Das könnte Ihnen auch gefallen
- Anxiety DisordersDokument34 SeitenAnxiety DisordersGafaranga Jean PierreNoch keine Bewertungen
- Anxiety disorders: types, symptoms, and treatmentDokument8 SeitenAnxiety disorders: types, symptoms, and treatmentShrests SinhaNoch keine Bewertungen
- Anxiety Disorders: Types, Symptoms, and TreatmentsDokument62 SeitenAnxiety Disorders: Types, Symptoms, and TreatmentsPRHSTNoch keine Bewertungen
- Screenshot 2020-01-13 at 2.35.04 PMDokument50 SeitenScreenshot 2020-01-13 at 2.35.04 PMSharifah NabaahaNoch keine Bewertungen
- Anxiety PresDokument17 SeitenAnxiety Preswillson gokuNoch keine Bewertungen
- Anxiety Disorders Lecture NotesDokument9 SeitenAnxiety Disorders Lecture NotesHerme BorladoNoch keine Bewertungen
- Anxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDDokument38 SeitenAnxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDadystiNoch keine Bewertungen
- 02 Anxiety DisordersDokument9 Seiten02 Anxiety DisorderskayalvizhiNoch keine Bewertungen
- C. Disturbi D'ansiaDokument45 SeitenC. Disturbi D'ansiailariaNoch keine Bewertungen
- Anxiety DisordersDokument39 SeitenAnxiety DisordersAugene ToribioNoch keine Bewertungen
- Anxiety DisordersDokument29 SeitenAnxiety DisordersJince V JohnNoch keine Bewertungen
- Lesson 6 - Anxiety-DisordersDokument74 SeitenLesson 6 - Anxiety-DisordersKristian Dave DivaNoch keine Bewertungen
- Anxiety Disorders: Nagy Ghattas Henein Ass. Lecturer, NeuropsychiatryDokument39 SeitenAnxiety Disorders: Nagy Ghattas Henein Ass. Lecturer, NeuropsychiatryNagy ShenodaNoch keine Bewertungen
- Understanding Anxiety DisordersDokument22 SeitenUnderstanding Anxiety DisordersShubham KumarNoch keine Bewertungen
- Anxiety Disorders FR ClassDokument11 SeitenAnxiety Disorders FR ClassPranali M.Noch keine Bewertungen
- PsychiatryDokument92 SeitenPsychiatrykimNoch keine Bewertungen
- Panic & Bipolar Affective Disorders: Group 1Dokument33 SeitenPanic & Bipolar Affective Disorders: Group 1AYO NELSONNoch keine Bewertungen
- Anxiety DisordersDokument20 SeitenAnxiety DisordersHndrNoch keine Bewertungen
- Anxiety and Depressive Disorders: Understanding the RelationshipDokument73 SeitenAnxiety and Depressive Disorders: Understanding the RelationshipDISKA YUNIAROHIMNoch keine Bewertungen
- Anxiety and StressDokument6 SeitenAnxiety and StressRubilyn SumayloNoch keine Bewertungen
- Anxiolytic & Hypnotic Agents: Presented By: Tocpel, SDokument12 SeitenAnxiolytic & Hypnotic Agents: Presented By: Tocpel, Sreinnard tocpelNoch keine Bewertungen
- AnxietyforSeminar 000Dokument55 SeitenAnxietyforSeminar 000Heka Setyo AriantoNoch keine Bewertungen
- Anxiety Disorders: Types, Causes and TreatmentsDokument61 SeitenAnxiety Disorders: Types, Causes and TreatmentsVeeresh TopalakattiNoch keine Bewertungen
- Psych Ch. 7 Notes (Tutor)Dokument5 SeitenPsych Ch. 7 Notes (Tutor)Haylle ThomasNoch keine Bewertungen
- Anxiety DisorderDokument33 SeitenAnxiety DisorderMahmoud SalehNoch keine Bewertungen
- Lecture 9 - Ch. 15 & 16 Psychological Disorders and TreatmentDokument15 SeitenLecture 9 - Ch. 15 & 16 Psychological Disorders and TreatmentSaad SiddiquiNoch keine Bewertungen
- Anxiolytic and Hypnotic Drugs 2Dokument44 SeitenAnxiolytic and Hypnotic Drugs 2Adeniran CharlesNoch keine Bewertungen
- ReviewerDokument5 SeitenReviewerEvieNoch keine Bewertungen
