Das könnte Ihnen auch gefallen
- A Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersVon EverandA Manual of the Operations of Surgery: For the Use of Senior Students, House Surgeons, and Junior PractitionersNoch keine Bewertungen
- Regional Anes 5Dokument13 SeitenRegional Anes 5Shiva Kumar P SNoch keine Bewertungen
- MinitrephDokument8 SeitenMinitrephdisk_la_poduNoch keine Bewertungen
- Pediatric Laparoscopic Inguinal Hernia Repair - A Review of Techniques - A SAGES Wiki ArticleDokument30 SeitenPediatric Laparoscopic Inguinal Hernia Repair - A Review of Techniques - A SAGES Wiki ArticleAndri Feisal NasutionNoch keine Bewertungen
- ESSURE Package Insert 0Dokument55 SeitenESSURE Package Insert 0Amy MishicaNoch keine Bewertungen
- EZ IO For Buncombe County ParamedicsDokument3 SeitenEZ IO For Buncombe County ParamedicscaffeineintolerantNoch keine Bewertungen
- EN CS 4 DA NL FR DE EL HU IT NO PL PT ES SV: MedicalDokument48 SeitenEN CS 4 DA NL FR DE EL HU IT NO PL PT ES SV: MedicalKhushboo WarhadeNoch keine Bewertungen
- Kugel Repair For HerniasDokument21 SeitenKugel Repair For HerniasElias Emmanuel JaimeNoch keine Bewertungen
- Ovariectomy Via Colpotomy ApproachDokument5 SeitenOvariectomy Via Colpotomy ApproachMeredithWindhorseHudes-Lowder100% (1)
- Mandibular SwingDokument12 SeitenMandibular SwingDr. T. Balasubramanian100% (4)
- DcsDokument4 SeitenDcsdisk_la_podu100% (1)
- Section Iic Suturing Techniques 2015Dokument13 SeitenSection Iic Suturing Techniques 2015André Pinheiro de AraújoNoch keine Bewertungen
- Closure in Lap PDFDokument10 SeitenClosure in Lap PDFpritiNoch keine Bewertungen
- Icrovascular Techniques: Tor ChiuDokument8 SeitenIcrovascular Techniques: Tor ChiuAlNoch keine Bewertungen
- Nur 146 RleDokument47 SeitenNur 146 RleKeziah Marie Chua Santa-AnaNoch keine Bewertungen
- Vertical Partial Laryngectomy An AtlasDokument14 SeitenVertical Partial Laryngectomy An AtlasDr. T. Balasubramanian100% (2)
- Practical Techniques in Injury Management: Casts and SplintsDokument30 SeitenPractical Techniques in Injury Management: Casts and SplintsBodescu Adrian100% (1)
- Laparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Dokument4 SeitenLaparoscopic Course: General Principles of Laparoscopy: Specific Aspects of Transperitoneal Access (R.Bollens)Anuj MisraNoch keine Bewertungen
- NYSORA Thoracic Paravertebral BlockDokument16 SeitenNYSORA Thoracic Paravertebral BlockYee Yeow100% (1)
- Y-Tec ProcedureDokument6 SeitenY-Tec ProcedurevennaNoch keine Bewertungen
- Surgical Atlas Primary Hypospadias Repair With Buccal MucosaDokument19 SeitenSurgical Atlas Primary Hypospadias Repair With Buccal MucosaNurul Simatupang100% (1)
- New Technique Combined With Suture and PDFDokument8 SeitenNew Technique Combined With Suture and PDFzachvuhaNoch keine Bewertungen
- Full Endoscopic Bilateral Over The Top Decompression in LumbarDokument6 SeitenFull Endoscopic Bilateral Over The Top Decompression in Lumbarckilincer2Noch keine Bewertungen
- Dall Miles Surgical ProtocolDokument16 SeitenDall Miles Surgical Protocolfarnaz_2647334Noch keine Bewertungen
- Techniques: Suturing and Knot Tying in Laparoscopy: TechniqueDokument6 SeitenTechniques: Suturing and Knot Tying in Laparoscopy: TechniqueAlldin AhmeetovicNoch keine Bewertungen
