Das könnte Ihnen auch gefallen
- Topical Steroids DermatologyDokument23 SeitenTopical Steroids DermatologyRitika Agarwal100% (1)
- Herbal Property Dictionary SampleDokument27 SeitenHerbal Property Dictionary Sampledarkllight100% (3)
- Common Pediatric Cases in OpdDokument90 SeitenCommon Pediatric Cases in OpdJamie Sebastian100% (3)
- Philippine Cancer Control Program.1.1Dokument8 SeitenPhilippine Cancer Control Program.1.1Ruby Joy EspirituNoch keine Bewertungen
- Anesth BarashDokument6 SeitenAnesth BarashIAN GABRIELLE MERCADO CUYNONoch keine Bewertungen
- Therapeutic Dosages For PEDIADokument7 SeitenTherapeutic Dosages For PEDIAPatrick PalaypayonNoch keine Bewertungen
- Clincal Practice Guidelines For Diabetes in The PhilippinesDokument40 SeitenClincal Practice Guidelines For Diabetes in The PhilippinesRans NosceNoch keine Bewertungen
- CDX 1 FinalDokument74 SeitenCDX 1 FinalGabby Elardo100% (1)
- Quaalude PDFDokument8 SeitenQuaalude PDFtom100% (1)
- Common Cases in Ambulatory Care Clinic For Lu6Dokument106 SeitenCommon Cases in Ambulatory Care Clinic For Lu6Joy SantosNoch keine Bewertungen
- Philippine Clinical Practice Guidelines UTIDokument95 SeitenPhilippine Clinical Practice Guidelines UTIToy Gallo100% (2)
- Vol 26.4 - Sleep Neurology.2020Dokument299 SeitenVol 26.4 - Sleep Neurology.2020Mardika FamilyNoch keine Bewertungen
- Nip Mop Booklet 1 8Dokument256 SeitenNip Mop Booklet 1 8camaso.noemiNoch keine Bewertungen
- Pedia Notes Print2Dokument5 SeitenPedia Notes Print2John Christopher LucesNoch keine Bewertungen
- Pedia TicklerDokument55 SeitenPedia TicklerMa Louize Magbanua100% (1)
- Mccod SGDDokument2 SeitenMccod SGDKYLE ANGELA PE�ARROYONoch keine Bewertungen
- Jurisprudence and EthicsDokument22 SeitenJurisprudence and EthicsRozamae Magnanao100% (1)
- Doctor's OrderDokument4 SeitenDoctor's OrderKinahZildredBibitNoch keine Bewertungen
- Pedia Idiot Notes 1Dokument12 SeitenPedia Idiot Notes 1David JonesNoch keine Bewertungen
- Standard Operating Procedures HospitalDokument5 SeitenStandard Operating Procedures HospitalCindy Gabayeron100% (1)
- Bioidentical Hormone TherapyDokument8 SeitenBioidentical Hormone TherapyKorry Meliana PangaribuanNoch keine Bewertungen
- PartographDokument6 SeitenPartographYep Yep100% (2)
- 10ADR & Reporting Methods - RutuDokument44 Seiten10ADR & Reporting Methods - RutuSejal khumanNoch keine Bewertungen
- ESSENTIAL DRUGS in The PhilippinesDokument58 SeitenESSENTIAL DRUGS in The Philippinesjquin3100% (1)
- Project Management Report On PharamaceuticalDokument15 SeitenProject Management Report On PharamaceuticalHamza AhmadNoch keine Bewertungen
- Er Admission PolicyDokument9 SeitenEr Admission PolicyIrish Martinez100% (2)
- Module 3: Hospital Pharmacy: Prepared By: Alexandra D. Atienza RPHDokument135 SeitenModule 3: Hospital Pharmacy: Prepared By: Alexandra D. Atienza RPHJojo DelosreyesNoch keine Bewertungen
- F U N W I S E: Know Your Symptom Severity Score!Dokument2 SeitenF U N W I S E: Know Your Symptom Severity Score!Jamie Sebastian50% (2)
- Surface TensionDokument50 SeitenSurface TensionbagheldhirendraNoch keine Bewertungen
- Worksheet Exercise 3 Prescription 1Dokument10 SeitenWorksheet Exercise 3 Prescription 1Guiller ReyesNoch keine Bewertungen
- MCCOD NotesDokument41 SeitenMCCOD NotesIvana Biado100% (1)
- Consensus Guidelines On Point of Care Testing in Hospitals: I. BackgroundDokument4 SeitenConsensus Guidelines On Point of Care Testing in Hospitals: I. BackgroundDocAxi Maximo Jr Axibal100% (2)
