDokument44 SeitenUterine Myoma CPCristina L. JaysonNoch keine Bewertungen
- Biochemistry IntroductionDokument72 SeitenBiochemistry IntroductionNatasha Jean100% (1)
- Neoplastic DisordersDokument36 SeitenNeoplastic DisordersJSeasharkNoch keine Bewertungen
- Mediastinal Tumors, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandMediastinal Tumors, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- 432 eDokument404 Seiten432 eIJAZ M RAHMANNoch keine Bewertungen
- Module Cellular AberrationDokument43 SeitenModule Cellular AberrationJojo JustoNoch keine Bewertungen
- Osteogenic Sarcoma (Osteosarcoma)Dokument12 SeitenOsteogenic Sarcoma (Osteosarcoma)Carmella CaritosNoch keine Bewertungen
- Parapneumonic Pleural Effusions and Empyema Thoracis - Background, Pathophysiology, EpidemiologyDokument4 SeitenParapneumonic Pleural Effusions and Empyema Thoracis - Background, Pathophysiology, EpidemiologyLorentina Den PanjaitanNoch keine Bewertungen
- EPS 001 Incubating and Hatching Eggs1 PDFDokument13 SeitenEPS 001 Incubating and Hatching Eggs1 PDFsanthoshNoch keine Bewertungen
- PCR, RT-PCR, Nested-Pcr, Multiplex PCR, Quantitative PCRDokument116 SeitenPCR, RT-PCR, Nested-Pcr, Multiplex PCR, Quantitative PCRYunizardiNoch keine Bewertungen
- Uveitis WorkupDokument75 SeitenUveitis WorkupGopal RaoNoch keine Bewertungen
- Biopsy in Oral SurgeryDokument45 SeitenBiopsy in Oral SurgeryMahamoud IsmailNoch keine Bewertungen
- Grade9 STE Con.-Chem. Q4 Module-3 Wk4 ADMDokument20 SeitenGrade9 STE Con.-Chem. Q4 Module-3 Wk4 ADMChelzy Catabas75% (4)
- Cervical Cancer: By. Ms. MurtiningsihDokument30 SeitenCervical Cancer: By. Ms. MurtiningsihraiNoch keine Bewertungen
- Staging and Grading CancerDokument20 SeitenStaging and Grading CancerSillent Kaze Of FKGNoch keine Bewertungen
- ÔN TẬP TỰ LUẬN TA YSDokument5 SeitenÔN TẬP TỰ LUẬN TA YS10 Lê Viết Hiển 12.13Noch keine Bewertungen
- Ministry of Education and Science of The Russian FederationDokument14 SeitenMinistry of Education and Science of The Russian Federationomkargawade755Noch keine Bewertungen
- 2018 FallDokument7 Seiten2018 Fallyasser farhanNoch keine Bewertungen
- Case Study: Breast CancerDokument72 SeitenCase Study: Breast CancerJoy Mariel Isadora BurgosNoch keine Bewertungen
- Modul English 2 (FIKA)Dokument54 SeitenModul English 2 (FIKA)SelviNoch keine Bewertungen
- Immune System DisordersDokument6 SeitenImmune System DisordersMiss OriginalNoch keine Bewertungen
- Anapath - Dr. Saad Khairallah - Session 1Dokument5 SeitenAnapath - Dr. Saad Khairallah - Session 1Nagham BazziNoch keine Bewertungen
- Biology Investigatory Project CancerDokument11 SeitenBiology Investigatory Project Canceranonymous user 345Noch keine Bewertungen
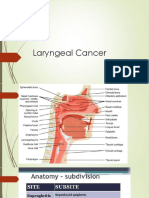
- Laryngeal Cancer 1Dokument49 SeitenLaryngeal Cancer 1Kpj KpjNoch keine Bewertungen
- Paguio, Leslie BSN 3-C Cellular-AberrationDokument20 SeitenPaguio, Leslie BSN 3-C Cellular-AberrationLeslie PaguioNoch keine Bewertungen
- Lesson 3 Cancer and CarcinogenDokument24 SeitenLesson 3 Cancer and CarcinogenKhaiyir NoyaNoch keine Bewertungen
- What Is The Brain?Dokument34 SeitenWhat Is The Brain?Sasikumar ChakkarapaniNoch keine Bewertungen
- Cancer of The OesophagusDokument44 SeitenCancer of The OesophagusAmirahShalehaNoch keine Bewertungen
- Modul English 2 (FIKA)Dokument54 SeitenModul English 2 (FIKA)Fadhlan PiyanNoch keine Bewertungen
