Das könnte Ihnen auch gefallen
- Marijuana Policy Progress Report 2019 Legislative UpdateDokument28 SeitenMarijuana Policy Progress Report 2019 Legislative UpdateMPP100% (3)
- Med Cannabis Stock SecurityDokument12 SeitenMed Cannabis Stock SecurityTrelospapasse BaftisedenyparxeisNoch keine Bewertungen
- SmartSafeFlorida AdultCannabisMeasureDokument4 SeitenSmartSafeFlorida AdultCannabisMeasureTony LangeNoch keine Bewertungen
- Petition Urging Governors To Protect Medical Cannabis AccessDokument70 SeitenPetition Urging Governors To Protect Medical Cannabis AccessMPPNoch keine Bewertungen
- Cannabis Cannabinoids and HealthDokument9 SeitenCannabis Cannabinoids and HealthCathy JenkinsNoch keine Bewertungen
- Severe Pain and Medical CannabisDokument1 SeiteSevere Pain and Medical CannabisMPPNoch keine Bewertungen
- Severe Pain and Medical CannabisDokument1 SeiteSevere Pain and Medical CannabisMPPNoch keine Bewertungen
- The Philippine Army Doctrine DevelopmentDokument10 SeitenThe Philippine Army Doctrine DevelopmentRy PomarNoch keine Bewertungen
- 15Dokument74 Seiten15physicsdocs60% (25)
- Cannabis Class Action Lawsuit - UHDokument2 SeitenCannabis Class Action Lawsuit - UHTony Lange100% (1)
- Linux OS MyanmarDokument75 SeitenLinux OS Myanmarweenyin100% (15)
- Ashforth & Mael 1989 Social Identity Theory and The OrganizationDokument21 SeitenAshforth & Mael 1989 Social Identity Theory and The Organizationhoorie100% (1)
- A Snapshot of Demand For Adult-Use Cannabis in IllinoisDokument27 SeitenA Snapshot of Demand For Adult-Use Cannabis in IllinoisTodd FeurerNoch keine Bewertungen
- Overview of Maryland's Medical Marijuana LawDokument3 SeitenOverview of Maryland's Medical Marijuana LawMPP100% (1)
- Economics of Cannabis LegalizationDokument12 SeitenEconomics of Cannabis LegalizationMPPNoch keine Bewertungen
- The History of Cannabis Regulation in Shasta County 10.11.14Dokument7 SeitenThe History of Cannabis Regulation in Shasta County 10.11.14MatthewMeyerNoch keine Bewertungen
- Cannabis in The ClinicDokument3 SeitenCannabis in The ClinicVianne ArcenioNoch keine Bewertungen
- UPA Cannabis Stories LeafletDokument2 SeitenUPA Cannabis Stories LeafletUnited Patients AllianceNoch keine Bewertungen
- Brett Painter Tech Writing SlideshowDokument17 SeitenBrett Painter Tech Writing SlideshowBrett PainterNoch keine Bewertungen
- Politics V Science Understanding Cannabis Therapeutics Before It Gets CensoredDokument3 SeitenPolitics V Science Understanding Cannabis Therapeutics Before It Gets Censoredjamie_clark_2Noch keine Bewertungen
- Oklahoma's Low-THC LawDokument1 SeiteOklahoma's Low-THC LawMPPNoch keine Bewertungen
- 7 31 2014 - CannabisFinalReport PDFDokument23 Seiten7 31 2014 - CannabisFinalReport PDFlighthouseventureNoch keine Bewertungen
- Regulating Cannabis in NunavutDokument10 SeitenRegulating Cannabis in NunavutNunatsiaqNewsNoch keine Bewertungen
- The Propagation, Characterisation and Optimisation of Cannabis Sativa L As A PhytopharmaceuticalDokument255 SeitenThe Propagation, Characterisation and Optimisation of Cannabis Sativa L As A PhytopharmaceuticalUPMMJNoch keine Bewertungen
- Joint Conversations Newsletter - January 2015Dokument16 SeitenJoint Conversations Newsletter - January 2015Casper LeitchNoch keine Bewertungen
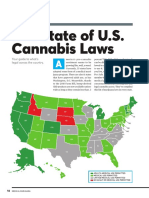
- The State of U.S. Cannabis Laws, AbridgedDokument6 SeitenThe State of U.S. Cannabis Laws, AbridgedPaul Marini100% (1)
- Iowa's Low-THC Law SummaryDokument1 SeiteIowa's Low-THC Law SummaryMPPNoch keine Bewertungen
- Regulatory Authorities and Medical CannabisDokument3 SeitenRegulatory Authorities and Medical CannabisMPPNoch keine Bewertungen
- Chardan Capital On Cannabis MarketDokument8 SeitenChardan Capital On Cannabis MarketotteromNoch keine Bewertungen