- H&N - Cervical Plexus BlockDokument9 SeitenH&N - Cervical Plexus BlockJane KoNoch keine Bewertungen
- Tubal SterilizationDokument19 SeitenTubal SterilizationEndaleNoch keine Bewertungen
- Bandage Wrapping - Bandaging Techniques: First AidDokument6 SeitenBandage Wrapping - Bandaging Techniques: First AidangelyaniNoch keine Bewertungen
- Air Way Equipment 2Dokument29 SeitenAir Way Equipment 2Alaa OmarNoch keine Bewertungen
- Pectus Excavatum: An Informational Brochure For Patients and Families With "Caved-In" ChestDokument11 SeitenPectus Excavatum: An Informational Brochure For Patients and Families With "Caved-In" ChestdanesiafiarekaNoch keine Bewertungen
- Pha Co EmulsificationDokument18 SeitenPha Co EmulsificationLucky PermanaNoch keine Bewertungen
- Principles of Laparoscopic Surgery.Dokument1 SeitePrinciples of Laparoscopic Surgery.abinash chihnaraNoch keine Bewertungen
- 2013 TTA Rapid ProtocolDokument5 Seiten2013 TTA Rapid ProtocolInstrulife OostkampNoch keine Bewertungen
- Perio 5Dokument7 SeitenPerio 5Meiz JaleelNoch keine Bewertungen
- Subarachnoid Block TOTW 059 2007 PDFDokument14 SeitenSubarachnoid Block TOTW 059 2007 PDFilham fadlilahNoch keine Bewertungen
- Et IntubationDokument3 SeitenEt IntubationCherry L. M. JaramilloNoch keine Bewertungen
- EnucleationDokument6 SeitenEnucleationRameez SarwarNoch keine Bewertungen
- Caldwell Luc IncisionDokument3 SeitenCaldwell Luc IncisionabdullahNoch keine Bewertungen
- Mecegah Komplikasi SicsDokument9 SeitenMecegah Komplikasi Sicsinna_luv_u9006Noch keine Bewertungen
- Nexgen Complete Knee Solution: ZimmerDokument37 SeitenNexgen Complete Knee Solution: Zimmerflo1987Noch keine Bewertungen
- Anesthesia For Healthy Rabbits - Veterinary Anesthesia Update - VINDokument8 SeitenAnesthesia For Healthy Rabbits - Veterinary Anesthesia Update - VINCristian FloreaNoch keine Bewertungen
- Bilateral Sagittal Split OsteotomyDokument8 SeitenBilateral Sagittal Split OsteotomydoctorniravNoch keine Bewertungen
- DFGDDokument16 SeitenDFGDAlexander MikerovNoch keine Bewertungen
- Canmedaj01567 0040Dokument2 SeitenCanmedaj01567 0040Luqmanul HakimNoch keine Bewertungen
- Negative: Quadrant Tray Section TrayDokument10 SeitenNegative: Quadrant Tray Section Trayapi-19967864Noch keine Bewertungen
- Draping of Tibia: Sandwich TechniqueDokument3 SeitenDraping of Tibia: Sandwich Techniquebagus lazuardiNoch keine Bewertungen
- 06 Inguinal Hernia SrsDokument10 Seiten06 Inguinal Hernia SrslowhillNoch keine Bewertungen
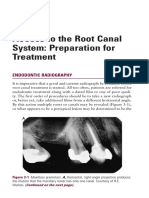
- Access To The Root Canal System: Preparation For Treatment: Endodontic RadiographyDokument13 SeitenAccess To The Root Canal System: Preparation For Treatment: Endodontic RadiographyMonika LohakpureNoch keine Bewertungen
- 07 Palatal Expansion With The Nitanium Palatal ExpanderDokument12 Seiten07 Palatal Expansion With The Nitanium Palatal ExpanderIG Fraga100% (1)
- Ward Prep NotesDokument7 SeitenWard Prep NotesReese Alessandra GandulfoNoch keine Bewertungen
- Knee AtrosDokument9 SeitenKnee AtrosNyoman Gede BimantaraNoch keine Bewertungen
- Temporal Bone Dissection - Basic Surgery of The Temporal BoneDokument26 SeitenTemporal Bone Dissection - Basic Surgery of The Temporal BoneIvana MatejováNoch keine Bewertungen
