Das könnte Ihnen auch gefallen
- Blood Test Results - Your Guide To Understanding The Numbers NNHDokument21 SeitenBlood Test Results - Your Guide To Understanding The Numbers NNHSN Wijesinhe100% (2)
- Mineral DeficienciesDokument16 SeitenMineral DeficienciesDragan Pitic100% (4)
- Week 2 Case StudyDokument8 SeitenWeek 2 Case StudyMelissa Cerny100% (3)
- Understand LDL Cholesterol BetterDokument4 SeitenUnderstand LDL Cholesterol BetterhealthcheckupNoch keine Bewertungen
- NUTR LS1020 Fall Comprehensive Case Study-LeoJuneDokument8 SeitenNUTR LS1020 Fall Comprehensive Case Study-LeoJuneCollin Hiett0% (8)
- Biochem Midterm ReviewerDokument19 SeitenBiochem Midterm ReviewerERIKA ROSE ALEJONoch keine Bewertungen
- Fmed 08 697986Dokument14 SeitenFmed 08 697986sana siddiqueNoch keine Bewertungen
- Q10 Redução de FadigaDokument13 SeitenQ10 Redução de Fadigamatheuspatos1998Noch keine Bewertungen
- L-Carnitine Reduces Muscle Cramps in Patients With CirrhosisDokument18 SeitenL-Carnitine Reduces Muscle Cramps in Patients With CirrhosisthiagoNoch keine Bewertungen
- Complementary Therapies in Medicine: SciencedirectDokument11 SeitenComplementary Therapies in Medicine: SciencedirectNejc KovačNoch keine Bewertungen
- 2017 - Article - 65 2 PDFDokument11 Seiten2017 - Article - 65 2 PDFPaulina Sobarzo VegaNoch keine Bewertungen
- Mckenzie For LBP HNPDokument15 SeitenMckenzie For LBP HNPRiri NandaNoch keine Bewertungen
- CTTC Estatinas Lancet 2022Dokument14 SeitenCTTC Estatinas Lancet 2022Silvia Montejo FareloNoch keine Bewertungen
- 1 s2.0 S2347562521000627 MainDokument8 Seiten1 s2.0 S2347562521000627 MainUtami DewiNoch keine Bewertungen
- Effecrof Exerciseon NAFLDDokument1 SeiteEffecrof Exerciseon NAFLDjihanvrpNoch keine Bewertungen
- JFP 06309 Article1Dokument9 SeitenJFP 06309 Article1Fcm-srAafNoch keine Bewertungen
- Renal Dosing of Antibiotics Are We Jumping The GunDokument7 SeitenRenal Dosing of Antibiotics Are We Jumping The GunAnaNoch keine Bewertungen
- Medscimonit 20 1833Dokument8 SeitenMedscimonit 20 1833Snezana DjukicNoch keine Bewertungen
- WJG 20 2186Dokument8 SeitenWJG 20 2186RonjavafantillanNoch keine Bewertungen
- Efek Hepatoprotektif N-Asetilsistein Dalam Mencegah Drug-Induced Liver InjuDokument6 SeitenEfek Hepatoprotektif N-Asetilsistein Dalam Mencegah Drug-Induced Liver InjuAndry Wahyudi AgusNoch keine Bewertungen
- Pone 0159966Dokument16 SeitenPone 0159966JESICA PAOLA RODRIGUEZ PEREZNoch keine Bewertungen
- Nstemi and Stemi: Therapeutic Updates 2011: AuthorDokument9 SeitenNstemi and Stemi: Therapeutic Updates 2011: AuthorAfdol Triatmojo SikumbangNoch keine Bewertungen
- Kontras StatinDokument10 SeitenKontras Statinale_rhdNoch keine Bewertungen
- 1 s2.0 S144395061501269X Main4Dokument10 Seiten1 s2.0 S144395061501269X Main4maracioNoch keine Bewertungen
- 經皮穴位電刺激聯合下肢康復... 建術後康復中的應用效果分析 王薇Dokument6 Seiten經皮穴位電刺激聯合下肢康復... 建術後康復中的應用效果分析 王薇agneschan2003Noch keine Bewertungen
- Clinical Nutrition: Randomized Control TrialsDokument7 SeitenClinical Nutrition: Randomized Control TrialsBby AdelinaNoch keine Bewertungen
- 1 s2.0 S1871402123000747 MainDokument10 Seiten1 s2.0 S1871402123000747 MainGABRIEL NUNESNoch keine Bewertungen
- 1 s2.0 S2405844023078313 MainDokument14 Seiten1 s2.0 S2405844023078313 MainAsadm HosshNoch keine Bewertungen