- Model State Adult-Use Legalization and Regulation BillDokument22 SeitenModel State Adult-Use Legalization and Regulation BillMPPNoch keine Bewertungen
- Model Tax and Regulate Bill SummaryDokument2 SeitenModel Tax and Regulate Bill SummaryMPPNoch keine Bewertungen
- Cannabis Use and Substantial Reduction in Premature Deaths in The United States.Dokument53 SeitenCannabis Use and Substantial Reduction in Premature Deaths in The United States.Monterey Bud100% (2)
- Joint Conversations Newsletter - January 2016Dokument20 SeitenJoint Conversations Newsletter - January 2016Casper LeitchNoch keine Bewertungen
- 2018 Model LegislationDokument18 Seiten2018 Model LegislationPaul MariniNoch keine Bewertungen
- Regulation WorksDokument1 SeiteRegulation WorksMPPNoch keine Bewertungen
- 2011 - La Globalización Del Cultivo Casero de Cannabis - Potter y ColDokument21 Seiten2011 - La Globalización Del Cultivo Casero de Cannabis - Potter y Colzxs17zNoch keine Bewertungen
- Argument Essay FinaleDokument4 SeitenArgument Essay Finaleapi-458895222Noch keine Bewertungen
- Revenue From Adult Use StatesDokument5 SeitenRevenue From Adult Use StatesMPPNoch keine Bewertungen
- Progress Report New York Medical Marijuana ProgramDokument2 SeitenProgress Report New York Medical Marijuana ProgramMPPNoch keine Bewertungen
- State Decrim ChartDokument4 SeitenState Decrim ChartMPPNoch keine Bewertungen
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDokument1 SeiteSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNoch keine Bewertungen
- Tax and Regulate BrochureDokument2 SeitenTax and Regulate BrochureMPPNoch keine Bewertungen
- When Cannabis Goes CorporateDokument9 SeitenWhen Cannabis Goes CorporateLes CanoNoch keine Bewertungen
- Michigan's Medical Marihuana ActDokument27 SeitenMichigan's Medical Marihuana Actapi-25946258Noch keine Bewertungen
- Marijuana Research PaperDokument12 SeitenMarijuana Research PaperTianna100% (1)
- Exposing The 'Reefer Madness' of The Parliament of Canada 11of10 ConclusionsDokument14 SeitenExposing The 'Reefer Madness' of The Parliament of Canada 11of10 ConclusionsSam VekemansNoch keine Bewertungen
- State-by-State Provisions For Adding Qualifying ConditionsDokument5 SeitenState-by-State Provisions For Adding Qualifying ConditionsMPPNoch keine Bewertungen
- Changing Landscape of Cannabis Novel Products Formulations and Methods of Administration PDFDokument5 SeitenChanging Landscape of Cannabis Novel Products Formulations and Methods of Administration PDFliaNoch keine Bewertungen
- Pennsylvania Report On Adult Use Recreational MarijuanaDokument89 SeitenPennsylvania Report On Adult Use Recreational MarijuanaMarijuana MomentNoch keine Bewertungen
- Chemical Basis For Increased Potency Related To Novel Method of PreparationDokument3 SeitenChemical Basis For Increased Potency Related To Novel Method of Preparationbagusu_6Noch keine Bewertungen
- Marijuana Research PaperDokument11 SeitenMarijuana Research PaperJack DohertyNoch keine Bewertungen
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDokument7 SeitenMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNoch keine Bewertungen
- Need For Standardization of Cannabis Sativa L. (Hemp, Medical Marijuana and Marijuana As A Drug) in SloveniaDokument18 SeitenNeed For Standardization of Cannabis Sativa L. (Hemp, Medical Marijuana and Marijuana As A Drug) in SloveniaTomaz KorenNoch keine Bewertungen
- Medical Marijuana Laws and Public SafetyDokument3 SeitenMedical Marijuana Laws and Public SafetyMPPNoch keine Bewertungen
- Legal Opinion Letter CBD Sold Nationwide Final August 21, 2018Dokument33 SeitenLegal Opinion Letter CBD Sold Nationwide Final August 21, 2018Robert KossackNoch keine Bewertungen
- Cannabis For Restless Legs SyndromeDokument1 SeiteCannabis For Restless Legs SyndromeGi GlerNoch keine Bewertungen