- EpisiotomyDokument6 SeitenEpisiotomyNishaThakuri100% (1)
- v2 71080982 Reva Ilizarov Foot Ankle Mid Foot Deformity Surgical Technique 0420Dokument22 Seitenv2 71080982 Reva Ilizarov Foot Ankle Mid Foot Deformity Surgical Technique 0420Charlie KorbaNoch keine Bewertungen
- Principles of Minimal Invasive Surgery: AnesthesiaDokument46 SeitenPrinciples of Minimal Invasive Surgery: AnesthesiaGladys SusantyNoch keine Bewertungen
- Zingaretti Et Al. 2019Dokument5 SeitenZingaretti Et Al. 2019Walid SasiNoch keine Bewertungen
- UntitledDokument19 SeitenUntitledChirashreeNoch keine Bewertungen
- AppendectomyDokument6 SeitenAppendectomyMarie Nelle Escriba LimpocoNoch keine Bewertungen
- Short Reconstruction NailDokument14 SeitenShort Reconstruction NailSimona DraganNoch keine Bewertungen
- CTF 10 Light Tower: Standard Control PanelDokument2 SeitenCTF 10 Light Tower: Standard Control PanelralphholingsheadNoch keine Bewertungen
- Ex Proof LampDokument2 SeitenEx Proof LampralphholingsheadNoch keine Bewertungen
- CTF 10 Light Tower: Standard Control PanelDokument2 SeitenCTF 10 Light Tower: Standard Control PanelralphholingsheadNoch keine Bewertungen
- AVR DECS200 Instalation and CommissioningDokument1 SeiteAVR DECS200 Instalation and CommissioningralphholingsheadNoch keine Bewertungen
- DECS200 200NComparison PDFDokument1 SeiteDECS200 200NComparison PDFralphholingsheadNoch keine Bewertungen
- Petrel 7-Series FCDokument2 SeitenPetrel 7-Series FCralphholingsheadNoch keine Bewertungen
- 200 TON ManualDokument4 Seiten200 TON ManualralphholingsheadNoch keine Bewertungen
- Generator Unit CircuitDokument1 SeiteGenerator Unit CircuitralphholingsheadNoch keine Bewertungen
- Ideco Vehicle Drive in Rambler 7005Dokument129 SeitenIdeco Vehicle Drive in Rambler 7005ralphholingsheadNoch keine Bewertungen
- Appendix: Approvals Partner at Industry Automation and Drive Technologies Online ServicesDokument20 SeitenAppendix: Approvals Partner at Industry Automation and Drive Technologies Online ServicesralphholingsheadNoch keine Bewertungen
- Elektronika-Tesco-06 - Tranzistori BJT PDFDokument15 SeitenElektronika-Tesco-06 - Tranzistori BJT PDFralphholingsheadNoch keine Bewertungen
- UG Governor: ApplicationsDokument4 SeitenUG Governor: ApplicationsralphholingsheadNoch keine Bewertungen
- UG-5.7, 8, and 10 Lever Governor: Product Manual 03036 (Revision L, 12/2014)Dokument58 SeitenUG-5.7, 8, and 10 Lever Governor: Product Manual 03036 (Revision L, 12/2014)ralphholingsheadNoch keine Bewertungen
- ISC Female PDFDokument4 SeitenISC Female PDFralphholingsheadNoch keine Bewertungen
- Judges Kings ProphetsDokument60 SeitenJudges Kings ProphetsKim John BolardeNoch keine Bewertungen
- Komatsu Hydraulic Excavator Pc290lc 290nlc 6k Shop ManualDokument20 SeitenKomatsu Hydraulic Excavator Pc290lc 290nlc 6k Shop Manualmallory100% (47)
- The Problem Between Teacher and Students: Name: Dinda Chintya Sinaga (2152121008) Astry Iswara Kelana Citra (2152121005)Dokument3 SeitenThe Problem Between Teacher and Students: Name: Dinda Chintya Sinaga (2152121008) Astry Iswara Kelana Citra (2152121005)Astry Iswara Kelana CitraNoch keine Bewertungen
- A Comparison of Practitioner and Student WritingDokument28 SeitenA Comparison of Practitioner and Student WritingMichael Sniper WuNoch keine Bewertungen