- Pemicu 6 Blok Saraf & Kejiwaan: Liliani Labitta 405120026Dokument8 SeitenPemicu 6 Blok Saraf & Kejiwaan: Liliani Labitta 405120026Florence StellaNoch keine Bewertungen
- Anxiety Disorders ExplainedDokument3 SeitenAnxiety Disorders ExplainedHaley Vest MustaficNoch keine Bewertungen
- Anxiety DisordersDokument10 SeitenAnxiety Disorderssrashta gargNoch keine Bewertungen
- Class II Neurotic DisordersDokument37 SeitenClass II Neurotic DisordersNarayan K Ghorapde100% (1)
- Anxiety DisordersDokument11 SeitenAnxiety DisordersMahmoud emadNoch keine Bewertungen
- Panic Disorder Diagnosis and Treatment OptionsDokument3 SeitenPanic Disorder Diagnosis and Treatment OptionsRavi Singh RathoreNoch keine Bewertungen
- Psychiatry 2 - Compilation (Midterm and FinalsDokument14 SeitenPsychiatry 2 - Compilation (Midterm and FinalsRavi Singh RathoreNoch keine Bewertungen
- Anxiety Disorders - Lecture NotesDokument14 SeitenAnxiety Disorders - Lecture NotesPeter Forster67% (3)
- PSYCH101 Lecture 10-11 PsychopathologyDokument80 SeitenPSYCH101 Lecture 10-11 PsychopathologyLucy YengNoch keine Bewertungen
- AP Psychology Module 66+67Dokument5 SeitenAP Psychology Module 66+67kyuuNoch keine Bewertungen
- Anxiety Disorders ExplainedDokument32 SeitenAnxiety Disorders ExplainedPedrosa NardNoch keine Bewertungen
- PMH Panic disorder pptDokument19 SeitenPMH Panic disorder pptycq5s9jdgnNoch keine Bewertungen
- Neurotic DisordersDokument59 SeitenNeurotic DisordersCristy-Esther DocdocNoch keine Bewertungen
- Anxiety Disorders-Batch 17 Srik-Sept 2012Dokument57 SeitenAnxiety Disorders-Batch 17 Srik-Sept 2012Sangkaran KumarNoch keine Bewertungen
- 3-Anxiety DisordersDokument57 Seiten3-Anxiety DisordersVidya BalaNoch keine Bewertungen
- Neurotic, Stress-Related DisordersDokument5 SeitenNeurotic, Stress-Related Disordersvarsha thakurNoch keine Bewertungen
- Anxiety DisordersDokument49 SeitenAnxiety DisordersMeena ViswaNoch keine Bewertungen
- Midterms Abno1Dokument22 SeitenMidterms Abno1Allana Ruth P. AbudaNoch keine Bewertungen
- Abnormal Psychology Midterm NotesDokument22 SeitenAbnormal Psychology Midterm NotesAllana Ruth P. AbudaNoch keine Bewertungen
- Anxiety Disorders in The Elderly Anxiety Disorders in The ElderlyDokument6 SeitenAnxiety Disorders in The Elderly Anxiety Disorders in The ElderlylolimelatinaNoch keine Bewertungen
- Molecular Basis of Anxiety DisordersDokument36 SeitenMolecular Basis of Anxiety DisordersRina WidarsihNoch keine Bewertungen
- Abnormal Psychology (Chapter 4)Dokument9 SeitenAbnormal Psychology (Chapter 4)Mavy QueenNoch keine Bewertungen
- Major Depression GuideDokument8 SeitenMajor Depression GuideLoren SangalangNoch keine Bewertungen
- Mood Disorders ExplainedDokument11 SeitenMood Disorders ExplainedPrincessXFaithNoch keine Bewertungen
- Schillo - L-Exam Two Study GuideDokument14 SeitenSchillo - L-Exam Two Study GuideLiz Schillo100% (1)
- Schillo - L-Exam Two Study GuideDokument19 SeitenSchillo - L-Exam Two Study GuideLiz SchilloNoch keine Bewertungen
- Anxiety Disorders Intro2Dokument18 SeitenAnxiety Disorders Intro2Noelle Grace Ulep BaromanNoch keine Bewertungen
- Biopsychology of Psychiatric DisordersDokument12 SeitenBiopsychology of Psychiatric DisordersGrace VillanuevaNoch keine Bewertungen
- Psychiatry Passmedicine & Onexamination Notes 2016 PDFDokument34 SeitenPsychiatry Passmedicine & Onexamination Notes 2016 PDFJyothi ReddyNoch keine Bewertungen