- Market Structure For Recreational Cannabis PROACTIVE FINALDokument57 SeitenMarket Structure For Recreational Cannabis PROACTIVE FINALda5idnzNoch keine Bewertungen
- Breakdown of Fees in Adult-Use StatesDokument6 SeitenBreakdown of Fees in Adult-Use StatesMPPNoch keine Bewertungen
- Cannabis Use Disorder Identification TestDokument1 SeiteCannabis Use Disorder Identification TestMichael_Lee_RobertsNoch keine Bewertungen
- MarijuanaDokument8 SeitenMarijuanajohnkyleNoch keine Bewertungen
- Phytochemical Screening of Cannabis IndicaDokument7 SeitenPhytochemical Screening of Cannabis IndicaafridiNoch keine Bewertungen
- Colorado and Washington: Life After Legalization and RegulationDokument2 SeitenColorado and Washington: Life After Legalization and RegulationMPP100% (3)
- Cannabis Psychosis Fact Sheet PDFDokument1 SeiteCannabis Psychosis Fact Sheet PDFricardo_balau8081Noch keine Bewertungen
- Federal Obstruction of Medical Marijuana ResearchDokument2 SeitenFederal Obstruction of Medical Marijuana ResearchMPPNoch keine Bewertungen
- GQR Connecticut Poll January 2020Dokument1 SeiteGQR Connecticut Poll January 2020MPPNoch keine Bewertungen
- 2018 SIU Paul Simon Public Policy Institute Legalization PollDokument4 Seiten2018 SIU Paul Simon Public Policy Institute Legalization PollMPPNoch keine Bewertungen
- 2020 Vermont Poll ResultsDokument7 Seiten2020 Vermont Poll ResultsMPPNoch keine Bewertungen
- U.S. Attorneys' Comments Post Cole Memo RecissionDokument8 SeitenU.S. Attorneys' Comments Post Cole Memo RecissionMPPNoch keine Bewertungen
- Medical Cannabis Provides An Alternative To OpiatesDokument1 SeiteMedical Cannabis Provides An Alternative To OpiatesMPPNoch keine Bewertungen
- MPP Policy Paper - Regulating Cannabis Oil VaporizersDokument7 SeitenMPP Policy Paper - Regulating Cannabis Oil VaporizersMPPNoch keine Bewertungen
- Marijuana Policy Map May 2020Dokument1 SeiteMarijuana Policy Map May 2020MPPNoch keine Bewertungen
- Simon Poll March 2019Dokument14 SeitenSimon Poll March 2019MPPNoch keine Bewertungen
- What Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?Dokument2 SeitenWhat Does Former AG Sessions' Marijuana Enforcement Memo Mean in Practice?MPPNoch keine Bewertungen
- Decriminalization and Expungement in NY: An Overview of A0840 / S06579Dokument1 SeiteDecriminalization and Expungement in NY: An Overview of A0840 / S06579MPPNoch keine Bewertungen
- Medical Cannabis Implementation TimelinesDokument10 SeitenMedical Cannabis Implementation TimelinesMPPNoch keine Bewertungen
- Medical Marijuana MapDokument1 SeiteMedical Marijuana MapMPPNoch keine Bewertungen
- 2017 SIU Paul Simon Public Policy Institute Legalization PollDokument7 Seiten2017 SIU Paul Simon Public Policy Institute Legalization PollMPPNoch keine Bewertungen
- D.C.'s Medical Marijuana ProgramDokument2 SeitenD.C.'s Medical Marijuana ProgramMPPNoch keine Bewertungen
- Progress Report New York Medical Marijuana ProgramDokument2 SeitenProgress Report New York Medical Marijuana ProgramMPPNoch keine Bewertungen
- Maryland Progress ReportDokument2 SeitenMaryland Progress ReportMPPNoch keine Bewertungen
- Medical Marijuana by The NumbersDokument2 SeitenMedical Marijuana by The NumbersMPPNoch keine Bewertungen
- Potential Revenue From Regulating Marijuana in ConnecticutDokument2 SeitenPotential Revenue From Regulating Marijuana in ConnecticutMPPNoch keine Bewertungen
- New Jersey Progress ReportDokument2 SeitenNew Jersey Progress ReportMPPNoch keine Bewertungen
- Expungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionDokument1 SeiteExpungement: Removing The Life-Long Stigma Caused by Marijuana ProhibitionMPPNoch keine Bewertungen