- What A Wonderful WorldDokument2 SeitenWhat A Wonderful WorldDraganaNoch keine Bewertungen
- PDF - Unpacking LRC and LIC Calculations For PC InsurersDokument14 SeitenPDF - Unpacking LRC and LIC Calculations For PC Insurersnod32_1206Noch keine Bewertungen
- HSE Induction Training 1687407986Dokument59 SeitenHSE Induction Training 1687407986vishnuvarthanNoch keine Bewertungen
- Sugar Industries of PakistanDokument19 SeitenSugar Industries of Pakistanhelperforeu50% (2)
- PH Water On Stability PesticidesDokument6 SeitenPH Water On Stability PesticidesMontoya AlidNoch keine Bewertungen
- Sycip v. CA (Sufficient Funds With The Drawee Bank)Dokument15 SeitenSycip v. CA (Sufficient Funds With The Drawee Bank)Arnold BagalanteNoch keine Bewertungen
- Why Nations Fail - SummaryDokument3 SeitenWhy Nations Fail - SummarysaraNoch keine Bewertungen
- Baixar Livro Draw With Jazza Creating Characters de Josiah Broo PDFDokument5 SeitenBaixar Livro Draw With Jazza Creating Characters de Josiah Broo PDFCarlos Mendoza25% (4)
- Module 5amp6 Cheerdance PDF FreeDokument27 SeitenModule 5amp6 Cheerdance PDF FreeKatNoch keine Bewertungen
- Corelation & Multiple Regression AnalysisDokument28 SeitenCorelation & Multiple Regression AnalysisSaad Bin Tariq100% (1)
- Hirarc Form: 1. Hazard Identification 2. Risk Analysis 3. Risk ControlDokument2 SeitenHirarc Form: 1. Hazard Identification 2. Risk Analysis 3. Risk ControlQurratulain Syarifuddinzaini100% (1)
- dm00226326 Using The Hardware Realtime Clock RTC and The Tamper Management Unit Tamp With stm32 MicrocontrollersDokument82 Seitendm00226326 Using The Hardware Realtime Clock RTC and The Tamper Management Unit Tamp With stm32 MicrocontrollersMoutaz KhaterNoch keine Bewertungen
- WIKADokument10 SeitenWIKAPatnubay B TiamsonNoch keine Bewertungen
- Kerjaya JuruterbangDokument11 SeitenKerjaya JuruterbangAqil NazriNoch keine Bewertungen
- Alankit Assignments LTD.: Project Report ONDokument84 SeitenAlankit Assignments LTD.: Project Report ONmannuNoch keine Bewertungen
- IN THE BEGINNING WAS AFFECT RolnikDokument22 SeitenIN THE BEGINNING WAS AFFECT RolnikFabiana PaulinoNoch keine Bewertungen
- Answer The Statements Below by Boxing The Past Perfect TenseDokument1 SeiteAnswer The Statements Below by Boxing The Past Perfect TenseMa. Myla PoliquitNoch keine Bewertungen
- ZultaniteDokument4 SeitenZultaniteAcharya BalwantNoch keine Bewertungen
- Boylestad Circan 3ce Ch02Dokument18 SeitenBoylestad Circan 3ce Ch02sherry mughalNoch keine Bewertungen
- Surge Protectionfor ACMachineryDokument8 SeitenSurge Protectionfor ACMachineryvyroreiNoch keine Bewertungen
- New Count The DotsDokument1 SeiteNew Count The Dotslin ee100% (1)
- Part A Questions and AnswersDokument10 SeitenPart A Questions and Answerssriparans356Noch keine Bewertungen
- E F Eng l1 l2 Si 011Dokument2 SeitenE F Eng l1 l2 Si 011Simona ButeNoch keine Bewertungen
- Student Management System - Full DocumentDokument46 SeitenStudent Management System - Full DocumentI NoNoch keine Bewertungen
- Adrenal Cortical TumorsDokument8 SeitenAdrenal Cortical TumorsSabrina whtNoch keine Bewertungen
- Rotation and Revolution of EarthDokument4 SeitenRotation and Revolution of EarthRamu ArunachalamNoch keine Bewertungen