- Neurotic, Stress-Related and Somatoform Disorders: By: Dr. Nyoman Ratep, SPKJ (K)Dokument26 SeitenNeurotic, Stress-Related and Somatoform Disorders: By: Dr. Nyoman Ratep, SPKJ (K)widyaNoch keine Bewertungen
- Calm and Centered: Overcoming Anxiety and Panic Attacks NaturallyVon EverandCalm and Centered: Overcoming Anxiety and Panic Attacks NaturallyNoch keine Bewertungen
- DOH Nurse Deployment Project 2014 Application FormDokument1 SeiteDOH Nurse Deployment Project 2014 Application FormjamieboyRNNoch keine Bewertungen
- DOH Nurse Deployment Project 2014 Application FormDokument1 SeiteDOH Nurse Deployment Project 2014 Application FormjamieboyRNNoch keine Bewertungen
- Child CareDokument21 SeitenChild CareDexter FloresNoch keine Bewertungen
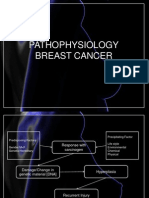
- Breast Cancer Patho MAcDokument5 SeitenBreast Cancer Patho MAcDexter FloresNoch keine Bewertungen
- Dating & CourtshipdasDokument7 SeitenDating & CourtshipdasDexter FloresNoch keine Bewertungen
- Handwashing Activity 1Dokument6 SeitenHandwashing Activity 1Rodel AgapitoNoch keine Bewertungen
- ReadingsDokument4 SeitenReadingsDexter FloresNoch keine Bewertungen
- Rds Patho (Dexsdad)Dokument9 SeitenRds Patho (Dexsdad)Dexter FloresNoch keine Bewertungen
- Schizophrenia NCMH Case StudyDokument41 SeitenSchizophrenia NCMH Case StudyJohn Crisostomo89% (36)
- Winona Ryder Overdose AspirinDokument4 SeitenWinona Ryder Overdose AspirinDexter FloresNoch keine Bewertungen
- Mac Documentaries in Health and HygieneDokument41 SeitenMac Documentaries in Health and HygieneDexter FloresNoch keine Bewertungen
- SyphiliskgkhgkjlhDokument94 SeitenSyphiliskgkhgkjlhDexter FloresNoch keine Bewertungen
- "I Have Neither Given Nor Received Unauthorized Assistance On This Activity." - Student's SignatureDokument1 Seite"I Have Neither Given Nor Received Unauthorized Assistance On This Activity." - Student's SignatureDexter FloresNoch keine Bewertungen
- Pott’s Disease: A Concise OverviewDokument54 SeitenPott’s Disease: A Concise OverviewDexter Flores100% (1)
- Nursing Care Plan for Neonatal JaundiceDokument8 SeitenNursing Care Plan for Neonatal JaundiceDexter FloresNoch keine Bewertungen
- Final Na!!!!!!!Dokument26 SeitenFinal Na!!!!!!!Dexter FloresNoch keine Bewertungen
- Front PAgeDokument2 SeitenFront PAgeDexter FloresNoch keine Bewertungen
- A Child This Day Is BornDokument8 SeitenA Child This Day Is BornDexter FloresNoch keine Bewertungen
- UnpaidDokument2 SeitenUnpaidDexter FloresNoch keine Bewertungen
- Ninety SeventiesDokument6 SeitenNinety Seventiesmuhammad talhaNoch keine Bewertungen
- Indian JudiciaryDokument6 SeitenIndian JudiciaryAdiba A. 130Noch keine Bewertungen
- Department of History Presidency University Post Graduate SyllabusDokument64 SeitenDepartment of History Presidency University Post Graduate SyllabusANUJ BISWASNoch keine Bewertungen
- Introduction to the Legal Environment of BusinessDokument13 SeitenIntroduction to the Legal Environment of BusinessanantarajkhanalNoch keine Bewertungen
- Assignment - Reflection of Movie Kramer Vs KramerDokument2 SeitenAssignment - Reflection of Movie Kramer Vs Krameryannie11Noch keine Bewertungen
- 02 - DNVs Hull STR For WW - Naming of StructureDokument27 Seiten02 - DNVs Hull STR For WW - Naming of StructureArpit GoyalNoch keine Bewertungen