- Breakdown of Fees in Adult-Use StatesDokument6 SeitenBreakdown of Fees in Adult-Use StatesMPPNoch keine Bewertungen
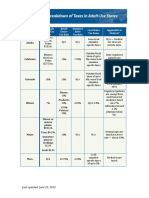
- Breakdown of Taxes in Adult-Use StatesDokument2 SeitenBreakdown of Taxes in Adult-Use StatesMPPNoch keine Bewertungen
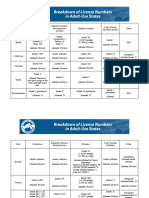
- Breakdown of License Numbers in Adult-Use StatesDokument2 SeitenBreakdown of License Numbers in Adult-Use StatesMPPNoch keine Bewertungen
- Sessions Asks Congress To Undo Medical Marijuana ProtectionsDokument3 SeitenSessions Asks Congress To Undo Medical Marijuana ProtectionsMPPNoch keine Bewertungen
- Revenue From Adult Use StatesDokument5 SeitenRevenue From Adult Use StatesMPPNoch keine Bewertungen
- Safe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicDokument1 SeiteSafe, Legal Access To Marijuana Can Help Fight The Opioid EpidemicMPPNoch keine Bewertungen
- Importance of SimilesDokument10 SeitenImportance of Similesnabeelajaved0% (1)
- Republic v. EncelanDokument2 SeitenRepublic v. EncelanKyla ReyesNoch keine Bewertungen
- CV Jan 2015 SDokument4 SeitenCV Jan 2015 Sapi-276142935Noch keine Bewertungen
- Indian Archaeology 1967 - 68 PDFDokument69 SeitenIndian Archaeology 1967 - 68 PDFATHMANATHANNoch keine Bewertungen
- Subarachnoid Cisterns & Cerebrospinal FluidDokument41 SeitenSubarachnoid Cisterns & Cerebrospinal Fluidharjoth395Noch keine Bewertungen
- My Testament On The Fabiana Arejola M...Dokument17 SeitenMy Testament On The Fabiana Arejola M...Jaime G. Arejola100% (1)
- Solutions To Basic Economic Problems - AllDokument27 SeitenSolutions To Basic Economic Problems - AllAsha GeorgeNoch keine Bewertungen
- Rak Single DentureDokument48 SeitenRak Single Denturerakes0Noch keine Bewertungen
- Jobgpt 9d48h0joDokument6 SeitenJobgpt 9d48h0jomaijel CancinesNoch keine Bewertungen
- Power of Positive Thinking EssayDokument7 SeitenPower of Positive Thinking Essayafiboeolrhismk100% (2)
- Electrostatics Formulas and Numerical ProblemsDokument11 SeitenElectrostatics Formulas and Numerical ProblemsManish kumar100% (2)
- Developing The Marketing Mix: Notre Dame of Jaro IncDokument3 SeitenDeveloping The Marketing Mix: Notre Dame of Jaro IncVia Terrado CañedaNoch keine Bewertungen
- Khin Thandar Myint EMPADokument101 SeitenKhin Thandar Myint EMPAAshin NandavamsaNoch keine Bewertungen
- Case Problems For Management ScienceDokument11 SeitenCase Problems For Management ScienceMargarita AtanacioNoch keine Bewertungen
- 01 Particle Sizing by Laser DifractionDokument145 Seiten01 Particle Sizing by Laser DifractionPramesvara NaoriNoch keine Bewertungen
- Listening LP1Dokument6 SeitenListening LP1Zee KimNoch keine Bewertungen
- LAWHIST - Week1 - Codamon Lim Tan PDFDokument32 SeitenLAWHIST - Week1 - Codamon Lim Tan PDFMargell TanNoch keine Bewertungen
- 2.1D Diy-Exercises (Questionnaires)Dokument31 Seiten2.1D Diy-Exercises (Questionnaires)Chinito Reel CasicasNoch keine Bewertungen
- Existentialism Is A HumanismDokument4 SeitenExistentialism Is A HumanismAlex MendezNoch keine Bewertungen
- Digoxin FABDokument6 SeitenDigoxin FABqwer22Noch keine Bewertungen
- Us Aers Roadmap Noncontrolling Interest 2019 PDFDokument194 SeitenUs Aers Roadmap Noncontrolling Interest 2019 PDFUlii PntNoch keine Bewertungen
- Aviation Case StudyDokument6 SeitenAviation Case Studynabil sayedNoch keine Bewertungen
- LP Moral Decision Making EditedDokument3 SeitenLP Moral Decision Making EditedCiana SacdalanNoch keine Bewertungen
- Needs and Language Goals of Students, Creating Learning Environments andDokument3 SeitenNeeds and Language Goals of Students, Creating Learning Environments andapi-316528766Noch keine Bewertungen
- Grecian Urn PaperDokument2 SeitenGrecian Urn PaperrhesajanubasNoch keine Bewertungen
- Lesson 6. TNCTDokument32 SeitenLesson 6. TNCTEsther EdaniolNoch keine Bewertungen