- Acupuncture Methods For Functional Constipation: Protocol For A Systematic Review and Network Meta-AnalysisDokument10 SeitenAcupuncture Methods For Functional Constipation: Protocol For A Systematic Review and Network Meta-AnalysisMohmmad Hossein NazariNoch keine Bewertungen
- 2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain SyndromeDokument7 Seiten2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain Syndromeenfermeironilson6321Noch keine Bewertungen
- Medicine: Effect of Magnesium Sulfate On Renal Colic PainDokument8 SeitenMedicine: Effect of Magnesium Sulfate On Renal Colic PainJunaidy TahirNoch keine Bewertungen
- The Effect of Addition Kinesio Taping To Mckenzie Exercise in Patient With Chronic Mechanical Low Back PainDokument4 SeitenThe Effect of Addition Kinesio Taping To Mckenzie Exercise in Patient With Chronic Mechanical Low Back PainRama BayuNoch keine Bewertungen
- Manual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical TrialDokument7 SeitenManual Therapy in The Treatment of Carpal Tunnel Syndrome in Diabetic Patients: A Randomized Clinical TrialHerwanda PrasetyoNoch keine Bewertungen
- Effect of Statin Therapy On Muscle Symptoms Estudo CTTDokument14 SeitenEffect of Statin Therapy On Muscle Symptoms Estudo CTTjoseNoch keine Bewertungen
- Apnm 2014 0357Dokument8 SeitenApnm 2014 0357adri20121989Noch keine Bewertungen
- Fisioterapi JurnalDokument7 SeitenFisioterapi JurnalAchenk BarcelonistaNoch keine Bewertungen
- Effects of Resistance Exercise On Fatigue and Quality of Life in Breast Cancer Patients Undergoing Adjuvant Chemotherapy - A Randomized Controlled TrialDokument10 SeitenEffects of Resistance Exercise On Fatigue and Quality of Life in Breast Cancer Patients Undergoing Adjuvant Chemotherapy - A Randomized Controlled TrialPablo NahuelcoyNoch keine Bewertungen
- Journal Pre-Proof: Eres, JadrankaDokument25 SeitenJournal Pre-Proof: Eres, JadrankaDiana Magnavita MouraNoch keine Bewertungen
- Disminucion de Lípidos en Sindrome Coronario Agudo. Nicholls S 2018Dokument2 SeitenDisminucion de Lípidos en Sindrome Coronario Agudo. Nicholls S 2018Tony Miguel Saba SabaNoch keine Bewertungen
- Chow Wu Meyer - SC20 QOL FUNCTION - JCO 2014Dokument11 SeitenChow Wu Meyer - SC20 QOL FUNCTION - JCO 2014AmyNoch keine Bewertungen
- Art - LDokument10 SeitenArt - LCarlos TorresNoch keine Bewertungen
- Coenzyme Q10 As Treatment For Statin-Associated Muscle Symptoms-A Good Idea, ButDokument5 SeitenCoenzyme Q10 As Treatment For Statin-Associated Muscle Symptoms-A Good Idea, Butstarskyhutch0000Noch keine Bewertungen
- J Cachexia Sarcopenia Muscle - 2016 - Klassen - Muscle Strength in Breast Cancer Patients Receiving Different TreatmentDokument12 SeitenJ Cachexia Sarcopenia Muscle - 2016 - Klassen - Muscle Strength in Breast Cancer Patients Receiving Different TreatmentVukašin Schooly StojanovićNoch keine Bewertungen
- Base 16 de EjercicioDokument9 SeitenBase 16 de EjercicioAlejandra DiazNoch keine Bewertungen
- Acupuncture Therapy For Angina Pectoris: A Systematic ReviewDokument8 SeitenAcupuncture Therapy For Angina Pectoris: A Systematic ReviewYoNoch keine Bewertungen
- Jurnal YakinDokument11 SeitenJurnal Yakinmas setiawanNoch keine Bewertungen
- X. Young 2011 HepDokument11 SeitenX. Young 2011 HepJuan Carlos FloresNoch keine Bewertungen