- Saga v2 - Getting Started With Mutatawwi'aDokument4 SeitenSaga v2 - Getting Started With Mutatawwi'abaneblade1Noch keine Bewertungen
- Contemporary Global GovernanceDokument28 SeitenContemporary Global GovernanceMa. Angelika MejiaNoch keine Bewertungen
- Ronald Francis Smart v. William D. Leeke, Commissioner, South Carolina Department of Corrections Attorney General of South Carolina, 917 F.2d 1302, 4th Cir. (1990)Dokument3 SeitenRonald Francis Smart v. William D. Leeke, Commissioner, South Carolina Department of Corrections Attorney General of South Carolina, 917 F.2d 1302, 4th Cir. (1990)Scribd Government DocsNoch keine Bewertungen
- 18 2023 6 39 14 AmDokument5 Seiten18 2023 6 39 14 AmIsa Yahya BayeroNoch keine Bewertungen
- Defense Statement of Tajalli Wa-Ru'yaDokument6 SeitenDefense Statement of Tajalli Wa-Ru'yaStaceMitchellNoch keine Bewertungen
- ISD International All Country Dialing Calling Codes Free Online List Database Download CSV PDFDokument15 SeitenISD International All Country Dialing Calling Codes Free Online List Database Download CSV PDFnss1234567890Noch keine Bewertungen
- North KoreaDokument2 SeitenNorth KoreamichaelmnbNoch keine Bewertungen
- Intermediate GW 12aDokument2 SeitenIntermediate GW 12aKarol Nicole Huanca SanchoNoch keine Bewertungen
- Amendment of Crime from Homicide to Murder UpheldDokument3 SeitenAmendment of Crime from Homicide to Murder UpheldBananaNoch keine Bewertungen
- Aermacchi M 346FTDokument2 SeitenAermacchi M 346FTRUBADUR100% (1)
- SantanderDokument1 SeiteSantanderKabanNoch keine Bewertungen
- Thayer Strategic Implications of President Biden's Visit To VietnamDokument3 SeitenThayer Strategic Implications of President Biden's Visit To VietnamCarlyle Alan Thayer100% (1)
- 1) German UnificationDokument7 Seiten1) German UnificationKaiwen XueNoch keine Bewertungen
- Jurisdiction of Juvenile Courts vs Regular CourtsDokument3 SeitenJurisdiction of Juvenile Courts vs Regular CourtsMeg GutierrezNoch keine Bewertungen
- DEPED Grievance Machinery GuideDokument6 SeitenDEPED Grievance Machinery Guideanita boholNoch keine Bewertungen
- U.S.A. V DARREN HUFF (ED TN) - 119 - MOTION in Limine To Require The GovernmentDokument6 SeitenU.S.A. V DARREN HUFF (ED TN) - 119 - MOTION in Limine To Require The GovernmentJack RyanNoch keine Bewertungen
- Sofitel Montreal Hotel and Resorts AgreementDokument3 SeitenSofitel Montreal Hotel and Resorts AgreementJoyce ReisNoch keine Bewertungen
- Lorie Smith v. Aubrey Elenis, Et Al.: Appeal NoticeDokument3 SeitenLorie Smith v. Aubrey Elenis, Et Al.: Appeal NoticeMichael_Lee_RobertsNoch keine Bewertungen
- FULE vs. CADokument6 SeitenFULE vs. CAlucky javellanaNoch keine Bewertungen
- DGST Benguet V KeppelDokument1 SeiteDGST Benguet V KeppelJan-Lawrence Olaco100% (2)
- Chapter 11 Path To Modernization - HssliveDokument7 SeitenChapter 11 Path To Modernization - Hssliveanujdubey0183% (6)
- Case Digests in Special Proceedings Rules 72 100 Atty. Yulo Sunday 3 5PM As of 28 Feb 2019Dokument37 SeitenCase Digests in Special Proceedings Rules 72 100 Atty. Yulo Sunday 3 5PM As of 28 Feb 2019Ivan Lee100% (1)
- Puncia vs. Toyota dismissal case analysisDokument7 SeitenPuncia vs. Toyota dismissal case analysisKimberly RamosNoch keine Bewertungen
- Full Text of Supreme Court Judgement in Ayodhya Land Dispute CaseDokument1.045 SeitenFull Text of Supreme Court Judgement in Ayodhya Land Dispute CaseNDTV96% (26)