- National Tuberculosis Control Program Manual of Procedures 5th EditionDokument192 SeitenNational Tuberculosis Control Program Manual of Procedures 5th EditionBlue Pielago100% (9)
- Common RHU DrugsDokument56 SeitenCommon RHU DrugsAlna Shelah IbañezNoch keine Bewertungen
- Addition and DeletionDokument10 SeitenAddition and DeletionNikkaMontilNoch keine Bewertungen
- Fundamentals of Nursing Bullets (Nle & Nclex)Dokument32 SeitenFundamentals of Nursing Bullets (Nle & Nclex)ulcNoch keine Bewertungen
- Clinical Practice Guidelines - Acute AppendicitisDokument3 SeitenClinical Practice Guidelines - Acute AppendicitisJamie Sebastian75% (4)
- Notes by Dr. Khurram PDFDokument22 SeitenNotes by Dr. Khurram PDFAdnan AsgharNoch keine Bewertungen
- Appendix C2 Cover Letter ASUBARDokument2 SeitenAppendix C2 Cover Letter ASUBARRuel Vincent AsubarNoch keine Bewertungen
- Republic Act No 6675Dokument4 SeitenRepublic Act No 6675JenilynM.ChuNoch keine Bewertungen
- Patient Medication ProfileDokument4 SeitenPatient Medication ProfileLaura HernandezNoch keine Bewertungen
- Ppgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityDokument5 SeitenPpgp-Mfg-Oc G3 - Pd-2 - CP, CPP, Cqa NOTES On The ActivityIsabel Peralta50% (2)
- Chapter 9.odtDokument31 SeitenChapter 9.odtsteamierNoch keine Bewertungen
- Drug Storage Room StandardsDokument4 SeitenDrug Storage Room StandardsAhmad Al SaddikNoch keine Bewertungen
- Chronic Suppurative Otitis Media in AdultsDokument10 SeitenChronic Suppurative Otitis Media in AdultsRstadam TagalogNoch keine Bewertungen
- Oath of A Pharmacy StudentDokument1 SeiteOath of A Pharmacy StudentJane100% (1)
- Poison InformationDokument29 SeitenPoison InformationPooja agarwalNoch keine Bewertungen
- 57 74Dokument5 Seiten57 74Lisa Puspadewi SusantoNoch keine Bewertungen
- Pro TaminaDokument2 SeitenPro TaminaArcenciel26Noch keine Bewertungen
- The Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgeDokument4 SeitenThe Hydrocephalus Foundation of The Philippines, Inc.: Save A Life, I PledgejomitraNoch keine Bewertungen
- Pocket-Pedia PDFDokument9 SeitenPocket-Pedia PDFKatrin Miñas MendozaNoch keine Bewertungen
- DOH National TB Control Program - PhilippinesDokument5 SeitenDOH National TB Control Program - PhilippinesJuan Miguel PangilinanNoch keine Bewertungen
- Organization Introduction and Background: Target CustomersDokument5 SeitenOrganization Introduction and Background: Target CustomersArthur GitauNoch keine Bewertungen
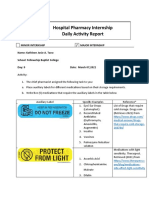
- Nica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 9 Major RevDokument2 SeitenNica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 9 Major RevMa Victoria ChuaNoch keine Bewertungen
- Orientation To The IVT ProgramDokument16 SeitenOrientation To The IVT ProgramCrystal Mae Castrodes DaquipilNoch keine Bewertungen
- Leopando Hospice-Palliative3Dokument2 SeitenLeopando Hospice-Palliative3Judy Ignacio EclarinoNoch keine Bewertungen
- Activities For Community PharmacyDokument12 SeitenActivities For Community Pharmacycjh1015960% (1)
- Stroke and HypertensionDokument4 SeitenStroke and HypertensionKhessie Laye Garcia JacintoNoch keine Bewertungen
- Microbio PDFDokument17 SeitenMicrobio PDFHernandez IanNoch keine Bewertungen
- Ali Medicos Pharmacy Standard Operating Procedures (Sops)Dokument4 SeitenAli Medicos Pharmacy Standard Operating Procedures (Sops)Amir ZakiNoch keine Bewertungen
- REC Form 3.3 Closure or Final Report FormDokument5 SeitenREC Form 3.3 Closure or Final Report FormJunjun Tupas100% (1)
- Bioavailability PK Practice Problems 2013Dokument2 SeitenBioavailability PK Practice Problems 2013Linh PhamNoch keine Bewertungen