- Fluids, Vasopressors and AKIDokument10 SeitenFluids, Vasopressors and AKIYasir Saleem KhanNoch keine Bewertungen
- 2 51 1624856559 Ijmpsdec20213Dokument10 Seiten2 51 1624856559 Ijmpsdec20213TJPRC PublicationsNoch keine Bewertungen
- Nonbacterial Prostatitis Treatment & Management: Approach ConsiderationsDokument3 SeitenNonbacterial Prostatitis Treatment & Management: Approach Considerationskhaje5Noch keine Bewertungen
- 2022 Article 456Dokument21 Seiten2022 Article 456Zu TranNoch keine Bewertungen
- Does Adding Hip Strengthening Exercises To ManualDokument8 SeitenDoes Adding Hip Strengthening Exercises To ManualBruno AssunçaoNoch keine Bewertungen
- Cheng-2021-Effect of Tai Chi and Resistance TRDokument8 SeitenCheng-2021-Effect of Tai Chi and Resistance TRFaizul HasanNoch keine Bewertungen
- Aerobic Interval Training Versus Continuous Moderate Exercise As A Treatment For The Metabolic SyndromeDokument10 SeitenAerobic Interval Training Versus Continuous Moderate Exercise As A Treatment For The Metabolic SyndromeSaulo MartinsNoch keine Bewertungen
- Respiratory Medicine: Kıymet Muammer, Fatma Mutluay, Rengin Demir, Alev Arat OzkanDokument10 SeitenRespiratory Medicine: Kıymet Muammer, Fatma Mutluay, Rengin Demir, Alev Arat OzkanMalik JamilNoch keine Bewertungen
- Annrheumdis 2016 210860.fullDokument8 SeitenAnnrheumdis 2016 210860.fullPatrick Leonard G. CoNoch keine Bewertungen
- Tgs TrdsionalDokument26 SeitenTgs TrdsionalrinirhynNoch keine Bewertungen
- Effects of Neuromuscular Electrical Stimulation in People With Spinal Cord InjuryDokument7 SeitenEffects of Neuromuscular Electrical Stimulation in People With Spinal Cord Injurynuttawat.runNoch keine Bewertungen
- Medscimonit 27 E931597Dokument7 SeitenMedscimonit 27 E931597kedelai pilihanNoch keine Bewertungen
- Jurnal Terapi ACE Inhibitors in Anthracycline Induced CardiotoxicityDokument6 SeitenJurnal Terapi ACE Inhibitors in Anthracycline Induced CardiotoxicityalerohmadNoch keine Bewertungen
- (European Heart Journal 2004) Beneficial Effects of Chronic Low-FrequencyDokument8 Seiten(European Heart Journal 2004) Beneficial Effects of Chronic Low-FrequencyRodolfo MatosNoch keine Bewertungen
- A Randomized Controlled Trial of Angiotensin-Converting Enzyme Inhibition For Skeletal Muscle Dysfunction in COPDDokument9 SeitenA Randomized Controlled Trial of Angiotensin-Converting Enzyme Inhibition For Skeletal Muscle Dysfunction in COPDᄋᄋNoch keine Bewertungen
- An Experimental Series Investigating The Effects of Hyperinsulinemic WuglycemiaDokument16 SeitenAn Experimental Series Investigating The Effects of Hyperinsulinemic WuglycemiaMarco Antonio Viera ArevaloNoch keine Bewertungen
- Cartlidge Timothy Role of Percutaneous CoronaryDokument7 SeitenCartlidge Timothy Role of Percutaneous Coronarybruno baileyNoch keine Bewertungen
- A Segurança e Eficácia Do Treinamento de Exercício de Iniciação Precoce Após Tromboembolismo Venoso Agudo Um Ensaio Clínico RandomizadoDokument7 SeitenA Segurança e Eficácia Do Treinamento de Exercício de Iniciação Precoce Após Tromboembolismo Venoso Agudo Um Ensaio Clínico RandomizadoSheilani MartinsNoch keine Bewertungen
- 3 Statins (Atorvastatin & Rosuvastatin)Dokument15 Seiten3 Statins (Atorvastatin & Rosuvastatin)Thet Su LwinNoch keine Bewertungen
