Das könnte Ihnen auch gefallen
- Grit: The Power of Passion and PerseveranceVon EverandGrit: The Power of Passion and PerseveranceBewertung: 4 von 5 Sternen4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Von EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Bewertung: 4 von 5 Sternen4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeVon EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeBewertung: 4 von 5 Sternen4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItVon EverandNever Split the Difference: Negotiating As If Your Life Depended On ItBewertung: 4.5 von 5 Sternen4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceVon EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceBewertung: 4 von 5 Sternen4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersVon EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersBewertung: 4.5 von 5 Sternen4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeVon EverandShoe Dog: A Memoir by the Creator of NikeBewertung: 4.5 von 5 Sternen4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingVon EverandThe Little Book of Hygge: Danish Secrets to Happy LivingBewertung: 3.5 von 5 Sternen3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureVon EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureBewertung: 4.5 von 5 Sternen4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryVon EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryBewertung: 3.5 von 5 Sternen3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealVon EverandOn Fire: The (Burning) Case for a Green New DealBewertung: 4 von 5 Sternen4/5 (74)
- The Emperor of All Maladies: A Biography of CancerVon EverandThe Emperor of All Maladies: A Biography of CancerBewertung: 4.5 von 5 Sternen4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaVon EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaBewertung: 4.5 von 5 Sternen4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaVon EverandThe Unwinding: An Inner History of the New AmericaBewertung: 4 von 5 Sternen4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnVon EverandTeam of Rivals: The Political Genius of Abraham LincolnBewertung: 4.5 von 5 Sternen4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyVon EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyBewertung: 3.5 von 5 Sternen3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreVon EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreBewertung: 4 von 5 Sternen4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Von EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Bewertung: 4.5 von 5 Sternen4.5/5 (121)
- Her Body and Other Parties: StoriesVon EverandHer Body and Other Parties: StoriesBewertung: 4 von 5 Sternen4/5 (821)
- Retensio PlasentaDokument3 SeitenRetensio PlasentaAnonymous c4GVTgkvNoch keine Bewertungen
- Med Ward JournalDokument1 SeiteMed Ward JournallordwinjohnbernardoNoch keine Bewertungen
- Biodentine PulpotomyDokument3 SeitenBiodentine PulpotomyDANIELA TOLOZANoch keine Bewertungen
- Nursing Fundamentals Test 1 Study GuideDokument15 SeitenNursing Fundamentals Test 1 Study GuideJasmin VasquezNoch keine Bewertungen
- Faculty of Nursing Zagazig University Nursing Administration 4 Year ExamDokument16 SeitenFaculty of Nursing Zagazig University Nursing Administration 4 Year ExamserviceNoch keine Bewertungen
- Our Process For Counseling ServicesDokument1 SeiteOur Process For Counseling ServicesPDM319100% (1)
- EthicsDokument24 SeitenEthicsAME DENTAL COLLEGE RAICHUR, KARNATAKANoch keine Bewertungen
- Moa - Cuta Farmers Multi-Purpose Cooperative PDFDokument6 SeitenMoa - Cuta Farmers Multi-Purpose Cooperative PDFLucy Marie RamirezNoch keine Bewertungen
- Provisional Result For Round-1 UG 2021Dokument723 SeitenProvisional Result For Round-1 UG 2021Aditya Banerjee100% (1)
- Drug Study 1Dokument5 SeitenDrug Study 1Arcee Feb Dela PazNoch keine Bewertungen
- In-Vehicle Health and Wellness: The New EssentialDokument22 SeitenIn-Vehicle Health and Wellness: The New EssentialSriram NatarajanNoch keine Bewertungen
- HPV - 2Dokument10 SeitenHPV - 2Apd. IDNoch keine Bewertungen
- Hormonal Physiology of Childbearing All Fact SheetsDokument18 SeitenHormonal Physiology of Childbearing All Fact SheetsFelix MolinaNoch keine Bewertungen
- Dopunska Lista Lijekova - Po Dijelovima - Web - Stupa Na Snagu - 23 - 06 - 2022Dokument256 SeitenDopunska Lista Lijekova - Po Dijelovima - Web - Stupa Na Snagu - 23 - 06 - 2022Alma FazlićNoch keine Bewertungen
- Historical Evolution of N.researchDokument26 SeitenHistorical Evolution of N.researchAnju Margaret100% (1)
- HWWB Concepts of Rehabilitation PDFDokument101 SeitenHWWB Concepts of Rehabilitation PDFprachi sontakkeNoch keine Bewertungen
- Malingering 4Dokument7 SeitenMalingering 4Vedora Angelia GultomNoch keine Bewertungen
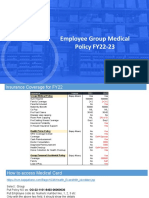
- Employee Group Medical Policy FY22-23: Merchant ExperienceDokument7 SeitenEmployee Group Medical Policy FY22-23: Merchant ExperienceLokesh SharmaNoch keine Bewertungen
- Jdo Vol 64 UpdatedDokument85 SeitenJdo Vol 64 UpdatedKanchit SuwanswadNoch keine Bewertungen
- Hepatitis B in PregnancyDokument46 SeitenHepatitis B in Pregnancycitra dewiNoch keine Bewertungen
- Paediatrics Case History Format by S.P.Kamthankar PDFDokument10 SeitenPaediatrics Case History Format by S.P.Kamthankar PDFManisha PatelNoch keine Bewertungen
- App 2021 AcogDokument26 SeitenApp 2021 AcogFernanda Copete Yolianis100% (1)
- Power and Politics in NursingDokument14 SeitenPower and Politics in NursingRufus Raj100% (2)
- BCPC Indicators For Child Friendly 2022Dokument18 SeitenBCPC Indicators For Child Friendly 2022Villanueva YuriNoch keine Bewertungen
- DOH Standards For Breast Cancer ScreeningDokument23 SeitenDOH Standards For Breast Cancer ScreeningBasil al-hashaikehNoch keine Bewertungen
- HTTP Indian BloggerDokument5 SeitenHTTP Indian BloggerpnrkumarNoch keine Bewertungen
- Orphan DrugsDokument3 SeitenOrphan Drugslisawong87Noch keine Bewertungen
- Assessing Healthcare Service Quality: A Comparative Study of Patient Treatment TypesDokument16 SeitenAssessing Healthcare Service Quality: A Comparative Study of Patient Treatment TypeshariiNoch keine Bewertungen
- Evaluascdc Hiv MethodDokument11 SeitenEvaluascdc Hiv MethodmasaruddinNoch keine Bewertungen
- Pernyataan Persetujuan Pemberian Informasi Medis Release of Medical Information Consent FormDokument1 SeitePernyataan Persetujuan Pemberian Informasi Medis Release of Medical Information Consent FormInta SugiartoNoch keine Bewertungen