- 6.1 Ra 9502 PDFDokument124 Seiten6.1 Ra 9502 PDFMhae Ü Samonte100% (1)
- Individual Prescription Order SystemDokument19 SeitenIndividual Prescription Order SystemShikitoka BatiancilaNoch keine Bewertungen
- Ra 7600 PDFDokument5 SeitenRa 7600 PDFanorith88Noch keine Bewertungen
- 2016 Cap by PsmidDokument26 Seiten2016 Cap by PsmidRay Emmanuel Enriquez DomingoNoch keine Bewertungen
- 2016 Cap by PsmidDokument26 Seiten2016 Cap by PsmidBaeyonce MDNoch keine Bewertungen
- Reviews: Proton-Pump Inhibitors: Understanding The Complications and RisksDokument14 SeitenReviews: Proton-Pump Inhibitors: Understanding The Complications and RisksRONALD. D VIERA .MNoch keine Bewertungen
- GuidelineDokument69 SeitenGuidelineDannah TagulaoNoch keine Bewertungen
- Lechien Saussez Karkos Curr Opin 2018Dokument12 SeitenLechien Saussez Karkos Curr Opin 2018alivanabilafarinisaNoch keine Bewertungen
- Feno Asma y Epoc Ers 2019Dokument11 SeitenFeno Asma y Epoc Ers 2019Estefania Yu AcevedoNoch keine Bewertungen
- New Perio ClassificationDokument8 SeitenNew Perio ClassificationLauraNoch keine Bewertungen
- Gerd CPG PDFDokument17 SeitenGerd CPG PDFJamie SebastianNoch keine Bewertungen
- Emailing CPG-E PDFDokument206 SeitenEmailing CPG-E PDFCarlos H. AcuñaNoch keine Bewertungen
- MOT PatentsDokument14 SeitenMOT PatentsAnonymous AWcEiTj5u0Noch keine Bewertungen
- Anti Anginal DrugsDokument1 SeiteAnti Anginal DrugsHatem AbouelnasrNoch keine Bewertungen
- CASE STUDY CHAPTER 3 Business EthicsDokument5 SeitenCASE STUDY CHAPTER 3 Business EthicsHeidy JosephineNoch keine Bewertungen
- Natco 2016 PDFDokument101 SeitenNatco 2016 PDFSagar BhardwajNoch keine Bewertungen
- Efficacy of Salbutamol-Ipratropium Bromide Nebulization Compared To SalbutamolDokument16 SeitenEfficacy of Salbutamol-Ipratropium Bromide Nebulization Compared To Salbutamolclear_safNoch keine Bewertungen
- Controlled Substances ListDokument23 SeitenControlled Substances ListJeremy MontgomeryNoch keine Bewertungen
- VoltarenTab PDFDokument6 SeitenVoltarenTab PDFhmarcalNoch keine Bewertungen
- Rahul Krishna Pandharpatte-3Dokument3 SeitenRahul Krishna Pandharpatte-3Vidhya ChuriNoch keine Bewertungen
- KXDokument28 SeitenKXGatwech Dech RutNoch keine Bewertungen
- Helicobacter Pylori - The Latest in Diagnosis and TreatmentDokument5 SeitenHelicobacter Pylori - The Latest in Diagnosis and TreatmentekramsNoch keine Bewertungen
- 6Dokument11 Seiten6UgaugaaNoch keine Bewertungen
- Routine For 8th Sem 2017Dokument5 SeitenRoutine For 8th Sem 2017Tanbir MukherjeeNoch keine Bewertungen
- Quality Risk Management Ich Q9Dokument57 SeitenQuality Risk Management Ich Q9prakash deshmukhNoch keine Bewertungen
- Formulation and Evaluation of Cefadroxil Mucoadhesive TabletsDokument18 SeitenFormulation and Evaluation of Cefadroxil Mucoadhesive TabletsBaru Chandrasekhar RaoNoch keine Bewertungen
- Ghana Market OverviewDokument27 SeitenGhana Market OverviewAshish PandeyNoch keine Bewertungen
- TABLE 56-4 - Neurological Side Effects of Antipsychotic DrugsDokument1 SeiteTABLE 56-4 - Neurological Side Effects of Antipsychotic DrugsDragutin PetrićNoch keine Bewertungen
- Colistin and Polymyxin BDokument6 SeitenColistin and Polymyxin BJia KhanNoch keine Bewertungen
- Session 10 KaddarDokument38 SeitenSession 10 KaddarsuybaNoch keine Bewertungen
- HBBBNDokument50 SeitenHBBBNHayyina FirdaniNoch keine Bewertungen
- Unit4 ADokument2 SeitenUnit4 AsaraNoch keine Bewertungen
- Alkan Health Science Business and Technology CollegeDokument62 SeitenAlkan Health Science Business and Technology CollegejibrNoch keine Bewertungen