- CASE ANALYSIS - Nasopharyngeal CancerDokument8 SeitenCASE ANALYSIS - Nasopharyngeal CancerTerry Mae Atilazal SarciaNoch keine Bewertungen
- Case Study FistulectomyDokument94 SeitenCase Study FistulectomyQuolette Constante80% (5)
- Esophageal CancerDokument4 SeitenEsophageal CancerhilcontiongsonNoch keine Bewertungen
- Cancer de LaringeDokument35 SeitenCancer de LaringejjpbNoch keine Bewertungen
- Penis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsVon EverandPenis Cancer, A Simple Guide To The Condition, Treatment And Related ConditionsNoch keine Bewertungen
- Oncology NotesDokument7 SeitenOncology NotesRochel Mae LomedaNoch keine Bewertungen
- Review of The TheoryDokument11 SeitenReview of The TheoryPriskaCliquersNoch keine Bewertungen
- AVYSDokument7 SeitenAVYSLâm Ngọc Bảo ChiNoch keine Bewertungen
- Define Colorectal CancerDokument8 SeitenDefine Colorectal Cancermiss latteNoch keine Bewertungen
- LP TMSDokument17 SeitenLP TMSEkoBudiartoNoch keine Bewertungen
- CancerDokument12 SeitenCancerUmair MalikNoch keine Bewertungen
- Homeopathic Heritage-Anorectal DisordersDokument6 SeitenHomeopathic Heritage-Anorectal DisordersDhanya G NairNoch keine Bewertungen
- Laporan Ca Serviks Fix PrintDokument31 SeitenLaporan Ca Serviks Fix PrintTeofilus Dani PNoch keine Bewertungen
- LECTURE RadPatho Complete 1Dokument69 SeitenLECTURE RadPatho Complete 1Soleil SierraNoch keine Bewertungen
- Tumor GinjalDokument26 SeitenTumor GinjalElisa NurmahidaNoch keine Bewertungen
- Soft Tissue TumorsDokument570 SeitenSoft Tissue TumorsGeo GrigoreNoch keine Bewertungen
- Uterine Cancer HandoutsDokument3 SeitenUterine Cancer Handoutslaurie.charlynjaneNoch keine Bewertungen
- Makalah B.Inggris Kel.6 CancerDokument13 SeitenMakalah B.Inggris Kel.6 Cancernurfasinta7Noch keine Bewertungen
- Cellular Growth and AberrationsDokument20 SeitenCellular Growth and Aberrationspyongjong100% (1)
- Myoma CaseDokument50 SeitenMyoma CasePopey MooreNoch keine Bewertungen
- The Pathology of Neoplasia: March 2019Dokument17 SeitenThe Pathology of Neoplasia: March 2019Mian KhanNoch keine Bewertungen
- CHE 101 Term PaperDokument16 SeitenCHE 101 Term PaperFuzail KhanNoch keine Bewertungen
- Medical Laborotoray: Faculty of Health Science. Department of Name: Abdirahman Yasin AhmedDokument6 SeitenMedical Laborotoray: Faculty of Health Science. Department of Name: Abdirahman Yasin AhmedAbdirahman YazinNoch keine Bewertungen
- Salivary Gland Disorder ScenarioDokument5 SeitenSalivary Gland Disorder ScenarioKemas IrsanNoch keine Bewertungen
- Class-Xii-Biology Project-2023-24Dokument16 SeitenClass-Xii-Biology Project-2023-24soumyaranjanmahakud5Noch keine Bewertungen
- 12 - Oral BiopsyDokument11 Seiten12 - Oral BiopsyMahmoud TayseerNoch keine Bewertungen
- Kidney Uyd enDokument20 SeitenKidney Uyd enJohn MillerNoch keine Bewertungen
- A Guide To Succeeding in The Df1 Interview (Sample Pages Only)Dokument15 SeitenA Guide To Succeeding in The Df1 Interview (Sample Pages Only)jaipald9067% (3)
- NeuroblastomaDokument4 SeitenNeuroblastomaGeleine Curutan - OniaNoch keine Bewertungen
- Resume Materi Presentasi EnglishDokument6 SeitenResume Materi Presentasi EnglishBunda SyifaNoch keine Bewertungen
- Pancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsVon EverandPancoast Syndrome, (Apical Lung Cancer) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNoch keine Bewertungen