- NDT Module 1Dokument97 SeitenNDT Module 1Fhei Lya Dee TioNoch keine Bewertungen
- Introduction To Data Analytics: Sampling DistributionsDokument31 SeitenIntroduction To Data Analytics: Sampling DistributionspreethiNoch keine Bewertungen
- Health Benefits of Tea Drinking: Camellia Sinensis "Tea sutra:Cha-Kyou" Written by Lu Yu inDokument6 SeitenHealth Benefits of Tea Drinking: Camellia Sinensis "Tea sutra:Cha-Kyou" Written by Lu Yu inDan George IIINoch keine Bewertungen
- Lipid MetabolismDokument38 SeitenLipid Metabolismraul sinatoNoch keine Bewertungen
- Keywords:-Effervescent Granules Beetroot Carrots : Apples CholesterolDokument5 SeitenKeywords:-Effervescent Granules Beetroot Carrots : Apples CholesterolInternational Journal of Innovative Science and Research TechnologyNoch keine Bewertungen
- Diagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newDokument94 SeitenDiagnostic Biochemistry. (Ms 1st &2nd Sem.3rd Year) Part-3newmatrix_oriNoch keine Bewertungen
- Clinical Chemistry 1: Lipids and Lipoprotein - Methods in TestingDokument5 SeitenClinical Chemistry 1: Lipids and Lipoprotein - Methods in TestingBRYAN M. MOLDENoch keine Bewertungen
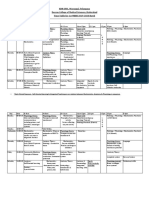
- KNRUHS 1st MBBS Time Table 2019-2020 DCMS - CumulativeDokument42 SeitenKNRUHS 1st MBBS Time Table 2019-2020 DCMS - CumulativeAnime FanNoch keine Bewertungen
- Cover Page MergedDokument98 SeitenCover Page MergedAmos OngNoch keine Bewertungen
- The National Kidney and Transplant Institute DietDokument8 SeitenThe National Kidney and Transplant Institute DietLucyellowOttemoesoeNoch keine Bewertungen
- Rit ReportDokument4 SeitenRit Reportadarshranjansingh1903Noch keine Bewertungen
- Aqa Bly1h QP Jan12Dokument12 SeitenAqa Bly1h QP Jan12ApplemeisterNoch keine Bewertungen
- Short EssayDokument13 SeitenShort EssayYazhiniNoch keine Bewertungen
- Cholesterol JChemEdDokument2 SeitenCholesterol JChemEdchyvNoch keine Bewertungen
- Farmakognosi Steroid PDFDokument14 SeitenFarmakognosi Steroid PDFjulioNoch keine Bewertungen
- Extract Ethanol Effect of Robusta Coffe Antihyperlipidemia Towards TAG Level On Male Wistar Rat Induced With High Fat DietsDokument31 SeitenExtract Ethanol Effect of Robusta Coffe Antihyperlipidemia Towards TAG Level On Male Wistar Rat Induced With High Fat DietsPbkkel 15Noch keine Bewertungen
- BioavailabilityDokument99 SeitenBioavailabilityChimdesaNoch keine Bewertungen
- FNSC 3002 Practical 1 Determination of Plasma Ldl-Cholesterol Hdl-Cholesterol Triacylglycerol and ApolipoproteinsDokument7 SeitenFNSC 3002 Practical 1 Determination of Plasma Ldl-Cholesterol Hdl-Cholesterol Triacylglycerol and ApolipoproteinsPurple DecibelNoch keine Bewertungen
- Nature Sunshine I-NDokument29 SeitenNature Sunshine I-Napi-244390023Noch keine Bewertungen
- A Concentration of Technology For High Quality Results: Clinical Chemistry SystemDokument2 SeitenA Concentration of Technology For High Quality Results: Clinical Chemistry SystemHabibNoch keine Bewertungen
- CAD, HPN, HyperlipidemiaDokument8 SeitenCAD, HPN, Hyperlipidemiasarguss14100% (2)
- Cholesterol Liquicolor CHOD-PAPDokument1 SeiteCholesterol Liquicolor CHOD-PAPmaarboleda1100% (2)
- Liver PhysiologyDokument46 SeitenLiver PhysiologyMaryNoch keine Bewertungen