- Litsearch UreaDokument126 SeitenLitsearch Ureaemmet11100% (1)
- Infection and Tumorigenesis of Biomaterials by Smit Prajapati-200280103028 and Yukta Dodia - 200280103052Dokument18 SeitenInfection and Tumorigenesis of Biomaterials by Smit Prajapati-200280103028 and Yukta Dodia - 200280103052Yukta DodiaNoch keine Bewertungen
- Animal Cell StructureDokument4 SeitenAnimal Cell StructureKella OrtegaNoch keine Bewertungen
- Peran BF Dalam Pandemi Covid-VaksinDokument28 SeitenPeran BF Dalam Pandemi Covid-VaksinFara EsterNoch keine Bewertungen
- Luminescent ATP Detection Assay Kit Ab113849 Luminescent ATP Detection Assay Kit Ab113849Dokument4 SeitenLuminescent ATP Detection Assay Kit Ab113849 Luminescent ATP Detection Assay Kit Ab113849carlosNoch keine Bewertungen
- Pertemuan 8. TDM Atau PKODDokument43 SeitenPertemuan 8. TDM Atau PKODBudi SayogaNoch keine Bewertungen
- Jove Materials 3064 Aseptic Laboratory Techniques Plating Methods PDFDokument4 SeitenJove Materials 3064 Aseptic Laboratory Techniques Plating Methods PDFChandan Kumar RayNoch keine Bewertungen
- Bacteriophage MCQsDokument3 SeitenBacteriophage MCQsMahi ShafiqueNoch keine Bewertungen
- Microbiology SyllabusDokument56 SeitenMicrobiology SyllabusYaswanth SinhaNoch keine Bewertungen
- Liver Fibrosis: Causes and Methods of Assessment, A ReviewDokument11 SeitenLiver Fibrosis: Causes and Methods of Assessment, A ReviewVICKI ANDREANNoch keine Bewertungen
- Nir Tononi TiCS 2010 Dreaming449Dokument13 SeitenNir Tononi TiCS 2010 Dreaming449jswzzNoch keine Bewertungen
- Bio 473 Reproductive Endocrinology Lab Compiled LabDokument10 SeitenBio 473 Reproductive Endocrinology Lab Compiled Labapi-253602935Noch keine Bewertungen
- Excretory ProductsDokument8 SeitenExcretory ProductsmatinNoch keine Bewertungen
- A Review On Dermatitis HerpetiformisDokument7 SeitenA Review On Dermatitis HerpetiformisjessicaNoch keine Bewertungen
- Intro To Genetics WebQuestDokument3 SeitenIntro To Genetics WebQuestFRANKLIN Ofori100% (1)
- Genetics in Pedo PDFDokument4 SeitenGenetics in Pedo PDFhetal majeethiaNoch keine Bewertungen
- Infeksi Alami Virus Rabies Pada Anjing: Studi Morfopatologi Dan ImunohistokimiaDokument63 SeitenInfeksi Alami Virus Rabies Pada Anjing: Studi Morfopatologi Dan ImunohistokimiaMuhammad KikiNoch keine Bewertungen
- Bartter Syndrome: ScapeDokument21 SeitenBartter Syndrome: ScapeAl DiNoch keine Bewertungen
- FIGO Releases New Guidelines To Combat Pre-Eclampsia - FIGODokument4 SeitenFIGO Releases New Guidelines To Combat Pre-Eclampsia - FIGOIgnasius HansNoch keine Bewertungen
- Journal of Neurology Volume 256 Issue 3 2009 (Doi 10.1007/s00415-009-0149-2) T. Lempert H. Neuhauser - Epidemiology of Vertigo, Migraine and Vestibular MigraineDokument6 SeitenJournal of Neurology Volume 256 Issue 3 2009 (Doi 10.1007/s00415-009-0149-2) T. Lempert H. Neuhauser - Epidemiology of Vertigo, Migraine and Vestibular MigraineDevi Arnes SimanjuntakNoch keine Bewertungen
- DAPI (4',6-Diamidine-2'-Phenylindole Dihydrochloride) : Cat. No. 10 236 276 001Dokument2 SeitenDAPI (4',6-Diamidine-2'-Phenylindole Dihydrochloride) : Cat. No. 10 236 276 001Estefani BlancasNoch keine Bewertungen
- 19 Literature Review - Primary MyelofibrosisDokument10 Seiten19 Literature Review - Primary MyelofibrosisMonica CalisayaNoch keine Bewertungen
- Etiopathogenesis of Diabetes MellitusDokument35 SeitenEtiopathogenesis of Diabetes MellitusironNoch keine Bewertungen